Interstitial Granuloma Annulare Triggered by Lyme Disease
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2017 Oregon Dental Conference® Course Handout
2017 Oregon Dental Conference® Course Handout Nasser Said-Al-Naief, DDS, MS Course 8125: “The Mouth as The Body’s Mirror: Oral, Maxillofacial, and Head and Neck Manifestations of Systemic Disease” Thursday, April 6 2 pm - 3:30 pm 2/28/2017 The Mouth as The Body’s Mirror Oral Maxillofacial and Head and Neck Manifestation of Ulcerative Conditions of Allergic & Immunological Systemic Disease the Oro-Maxillofacial Diseases Region Nasser Said-Al-Naief, DDS, MS Professor & Chair, Oral Pathology and Radiology Director, OMFP Laboratory Oral manifestations of Office 503-494-8904// Direct: 503-494-0041 systemic diseases Oral Manifestations of Fax: 503-494-8905 Dermatological Diseases Cell: 1-205-215-5699 Common Oral [email protected] Conditions [email protected] OHSU School of Dentistry OHSU School of Medicine 2730 SW Moody Ave, CLSB 5N008 Portland, Oregon 97201 Recurrent aphthous stomatitis (RAS) Recurrent aphthous stomatitis (RAS) • Aphthous" comes from the Greek word "aphtha”- • Recurrence of one or more painful oral ulcers, in periods of days months. = ulcer • Usually begins in childhood or adolescence, • The most common oral mucosal disease in North • May decrease in frequency and severity by age America. (30+). • Affect 5% to 66% of the North American • Ulcers are confined to the lining (non-keratinized) population. mucosa: • * 60% of those affected are members of the • Buccal/labial mucosa, lateral/ventral tongue/floor of professional class. the mouth, soft palate/oropharyngeal mucosa • Etiopathogenesis: 1 2/28/2017 Etiology of RAU Recurrent Aphthous Stomatitis (RAS): Types: Minor; small size, shallow, regular, preceeded by prodrome, heal in 7-10 days Bacteria ( S. -

A Patient with Plaque Type Morphea Mimicking Systemic Lupus Erythematosus
CASE REPORT A Patient With Plaque Type Morphea Mimicking Systemic Lupus Erythematosus Wardhana1, EA Datau2 1 Department of Internal Medicine, Siloam International Hospitals. Karawaci, Indonesia. 2 Department of Internal Medicine, Prof. Dr. RD Kandou General Hospital & Sitti Maryam Islamic Hospital, Manado, North Sulawesi, Indonesia. Correspondence mail: Siloam Hospitals Group’s CEO Office, Siloam Hospital Lippo Village. 5th floor. Jl. Siloam No.6, Karawaci, Indonesia. email: [email protected] ABSTRAK Morfea merupakan penyakit jaringan penyambung yang jarang dengan gambaran utama berupa penebalan dermis tanpa disertai keterlibatan organ dalam. Penyakit ini juga dikenal sebagai bagian dari skleroderma terlokalisir. Berdasarkan gambaran klinis dan kedalaman jaringan yang terlibat, morfea dikelompokkan ke dalam beberapa bentuk dan sekitar dua pertiga orang dewasa dengan morfea mempunyai tipe plak. Produksi kolagen yang berlebihan oleh fibroblast merupakan penyebab kelainan pada morfea dan mekanisme terjadinya aktivitas fibroblast yang berlebihan ini masih belum diketahui, meskipun beberapa mekanisme pernah diajukan. Morfe tipe plak biasanya bersifat ringan dan dapat sembuh dengan sendirinya. Morfea tipe plak yang penampilan klinisnya menyerupai lupus eritematosus sistemik, misalnya meliputi alopesia dan ulkus mukosa di mulut, jarang dijumpai. Sebuah kasus morfea tipe plak pada wanita berusia 20 tahun dibahas. Pasien ini diobati dengan imunosupresan dan antioksidan local maupun sistemik. Kondisi paisen membaik tanpa disertai efek samping yang berarti. Kata kunci: morfea, tipe plak. ABSTRACT Morphea is an uncommon connective tissue disease with the most prominent feature being thickening or fibrosis of the dermal without internal organ involvement. It is also known as a part of localized scleroderma. Based on clinical presentation and depth of tissue involvement, morphea is classified into several forms, and about two thirds of adults with morphea have plaque type. -

