2017 Oregon Dental Conference® Course Handout
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Use of Biologic Agents in the Treatment of Oral Lesions Due to Pemphigus and Behçet's Disease: a Systematic Review
Davis GE, Sarandev G, Vaughan AT, Al-Eryani K, Enciso R. The Use of Biologic Agents in the Treatment of Oral Lesions due to Pemphigus and Behçet’s Disease: A Systematic Review. J Anesthesiol & Pain Therapy. 2020;1(1):14-23 Systematic Review Open Access The Use of Biologic Agents in the Treatment of Oral Lesions due to Pemphigus and Behçet’s Disease: A Systematic Review Gerald E. Davis II1,2, George Sarandev1, Alexander T. Vaughan1, Kamal Al-Eryani3, Reyes Enciso4* 1Advanced graduate, Master of Science Program in Orofacial Pain and Oral Medicine, Herman Ostrow School of Dentistry of USC, Los Angeles, California, USA 2Assistant Dean of Academic Affairs, Assistant Professor, Restorative Dentistry, Meharry Medical College, School of Dentistry, Nashville, Tennessee, USA 3Assistant Professor of Clinical Dentistry, Division of Periodontology, Dental Hygiene & Diagnostic Sciences, Herman Ostrow School of Dentistry of USC, Los Angeles, California, USA 4Associate Professor (Instructional), Division of Dental Public Health and Pediatric Dentistry, Herman Ostrow School of Dentistry of USC, Los Angeles, California, USA Article Info Abstract Article Notes Background: Current treatments for pemphigus and Behçet’s disease, such Received: : March 11, 2019 as corticosteroids, have long-term serious adverse effects. Accepted: : April 29, 2020 Objective: The objective of this systematic review was to evaluate the *Correspondence: efficacy of biologic agents (biopharmaceuticals manufactured via a biological *Dr. Reyes Enciso, Associate Professor (Instructional), Division source) on the treatment of intraoral lesions associated with pemphigus and of Dental Public Health and Pediatric Dentistry, Herman Ostrow Behçet’s disease compared to glucocorticoids or placebo. School of Dentistry of USC, Los Angeles, California, USA; Email: [email protected]. -

