A Patient with Plaque Type Morphea Mimicking Systemic Lupus Erythematosus
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Interstitial Granuloma Annulare Triggered by Lyme Disease
Volume 27 Number 5| May 2021 Dermatology Online Journal || Case Presentation 27(5):11 Interstitial granuloma annulare triggered by Lyme disease Jordan Hyde1 MD, Jose A Plaza1,2 MD, Jessica Kaffenberger1 MD Affiliations: 1Division of Dermatology, The Ohio State University Wexner Medical Center, Columbus, Ohio, USA, 2Department of Pathology, The Ohio State University Wexner Medical Center, Columbus, Ohio, USA Corresponding Author: Jessica Kaffenberger MD, Division of Dermatology, The Ohio State University Medical Wexner Medical Center, Suite 240, 540 Officenter Place, Columbus, OH 43230, Tel: 614-293-1707, Email: [email protected] been associated with a variety of systemic diseases Abstract including diabetes mellitus, malignancy, thyroid Granuloma annulare is a non-infectious disease, dyslipidemia, and infection [3,4]. granulomatous skin condition with multiple different associations. We present a case of a man in his 60s There are multiple histological variants of GA, with a three-week history of progressive targetoid including interstitial GA. The histopathology of plaques on his arms, legs, and trunk. Skin biopsy classic GA demonstrates a focal degeneration of demonstrated interstitial granuloma annulare. collagen surrounded by an inflammatory infiltrate Additional testing revealed IgM antibodies to Borrelia composed of lymphocytes and histiocytes. In a less burgdorferi on western blot suggesting interstitial common variant, interstitial GA, scattered histiocytes granuloma annulare was precipitated by the recent are seen -

2017 Oregon Dental Conference® Course Handout
2017 Oregon Dental Conference® Course Handout Nasser Said-Al-Naief, DDS, MS Course 8125: “The Mouth as The Body’s Mirror: Oral, Maxillofacial, and Head and Neck Manifestations of Systemic Disease” Thursday, April 6 2 pm - 3:30 pm 2/28/2017 The Mouth as The Body’s Mirror Oral Maxillofacial and Head and Neck Manifestation of Ulcerative Conditions of Allergic & Immunological Systemic Disease the Oro-Maxillofacial Diseases Region Nasser Said-Al-Naief, DDS, MS Professor & Chair, Oral Pathology and Radiology Director, OMFP Laboratory Oral manifestations of Office 503-494-8904// Direct: 503-494-0041 systemic diseases Oral Manifestations of Fax: 503-494-8905 Dermatological Diseases Cell: 1-205-215-5699 Common Oral [email protected] Conditions [email protected] OHSU School of Dentistry OHSU School of Medicine 2730 SW Moody Ave, CLSB 5N008 Portland, Oregon 97201 Recurrent aphthous stomatitis (RAS) Recurrent aphthous stomatitis (RAS) • Aphthous" comes from the Greek word "aphtha”- • Recurrence of one or more painful oral ulcers, in periods of days months. = ulcer • Usually begins in childhood or adolescence, • The most common oral mucosal disease in North • May decrease in frequency and severity by age America. (30+). • Affect 5% to 66% of the North American • Ulcers are confined to the lining (non-keratinized) population. mucosa: • * 60% of those affected are members of the • Buccal/labial mucosa, lateral/ventral tongue/floor of professional class. the mouth, soft palate/oropharyngeal mucosa • Etiopathogenesis: 1 2/28/2017 Etiology of RAU Recurrent Aphthous Stomatitis (RAS): Types: Minor; small size, shallow, regular, preceeded by prodrome, heal in 7-10 days Bacteria ( S. -