Granulomatous Dermatitis As a Postherpetic Isotopic Response in Immunocompromised Patients: a Report of 5 Cases William H
Washington University School of Medicine Digital Commons@Becker Open Access Publications 2018 Granulomatous dermatitis as a postherpetic isotopic response in immunocompromised patients: A report of 5 cases William H. McCoy Washington University School of Medicine in St. Louis Elaine Otchere Washington University School of Medicine in St. Louis Amy C. Musiek Washington University School of Medicine in St. Louis Milan J. Anadkat Washington University School of Medicine in St. Louis Follow this and additional works at: https://digitalcommons.wustl.edu/open_access_pubs Recommended Citation McCoy, William H.; Otchere, Elaine; Musiek, Amy C.; and Anadkat, Milan J., ,"Granulomatous dermatitis as a postherpetic isotopic response in immunocompromised patients: A report of 5 cases." JAAD Case Reports.4,8. 752-760. (2018). https://digitalcommons.wustl.edu/open_access_pubs/7169 This Open Access Publication is brought to you for free and open access by Digital Commons@Becker. It has been accepted for inclusion in Open Access Publications by an authorized administrator of Digital Commons@Becker. For more information, please contact [email protected]. CASE SERIES Granulomatous dermatitis as a postherpetic isotopic response in immunocompromised patients: A report of 5 cases William H. McCoy 4th, MD, PhD,a,b,c Elaine Otchere, BS,a Amy C. Musiek, MD,a,b,c and MilanJ.Anadkat,MDa,b,c Saint Louis, Missouri Key words: Chronic lymphocytic leukemia; granuloma annulare; granulomatous dermatitis; immunocom- promised district; immunodeficiency; immunocompromise; immunosuppression; isotopic response; locus minoris resistentiae; postherpetic isotopic response; Wolf’s isotopic response. INTRODUCTION Abbreviations used: Granulomatous dermatitis (GD) describes disor- ders in which mixed inflammatory infiltrates AML: acute myelogenous leukemia CLL: chronic lymphocytic leukemia composed primarily of histiocytes invade the skin. -
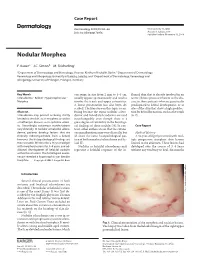
Nodular Morphea
Case Report Dermatology 2009;218:63–66 Received: July 13, 2008 DOI: 10.1159/000173976 Accepted: July 23, 2008 Published online: November 13, 2008 Nodular Morphea a b c F. Kauer J.C. Simon M. Sticherling a b Department of Dermatology and Venerology, Vivantes Klinikum Neukölln, Berlin , Department of Dermatology, c Venerology and Allergology, University of Leipzig, Leipzig , and Department of Dermatology, Venerology and Allergology, University of Erlangen, Erlangen , Germany Key Words can range in size from 2 mm to 4–5 cm, flamed skin that is already involved in an -Scleroderma ؒ Keloid ؒ Hypertrophic scar ؒ usually appear spontaneously and tend to active fibrotic process inherent to the dis Morphea involve the trunk and upper extremities. ease in those patients who are genetically A linear presentation has also been de- predisposed to keloid development, or at scribed. The literature on this topic is con- sites of the skin that show a high predilec- Abstract fusing because the terms ‘nodular sclero- tion for keloid formation, such as the trunk Scleroderma may present as being strictly derma’ and ‘keloidal scleroderma’ are used [6, 7] . limited to the skin, as in morphea, or within interchangeably even though there is a a multiorgan disease, as in systemic sclero- great degree of variability in the histologi- sis. Accordingly, cutaneous manifestations cal findings of these nodules [4] . In con- C a s e R e p o r t vary clinically. In nodular or keloidal sclero- trast, other authors stress that the cutane- derma, patients develop lesions that are ous manifestations may vary clinically, but Medical History clinically indistinguishable from a keloid; all share the same histopathological pat- A 16-year-old girl presented with mul- however, the histopathological findings are tern of both morphea/scleroderma and ke- tiple progressive morpheic skin lesions more variable. -