Rebamipide to Manage Stomatopyrosis in Oral Submucous Fibrosis 1Joanna Baptist, 2Shrijana Shakya, 3Ravikiran Ongole
JCDP Rebamipide to Manage Stomatopyrosis10.5005/jp-journals-10024-1972 in Oral Submucous Fibrosis ORIGINAL RESEARCH Rebamipide to Manage Stomatopyrosis in Oral Submucous Fibrosis 1Joanna Baptist, 2Shrijana Shakya, 3Ravikiran Ongole ABSTRACT Source of support: Nil Introduction: Oral submucous fibrosis (OSF) causes progres- Conflict of interest: None sive debilitating symptoms, such as oral burning sensation (sto- matopyrosis) and limited mouth opening. The standard of care INTRODUCTION (SOC) protocol includes habit cessation, intralesional steroid and hyaluronidase injections, and mouth opening exercises. The Oral submucous fibrosis (OSF) is commonly seen in objective of the study was to evaluate efficacy of rebamipide the Indian subcontinent affecting individuals of all age in alleviating burning sensation of the oral mucosa in OSF in groups. It is a potentially malignant disorder caused comparison with SOC intralesional steroid injections. almost exclusively by the use of smokeless form of Materials and methods: Twenty OSF patients were divided into tobacco products. The malignant transformation rates two groups [rebamipide (100 mg TID for 21 days) and betametha- vary from 3 to 19%.1,2 sone (4 mg/mL biweekly for 4 weeks)] of 10 each by random Oral submucous fibrosis causes progressive debilitat- sampling. Burning sensation was assessed every week for 1 month. Burning sensation scores were analyzed using repeated ing symptoms affecting the oral cavity, such as burning measures analysis of variance (ANOVA) and paired t-test. sensation, loss of cheek elasticity, restricted tongue move- Results: Change in burning sensation score was significant ments, and limited mouth opening. Oral submucous (p < 0.05) in the first four visits. However, score between the fibrosis is an irreversible condition and the management 4th and 5th visit was not statistically significant (p > 0.05). -
The Neumann Type of Pemphigus Vegetans Treated with Combination of Dapsone and Steroid
YM Son, et al Ann Dermatol Vol. 23, Suppl. 3, 2011 http://dx.doi.org/10.5021/ad.2011.23.S3.S310 CASE REPORT The Neumann Type of Pemphigus Vegetans Treated with Combination of Dapsone and Steroid Young-Min Son, M.D., Hong-Kyu Kang, M.D., Jeong-Hwan Yun, M.D., Joo-Young Roh, M.D., Jong-Rok Lee, M.D. Department of Dermatology, Gachon University of Medicine and Science, Gil Hospital, Incheon, Korea Pemphigus vegetans is a rare variant of pemphigus vulgaris INTRODUCTION and is characterized by vegetating lesions in the inguinal folds and mouth and by the presence of autoantibodies Pemphigus diseases are a group of autoimmune disorders against desmoglein 3. Two clinical subtypes of pemphigus that have certain common features, and these diseases are vegetans exist, which are initially characterized by flaccid considered to be potentially fatal1,2. Pemphigus vegetans bullae and erosions (the Neumann subtype) or pustules (the is a variant of pemphigus vulgaris and is the rarest form of Hallopeau subtype). Both subtypes subsequently develop pemphigus; Pemphigus vegetans comprises less than 1∼ into hyperpigmented vegetative plaques with pustules and 2% of all pemphigus cases1,3,4. This variant is charac- hypertrophic granulation tissue at the periphery of the terized by flaccid bullae or pustules that erode to form hy- lesions. Oral administration of corticosteroids alone does not pertrophic papillated plaques that predominantly involve always induce disease remission in patients with pemphigus the intertriginous areas, the scalp, and the face; in 60∼ vegetans. We report here on a 63-year-old woman with 80% of all cases, the oral mucosa are also affected5,6. -

Interstitial Granuloma Annulare Triggered by Lyme Disease
Volume 27 Number 5| May 2021 Dermatology Online Journal || Case Presentation 27(5):11 Interstitial granuloma annulare triggered by Lyme disease Jordan Hyde1 MD, Jose A Plaza1,2 MD, Jessica Kaffenberger1 MD Affiliations: 1Division of Dermatology, The Ohio State University Wexner Medical Center, Columbus, Ohio, USA, 2Department of Pathology, The Ohio State University Wexner Medical Center, Columbus, Ohio, USA Corresponding Author: Jessica Kaffenberger MD, Division of Dermatology, The Ohio State University Medical Wexner Medical Center, Suite 240, 540 Officenter Place, Columbus, OH 43230, Tel: 614-293-1707, Email: [email protected] been associated with a variety of systemic diseases Abstract including diabetes mellitus, malignancy, thyroid Granuloma annulare is a non-infectious disease, dyslipidemia, and infection [3,4]. granulomatous skin condition with multiple different associations. We present a case of a man in his 60s There are multiple histological variants of GA, with a three-week history of progressive targetoid including interstitial GA. The histopathology of plaques on his arms, legs, and trunk. Skin biopsy classic GA demonstrates a focal degeneration of demonstrated interstitial granuloma annulare. collagen surrounded by an inflammatory infiltrate Additional testing revealed IgM antibodies to Borrelia composed of lymphocytes and histiocytes. In a less burgdorferi on western blot suggesting interstitial common variant, interstitial GA, scattered histiocytes granuloma annulare was precipitated by the recent are seen -