Case Report an Exophytic and Symptomatic Lesion of the Labial Mucosa Diagnosed As Labial Seborrheic Keratosis
Int J Clin Exp Pathol 2019;12(7):2749-2752 www.ijcep.com /ISSN:1936-2625/IJCEP0093949 Case Report An exophytic and symptomatic lesion of the labial mucosa diagnosed as labial seborrheic keratosis Hui Feng1,2, Binjie Liu1, Zhigang Yao1, Xin Zeng2, Qianming Chen2 1XiangYa Stomatological Hospital, Central South University, Changsha 410000, Hunan, P. R. China; 2State Key Laboratory of Oral Diseases, West China Hospital of Stomatology, Sichuan University, Chengdu 610041, Sichuan, P. R. China Received March 16, 2019; Accepted April 23, 2019; Epub July 1, 2019; Published July 15, 2019 Abstract: Seborrheic keratosis is a common benign epidermal tumor that occurs mainly in the skin of the face and neck, trunk. The tumors are not, however, seen on the oral mucous membrane. Herein, we describe a case of labial seborrheic keratosis confirmed by histopathology. A healthy 63-year-old man was referred to our hospital for evalu- ation and treatment of a 2-month history of a labial mass with mild pain. Clinically, the initial impressions were ma- lignant transformation of chronic discoid lupus erythematosus, syphilitic chancre, or keratoacanthoma. Surprisingly, our laboratory results and histopathologic evaluations established a novel diagnosis of a hyperkeratotic type of labial seborrheic keratosis (SK). This reminds us that atypical or varying features of seborrheic keratosis make it difficult to provide an accurate diagnosis. Clinical manifestations of some benign lesions may be misdiagnosed as malignancy. Consequently, dentists should consider this as a differential diagnosis in labial or other oral lesions. Keywords: Seborrheic keratosis, exophytic lesion, symptomatic lesion, labial mucosa, oral mucous membrane Introduction findings were revealed in his medical history, and he had no known allergies to foods or me- Seborrheic keratosis is a common benign epi- dications. -

Systemic Lupus Erythematosus and Granulomatous Lymphadenopathy
Shrestha et al. BMC Pediatrics 2013, 13:179 http://www.biomedcentral.com/1471-2431/13/179 CASE REPORT Open Access Systemic lupus erythematosus and granulomatous lymphadenopathy Devendra Shrestha1*, Ajaya Kumar Dhakal1, Shiva Raj KC2, Arati Shakya1, Subhash Chandra Shah1 and Henish Shakya1 Abstract Background: Systemic lupus erythematosus (SLE) is known to present with a wide variety of clinical manifestations. Lymphadenopathy is frequently observed in children with SLE and may occasionally be the presenting feature. SLE presenting with granulomatous changes in lymph node biopsy is rare. These features may also cause diagnostic confusion with other causes of granulomatous lymphadenopathy. Case presentation: We report 12 year-old female who presented with generalized lymphadenopathy associated with intermittent fever as well as weight loss for three years. She also had developed anasarca two years prior to presentation. On presentation, she had growth failure and delayed puberty. Lymph node biopsy revealed granulomatous features. She developed a malar rash, arthritis and positive ANA antibodies over the course of next two months and showed WHO class II lupus nephritis on renal biopsy, which confirmed the final diagnosis of SLE. She was started on oral prednisolone and hydroxychloroquine with which her clinical condition improved, and she is currently much better under regular follow up. Conclusion: Generalized lymphadenopathy may be the presenting feature of SLE and it may preceed the other symptoms of SLE by many years as illustrated by this patient. Granulomatous changes may rarely be seen in lupus lymphadenitis. Although uncommon, in children who present with generalized lymphadenopathy along with prolonged fever and constitutional symptoms, non-infectious causes like SLE should also be considered as a diagnostic possibility. -
Nodular Morphea
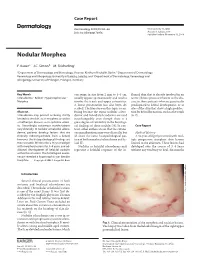
Case Report Dermatology 2009;218:63–66 Received: July 13, 2008 DOI: 10.1159/000173976 Accepted: July 23, 2008 Published online: November 13, 2008 Nodular Morphea a b c F. Kauer J.C. Simon M. Sticherling a b Department of Dermatology and Venerology, Vivantes Klinikum Neukölln, Berlin , Department of Dermatology, c Venerology and Allergology, University of Leipzig, Leipzig , and Department of Dermatology, Venerology and Allergology, University of Erlangen, Erlangen , Germany Key Words can range in size from 2 mm to 4–5 cm, flamed skin that is already involved in an -Scleroderma ؒ Keloid ؒ Hypertrophic scar ؒ usually appear spontaneously and tend to active fibrotic process inherent to the dis Morphea involve the trunk and upper extremities. ease in those patients who are genetically A linear presentation has also been de- predisposed to keloid development, or at scribed. The literature on this topic is con- sites of the skin that show a high predilec- Abstract fusing because the terms ‘nodular sclero- tion for keloid formation, such as the trunk Scleroderma may present as being strictly derma’ and ‘keloidal scleroderma’ are used [6, 7] . limited to the skin, as in morphea, or within interchangeably even though there is a a multiorgan disease, as in systemic sclero- great degree of variability in the histologi- sis. Accordingly, cutaneous manifestations cal findings of these nodules [4] . In con- C a s e R e p o r t vary clinically. In nodular or keloidal sclero- trast, other authors stress that the cutane- derma, patients develop lesions that are ous manifestations may vary clinically, but Medical History clinically indistinguishable from a keloid; all share the same histopathological pat- A 16-year-old girl presented with mul- however, the histopathological findings are tern of both morphea/scleroderma and ke- tiple progressive morpheic skin lesions more variable. -