Treatment Or Removal of Benign Skin Lesions
Treatment or Removal of Benign Skin Lesions Date of Origin: 10/26/2016 Last Review Date: 03/24/2021 Effective Date: 04/01/2021 Dates Reviewed: 10/2016, 10/2017, 10/2018, 04/2019, 10/2019, 01/2020, 03/2020, 03/2021 Developed By: Medical Necessity Criteria Committee I. Description Individuals may acquire a multitude of benign skin lesions over the course of a lifetime. Most benign skin lesions are diagnosed on the basis of clinical appearance and history. If the diagnosis of a lesion is uncertain, or if a lesion has exhibited unexpected changes in appearance or symptoms, a diagnostic procedure (eg, biopsy, excision) is indicated to confirm the diagnosis. The treatment of benign skin lesions consists of destruction or removal by any of a wide variety of techniques. The removal of a skin lesion can range from a simple biopsy, scraping or shaving of the lesion, to a radical excision that may heal on its own, be closed with sutures (stitches) or require reconstructive techniques involving skin grafts or flaps. Laser, cautery or liquid nitrogen may also be used to remove benign skin lesions. When it is uncertain as to whether or not a lesion is cancerous, excision and laboratory (microscopic) examination is usually necessary. II. Criteria: CWQI HCS-0184A Note: **If request is for treatment or removal of warts, medical necessity review is not required** A. Moda Health will cover the treatment and removal of 1 or more of the following benign skin lesions: a. Treatment or removal of actinic keratosis (pre-malignant skin lesions due to sun exposure) is considered medically necessary with 1 or more of the following procedures: i. -

A New Case of Granuloma Annulare
SOCIETY INTELLIGENCE. 307 the first week of life, but that these had cleared off, and that the child had been free until five months ago. The health of the child was and had always been quite good, but recently it had suffered from broken sleep caused by the irritation of the present eruption. The whole of the body and limbs were covered with a very poly- morphous eruption, and on the face there were a few impetiginous scabs. The buttocks showed the typical thumb-nail-sized red papules of Lichen urticatus, and on the thighs and forearms, especially on the extensor surfaces, were the small hard lichenoid papules which are generally seen as the involution-form of this disease. In addition to these lesions, however, were numerous scratch marks whizh, when first seen, showed a tendency to rise into bulls. There were also large blood-stained hulls on the knees and elbows, and the mark of a recent one on the dorsnm of the right foot. There was no factitious urticaria, and the exhibitors had not found any factitious bullous production, though the case had not been watched rmfficiently long for them to be certain on this point. Dr. WHITFIELDsaid that he thought that everyone present would agree with the diagnosis of Lichen urticatus, but the question arose whether there was something else behind it. Epidermolysis bullosa had occurred to him, but although unable to exclude it he thought the history of seven months’ complete freedom from skin-trouble was against it. Dr. COLCOTTFox said that in his opinion the Lichen urticatus was undoubted, and that he would not like to state without watching the case whether this was accompanied by Epidermolysis bullosa or not. -

Lupus Mimickers
Lupus Mimickers Arup Kumar Kundu, Somak Kumar Das INTRODUCTION Systemic lupus erythematosus is considered as “the great mimic of other conditions”. Conversely there are many diseases which can mimic SLE as a systemic disease or as dermatological, rheumatological, vasculitic, or immunological mimickers. This monograph is restricted to the lupus mimickers only, not the discussion on SLE. DERMATOLOGICAL MIMICKERS OF S.L.E. 1,2 I. Dermatological conditions mimicking acute cutaneous lupus erythematosus (LE) Rosacea: Rosacea is characterized by erythema of the central face that has persisted for months or more. The convex areas of the nose, cheeks, chin, and forehead are the characteristic distribution [Fig. 1]. Triggers of rosacea may include hot or cold temperature, sunlight (hence, photosensitive), wind, hot drinks, spicy foods, exercise, emotions, alcohol, cosmetics, topical irritants, menopausal flushing, medications etc. Erythematotelangiectatic subtype and papulopustular subtype may mimic acute cutaneous LE. The malar erythema of lupus erythematosus [Fig. 2] can be difficult to differentiate from rosacea3. The presence of pustules and papules or blepharitis favors a diagnosis Fig.1: Acne Rosacea of rosacea, while fine scaling, pigment change, follicular plugging and scarring favor a diagnosis of lupus. In occasional photodistribution. patients, histologic examination of involved skin may be Chloasma / Melasma: It is combined epidermal and dermal necessary for distinction. hyperpigmentation of forehead, cheeks, and perioral area. It Seborrheic dermatitis: Seborrheic dermatitis of the face is a common problem, almost exclusively limited to women; may closely mimic both early rosacea and the butterfly extremely prevalent in Latin America, among patients with lesions of systemic lupus erythematosus2. In contrast to mixed Indian/Spanish background. -