Tumid Lupus Erythematosus
Tumid Lupus Erythematosus Sylvia Hsu, MD; Linda Y. Hwang, MD; Hiram Ruiz, MD Tumid lupus erythematosus (TLE) is a variant of cutaneous lupus erythematosus. Most patients who present with these skin lesions are young women. The condition clinically resembles polymorphous light eruption, systemic lupus ery- thematosus (SLE), reticulated erythematous mucinosis, or gyrate erythema. Histopathologi- cally, the lesions resemble classic lupus erythem- atosus because of their superficial and deep lymphohistiocytic inflammatory infiltrates and dermal mucin. However, unlike classic lupus ery- thematosus, there is little or no epidermal or dermo-epidermal involvement. Antinuclear anti- body test results are usually negative. We describe 4 cases of TLE and discuss the differ- ential diagnosis. here have been few reports of tumid lupus erythematosus (TLE) in the literature.1-4 T Most major textbooks of dermatology or Figure 1. Erythematous papules and plaques on the dermatopathology mention this entity only briefly, chest of patient 1. if at all. Ackerman et al5 consider TLE to be a manifestation of discoid lupus erythematosus (DLE). We describe 4 patients with TLE and review the her chest, upper extremities, and face (Figure 1). list of controversial entities that overlap clinically Test results for antinuclear antibodies (ANA), Ro, and histologically with TLE. La, and dsDNA were all negative. Histopathology results revealed superficial and deep perivascular Case Reports and periadnexal lymphohistiocytic infiltrates with Patient 1—A 34-year-old white woman presented dermal mucin. There was no involvement of the with an 8-year history of asymptomatic lesions on epidermis, the dermo-epidermal junction, or the her face, neck, chest, and upper extremities. -

Clinical Spectrum of Lyme Disease
European Journal of Clinical Microbiology & Infectious Diseases (2019) 38:201–208 https://doi.org/10.1007/s10096-018-3417-1 REVIEW Clinical spectrum of Lyme disease Jesus Alberto Cardenas-de la Garza1 & Estephania De la Cruz-Valadez1 & Jorge Ocampo-Candiani 1 & Oliverio Welsh1 Received: 4 September 2018 /Accepted: 30 October 2018 /Published online: 19 November 2018 # Springer-Verlag GmbH Germany, part of Springer Nature 2018 Abstract Lyme disease (borreliosis) is one of the most common vector-borne diseases worldwide. Its incidence and geographic expansion has been steadily increasing in the last decades. Lyme disease is caused by Borrelia burgdorferi sensu lato, a heterogeneous group of which three genospecies have been systematically associated to Lyme disease: B. burgdorferi sensu stricto Borrelia afzelii and Borrelia garinii. Geographical distribution and clinical manifestations vary according to the species involved. Lyme disease clinical manifestations may be divided into three stages. Early localized stage is characterized by erythema migrans in the tick bite site. Early disseminated stage may present multiple erythema migrans lesions, borrelial lymphocytoma, lyme neuroborreliosis, carditis, or arthritis. The late disseminated stage manifests with acordermatitis chronica atrophicans, lyme arthritis, and neurological symptoms. Diagnosis is challenging due to the varied clinical manifestations it may present and usually involves a two-step serological approach. In the current review, we present a thorough revision of the clinical manifestations Lyme disease may present. Additionally, history, microbiology, diagnosis, post-treatment Lyme disease syndrome, treatment, and prognosis are discussed. Keywords Lyme disease . Borrelia burgdorferi . Tick-borne diseases . Ixodes . Erythema migrans . Lyme neuroborreliosis History posteriorly meningitis, establishing a link between both mani- festations. -

Systemic Lupus Erythematosus
Systemic Lupus Erythematosus potential side effects, so their use should be monitored by your ABOUT THE DIAGNOSIS veterinarian. If your pet does not tolerate corticosteroid therapy or if Systemic lupus erythematosus (SLE, “lupus”) is an autoimmune the disease is severe, other types of immunosuppressive therapy is disease that can affect multiple body systems. Normally, the immune indicated. This allows lower dosages of corticosteroids and control system attacks germs or foreign substances that invade the body. of severe or persistent symptoms. Azathioprine is most often used Autoimmune diseases occur when the immune system mistakenly in dogs; chlorambucil is frequently chosen for cats. After your pet’s attacks parts of the body. In SLE, multiple body tissues are targeted disease is controlled and the symptoms are reduced or resolved, by the immune system. Susceptibility to developing SLE appears to the dosage of the drugs used will be gradually tapered to the be genetically determined, but environmental factors seem to trigger lowest effective level. the onset of the disease. Some medications can trigger a disease similar to SLE. The role of environmental factors in the development DOs of SLE remains under investigation. Overall, the features of SLE are • Realize that no single test is conclusive for lupus and that the very similar, and sometimes identical, to lupus in humans. diagnosis requires several diagnostic tests for confirmation. Symptoms can be extremely variable, and SLE is sometimes • Keep your pet from excessive exposure to sunlight if he or she referred to as “the great impostor” because of the wide spectrum has SLE, since ultraviolet radiation may make the condition of symptoms it may cause. -

S2 Table. List of Syntax for 96 Diseases
S2 Table. List of syntax for 96 diseases 'autoimmune gastritis'/exp OR 'acantholysis'/exp OR 'acantholysis' OR 'acute disseminated encephalomyelitis'/exp OR 'adem (acute disseminated encephalomyelitis)' OR 'acute disseminated encephalitis' OR 'acute disseminated encephalomyelitis' OR 'encephalitis postvaccinalis' OR 'encephalitis, post-vaccinal' OR 'encephalomyelitis, acute disseminated' OR 'post vaccinal encephalitis' OR 'post vaccination encephalitis' OR 'post-infectious encephalitis' OR 'post-infectious encephalomyelitis' OR 'postinfection encephalitis' OR 'postinfectious encephalitis' OR 'postinfectious encephalomyelitis' OR 'postvaccinal encephalitis' OR 'postvaccinal encephalopathy' OR 'postvaccination encephalitis' OR 'postvaccine encephalitis' OR 'postvaccinial encephalitis' OR 'postvaccinial encephalomyelitis' OR 'smallpox vaccination encephalitis' OR 'vaccinal encephalitis' OR 'vaccination encephalopathy' OR 'vaccination post vaccinial encephalitis' OR 'vaccinia encephalitis' OR 'addison disease'/exp OR 'addison disease' OR 'addison`s disease' OR 'addisons disease' OR 'addison biermer disease' OR 'adult onset still disease'/exp OR 'adult onset still disease' OR 'still`s disease, adult- onset' OR 'allergic glomerulonephritis'/exp OR 'allergic glomerulonephritis' OR 'glomerulonephritis, allergic' OR 'glomerulonephritis, poststreptococcal' OR 'post streptococcal glomerulonephritis' OR 'poststreptococcal glomerulonephritis' OR 'anca associated vasculitis'/exp OR 'anca associated vasculitis' OR 'anca vasculitis' OR 'anca-associated -

Distinct Autoimmune Syndromes in Morphea a Review of 245 Adult and Pediatric Cases
STUDY Distinct Autoimmune Syndromes in Morphea A Review of 245 Adult and Pediatric Cases Justin J. Leitenberger, BS; Rachael L. Cayce, BS; Robert W. Haley, MD; Beverley Adams-Huet, MS; Paul R. Bergstresser, MD; Heidi T. Jacobe, MD Objective: To determine the prevalence of extracuta- fected less frequently than expected. The prevalence of neous manifestations and autoimmunity in adult and pe- concomitant autoimmunity in the generalized subtype diatric patients with morphea. of morphea was statistically significantly greater than that found in all other subtypes combined (P=.01). Fre- Design: A retrospective review of 245 patients with quency of a family history of autoimmune disease showed morphea. a trend in favor of generalized and mixed subgroups. The linear subtype showed a significant association with neu- Setting: University of Texas Southwestern Medical Cen- rologic manifestations, while general systemic manifes- ter–affiliated institutions. tations were most common in the generalized subtype. Antinuclear antibody positivity was most frequent in Patients: Patients with clinical findings consistent with mixed and generalized subtypes. morphea. Conclusions: High prevalences of concomitant and fa- Main Outcome Measures: Prevalence of concomi- tant autoimmune diseases, prevalence of familial auto- milial autoimmune disease, systemic manifestations, and immune disease, prevalence of extracutaneous manifes- antinuclear antibody positivity in the generalized and pos- tations, and laboratory evidence of autoimmunity sibly mixed subtypes suggest that these are systemic au- (antinuclear antibody positivity). Secondary outcome toimmune syndromes and not skin-only phenomena. This measures included demographic features. has implications for the management and treatment of patients with morphea. Results: In this group, adults and children were af- fected nearly equally, and African Americans were af- Arch Dermatol. -