Necrobiosis Lipoidica with Superimposed Pyoderma Vegetans
CASE REPORT Necrobiosis Lipoidica With Superimposed Pyoderma Vegetans Carl J. Barrick, DO; Omobola Onikoyi, DO; Nektarios I. Lountzis, MD; Tanya Ermolovich, DO; Stephen M. Purcell, DO foul odor was noted in the area underlying the lesion. PRACTICE POINTS Initial punch biopsy demonstrated epidermal hyperplasia • Necrobiosis lipoidica (NL), a chronic granulomatous with neutrophil-rich sinus tracts consistent with pyoderma disease characterized by collagen degeneration, vegetans (PV)(Figure 2A). Tissue culture was positive for granulomatous formation, and endothelial-wall thick- Staphylococcus aureus and Streptococcus anginosus. Cultures ening, is most often seen in association with insulin- for both fungi and acid-fast bacilli were negative for growth. dependent diabetes mellitus (DM). The patient was treated with mupirocin ointment 2% • Asymptomatic, well-circumscribed, violaceous pap- and 3 months of cephalexin 250 mg twice daily, which ules and nodules coalesce into plaques on the lower cleared the purulent crust; however, serous drainage, extremities, face, or trunk in NL. ulceration, and erythemacopy persisted. The patient needed an • Treatment mainstay is topical and intralesional extended course of antibiotics, which had not been previ- corticosteroids at active borders of lesions. Other ously administered to clear the purulence. During this treat- treatments used with some success include tumor ment regimen, the patient’s DM remained uncontrolled. necrosis factor α inhibitors, topical tretinoin, topical tacrolimus, and skin grafting. Control and manage- notA second deeper punch biopsy revealed a layered gran- ment of DM can be helpful. ulomatous infiltrate with sclerosis throughout the dermis most consistent with necrobiosis lipoidica (NL)(Figure 2B). Direct immunofluorescence biopsy was negative. Once the Necrobiosis lipoidica (NL) is a granulomatous inflammatory skin PV was clear, betamethasone dipropionate ointment 0.05% disease strongly associated with diabetes mellitus (DM). -

S2 Table. List of Syntax for 96 Diseases
S2 Table. List of syntax for 96 diseases 'autoimmune gastritis'/exp OR 'acantholysis'/exp OR 'acantholysis' OR 'acute disseminated encephalomyelitis'/exp OR 'adem (acute disseminated encephalomyelitis)' OR 'acute disseminated encephalitis' OR 'acute disseminated encephalomyelitis' OR 'encephalitis postvaccinalis' OR 'encephalitis, post-vaccinal' OR 'encephalomyelitis, acute disseminated' OR 'post vaccinal encephalitis' OR 'post vaccination encephalitis' OR 'post-infectious encephalitis' OR 'post-infectious encephalomyelitis' OR 'postinfection encephalitis' OR 'postinfectious encephalitis' OR 'postinfectious encephalomyelitis' OR 'postvaccinal encephalitis' OR 'postvaccinal encephalopathy' OR 'postvaccination encephalitis' OR 'postvaccine encephalitis' OR 'postvaccinial encephalitis' OR 'postvaccinial encephalomyelitis' OR 'smallpox vaccination encephalitis' OR 'vaccinal encephalitis' OR 'vaccination encephalopathy' OR 'vaccination post vaccinial encephalitis' OR 'vaccinia encephalitis' OR 'addison disease'/exp OR 'addison disease' OR 'addison`s disease' OR 'addisons disease' OR 'addison biermer disease' OR 'adult onset still disease'/exp OR 'adult onset still disease' OR 'still`s disease, adult- onset' OR 'allergic glomerulonephritis'/exp OR 'allergic glomerulonephritis' OR 'glomerulonephritis, allergic' OR 'glomerulonephritis, poststreptococcal' OR 'post streptococcal glomerulonephritis' OR 'poststreptococcal glomerulonephritis' OR 'anca associated vasculitis'/exp OR 'anca associated vasculitis' OR 'anca vasculitis' OR 'anca-associated -