A Rare Case of Systemic Lupus Erythematosus with Subacute Cutaneous Lupus Erythematosus and Morphea
A RARE CASE OF SYSTEMIC LUPUS ERYTHEMATOSUS WITH SUBACUTE CUTANEOUS LUPUS ERYTHEMATOSUS AND MORPHEA Oleh: Satya Wydya Yenny lsramiharti Gardenia Akhyar Puridelko Kampar Yenita Najirman 3.0th lnternational Congress On Autoimmunity Leipzig Germani,6-10 APRIL 2016 BAGIAN ILMU KESEHATAN KULIT DAN KELAMIN FAKULTAS KEDIKTERAN UNIVERSITAS ANDALAS PADANG A RARE CASE OF SYSTEMIC LUPUS ERYTHEMATOSUS WITH SUBACUTE CUTANEOUS LUPUS ERYTHEMATOSUS AND MORPHEA Satya Wydya Yenny, Isramiharti, Gardenia Akhyar, Puridelko Kampar, Yenita*, Najinlan** Demrato-Venereoli:gy Department, A-natomical Pathology Departmentx, Internal Medicine Deparlment** Dr. M. Djamil Hospital/Medical Faculty of Andalas University. Padang West Sumatera. Indonesia ABSTRACT Background: Systemic lupus erythematosus (SLE) is a multisystem disease caused by production and deposition of imn:une-conrpiex resulting in tissue dan.rage. Subacute cutaneons lupus ery'thematosus (SCLE) is part of cutaneus lupus ery.thematosus. Morphea (localized sclerodema) is a fibrosing clisorder of the skin and subcutaneous tissues. Systemic lupus er1'thematosus with SCLE type and morphea in the same patient is a rare case and the incidence retnains unknown, but there were six cases have been reported. Defect of apoptosis regulation suggested play a role in both of these autoimmune diseases. Case report: Reporled a case of SLE with SCLE type and morphea in a 17-year-old {'emale. There was history of hard palpable red-brownish patches on both of cheeks, right nasolabial tbld. under both eyes, both legs, both antts, back, and scalp since Tmonths ago. Patient easily feeis tired, complaining of joint pain, hair easy to tbll, fever, decreased of body weight. Physical examination: hair pull test (+). There were hard palpabie atrophic scars, hyperpigmentation plaques. -

Postvaccination Morphea Profunda in a Child
Brief Reports 525 2. Dobru D, Seuchea N, Dorin M et al. Blue rubber bleb nevus syndrome: case report and literature review. Rom J Gastroenterol 2004;13:237–240. 3. Nahm WK, Moise S, Eichenfield LF et al. Venous malfor- mations in blue rubber bleb nevus syndrome: variable onset of presentation. J Am Acad Dermatol 2004;5(Suppl): S101–S106. 4. Moodley M, Ramdial P. Blue rubber bleb nevus syndrome: case report and review of the literature. Pediatr 1993;92: 160–162. 5. Ertem D, Acar Y, Kotiloglu E et al. Blue rubber bleb nevus syndrome. Pediatr 2001;107:418–420. William Huang, M.D., M.P.H. Arthur Rhodes, M.D., M.P.H. Department of Dermatology, Rush University Medical Center, Chicago, Illinois Address correspondence to William Huang, M.D., M.P.H., Figure 2. H&E section (2·). 1653 West Congress Parkway, 220 Annex Building, Chicago, IL 60612, or e-mail: [email protected]. equally affected. Approximately 150 cases have been reported in the literature. The differential diagnosis Postvaccination Morphea Profunda in a Child includes familial cutaneous and mucosal venous mal- formation syndrome, familial glomangiomatosis, diffuse neonatal hemangiomatosis, and Maffuci syndrome (1). Abstract: We report a new case of postvaccination The most common site of visceral involvement is the morphea profunda (MP) in a child and discuss its dif- gastrointestinal tract, most commonly the small intes- ferent clinical presentations, prognosis, and therapy tine, documented by upper endoscopy, colonoscopy, or and its relationship with ‘‘solitary morphea profunda.’’ magnetic resonance imaging (MRI). Significant compli- A 2-year-old healthy girl presented with an induration of cations of gastrointestinal involvement include gastro- the anterior aspect of the left thigh of 9 months dura- intestinal hemorrhage, intussusception, volvulus, tion.