Paradoxical Reactions Under TNF-Α Blocking Agents and Other Biological Agents Given for Chronic Immune- Mediated Diseases: an Analytical and Comprehensive Overview
Treatments RMD Open: first published as 10.1136/rmdopen-2015-000239 on 15 July 2016. Downloaded from REVIEW Paradoxical reactions under TNF-α blocking agents and other biological agents given for chronic immune- mediated diseases: an analytical and comprehensive overview Éric Toussirot,1,2,3,4 François Aubin5,6 To cite: Toussirot É, Aubin F. ABSTRACT Key messages Paradoxical reactions under Paradoxical adverse events (PAEs) have been reported α TNF- blocking agents and during biological treatment for chronic immune- other biological agents given What is already known about this subject? mediated diseases. PAEs are defined as the occurrence for chronic immune-mediated Different paradoxical adverse events have been diseases: an analytical and during biological agent therapy of a pathological described under biological agents, mainly tumour comprehensive overview. condition that usually responds to this class of drug. necrosis factor α inhibitors. RMD Open 2016;2:e000239. A wide range of PAEs have been reported including doi:10.1136/rmdopen-2015- dermatological, intestinal and ophthalmic conditions, What does this study add? 000239 mainly with antitumour necrosis factor α (TNF-α) A wide range of paradoxical adverse events have agents. True PAEs include psoriasis, Crohn’s disease been reported including dermatological, intestinal ▸ Prepublication history for and hidradenitis suppurativa. Other PAEs may be and ophthalmic conditions, but their relationship this paper is available online. qualified as borderline and include uveitis, scleritis, with the biological agent exposition remains still To view these files please sarcoidosis and other granulomatous diseases debated. visit the journal online (granuloma annulare, interstitial granulomatous (http://dx.doi.org/10.1136/ dermatitis), vasculitis, vitiligo and alopecia areata. -

Distinct Autoimmune Syndromes in Morphea a Review of 245 Adult and Pediatric Cases
STUDY Distinct Autoimmune Syndromes in Morphea A Review of 245 Adult and Pediatric Cases Justin J. Leitenberger, BS; Rachael L. Cayce, BS; Robert W. Haley, MD; Beverley Adams-Huet, MS; Paul R. Bergstresser, MD; Heidi T. Jacobe, MD Objective: To determine the prevalence of extracuta- fected less frequently than expected. The prevalence of neous manifestations and autoimmunity in adult and pe- concomitant autoimmunity in the generalized subtype diatric patients with morphea. of morphea was statistically significantly greater than that found in all other subtypes combined (P=.01). Fre- Design: A retrospective review of 245 patients with quency of a family history of autoimmune disease showed morphea. a trend in favor of generalized and mixed subgroups. The linear subtype showed a significant association with neu- Setting: University of Texas Southwestern Medical Cen- rologic manifestations, while general systemic manifes- ter–affiliated institutions. tations were most common in the generalized subtype. Antinuclear antibody positivity was most frequent in Patients: Patients with clinical findings consistent with mixed and generalized subtypes. morphea. Conclusions: High prevalences of concomitant and fa- Main Outcome Measures: Prevalence of concomi- tant autoimmune diseases, prevalence of familial auto- milial autoimmune disease, systemic manifestations, and immune disease, prevalence of extracutaneous manifes- antinuclear antibody positivity in the generalized and pos- tations, and laboratory evidence of autoimmunity sibly mixed subtypes suggest that these are systemic au- (antinuclear antibody positivity). Secondary outcome toimmune syndromes and not skin-only phenomena. This measures included demographic features. has implications for the management and treatment of patients with morphea. Results: In this group, adults and children were af- fected nearly equally, and African Americans were af- Arch Dermatol. -

Orphanet Journal of Rare Diseases Biomed Central
Orphanet Journal of Rare Diseases BioMed Central Review Open Access Sweet's syndrome – a comprehensive review of an acute febrile neutrophilic dermatosis Philip R Cohen*1,2 Address: 1University of Houston Health Center, Houston, Texas, USA and 2The Department of Dermatology, University of Texas-Houston Medical School, Houston, Texas, USA Email: Philip R Cohen* - [email protected] * Corresponding author Published: 26 July 2007 Received: 5 July 2007 Accepted: 26 July 2007 Orphanet Journal of Rare Diseases 2007, 2:34 doi:10.1186/1750-1172-2-34 This article is available from: http://www.OJRD.com/content/2/1/34 © 2007 Cohen; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Abstract Sweet's syndrome (the eponym for acute febrile neutrophilic dermatosis) is characterized by a constellation of clinical symptoms, physical features, and pathologic findings which include fever, neutrophilia, tender erythematous skin lesions (papules, nodules, and plaques), and a diffuse infiltrate consisting predominantly of mature neutrophils that are typically located in the upper dermis. Several hundreds cases of Sweet's syndrome have been published. Sweet's syndrome presents in three clinical settings: classical (or idiopathic), malignancy-associated, and drug-induced. Classical Sweet's syndrome (CSS) usually presents in women between the age of 30 to 50 years, it is often preceded by an upper respiratory tract infection and may be associated with inflammatory bowel disease and pregnancy.