Oral Manifestations of Systemic Disease Their Clinical Practice
ARTICLE Oral manifestations of systemic disease ©corbac40/iStock/Getty Plus Images S. R. Porter,1 V. Mercadente2 and S. Fedele3 provide a succinct review of oral mucosal and salivary gland disorders that may arise as a consequence of systemic disease. While the majority of disorders of the mouth are centred upon the focus of therapy; and/or 3) the dominant cause of a lessening of the direct action of plaque, the oral tissues can be subject to change affected person’s quality of life. The oral features that an oral healthcare or damage as a consequence of disease that predominantly affects provider may witness will often be dependent upon the nature of other body systems. Such oral manifestations of systemic disease their clinical practice. For example, specialists of paediatric dentistry can be highly variable in both frequency and presentation. As and orthodontics are likely to encounter the oral features of patients lifespan increases and medical care becomes ever more complex with congenital disease while those specialties allied to disease of and effective it is likely that the numbers of individuals with adulthood may see manifestations of infectious, immunologically- oral manifestations of systemic disease will continue to rise. mediated or malignant disease. The present article aims to provide This article provides a succinct review of oral manifestations a succinct review of the oral manifestations of systemic disease of of systemic disease. It focuses upon oral mucosal and salivary patients likely to attend oral medicine services. The review will focus gland disorders that may arise as a consequence of systemic upon disorders affecting the oral mucosa and salivary glands – as disease. -

Orofacial Granulomatosis
Al-Hamad, A; Porter, S; Fedele, S; (2015) Orofacial Granulomatosis. Dermatol Clin , 33 (3) pp. 433- 446. 10.1016/j.det.2015.03.008. Downloaded from UCL Discovery: http://discovery.ucl.ac.uk/1470143 ARTICLE Oro-facial Granulomatosis Arwa Al-Hamad1, 2, Stephen Porter1, Stefano Fedele1, 3 1 University College London, UCL Eastman Dental Institute, Oral Medicine Unit, 256 Gray’s Inn Road, WC1X 8LD, London UK. 2 Dental Services, King Abdulaziz Medical City-Riyadh, Ministry of National Guard, Riyadh, Saudi Arabia. 3 NIHR University College London Hospitals Biomedical Research Centre, London, UK. Acknowledgments: Part of this work was undertaken at University College London/University College London Hospital, which received a proportion of funding from the Department of Health’s National Institute for Health Research Biomedical Research Centre funding scheme. Conflicts of Interest: The authors declare that they have no affiliation with any organization with a financial interest, direct or indirect, in the subject matter or materials discussed in the manuscript that may affect the conduct or reporting of the work submitted. Authorship: all authors named above meet the following criteria of the International Committee of Medical Journal Editors: 1) Substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data; 2) Drafting the article or revising it critically for important intellectual content; 3) Final approval of the version to be published. Corresponding author: Dr. Stefano Fedele DDS, PhD -

A Patient with Plaque Type Morphea Mimicking Systemic Lupus Erythematosus
CASE REPORT A Patient With Plaque Type Morphea Mimicking Systemic Lupus Erythematosus Wardhana1, EA Datau2 1 Department of Internal Medicine, Siloam International Hospitals. Karawaci, Indonesia. 2 Department of Internal Medicine, Prof. Dr. RD Kandou General Hospital & Sitti Maryam Islamic Hospital, Manado, North Sulawesi, Indonesia. Correspondence mail: Siloam Hospitals Group’s CEO Office, Siloam Hospital Lippo Village. 5th floor. Jl. Siloam No.6, Karawaci, Indonesia. email: [email protected] ABSTRAK Morfea merupakan penyakit jaringan penyambung yang jarang dengan gambaran utama berupa penebalan dermis tanpa disertai keterlibatan organ dalam. Penyakit ini juga dikenal sebagai bagian dari skleroderma terlokalisir. Berdasarkan gambaran klinis dan kedalaman jaringan yang terlibat, morfea dikelompokkan ke dalam beberapa bentuk dan sekitar dua pertiga orang dewasa dengan morfea mempunyai tipe plak. Produksi kolagen yang berlebihan oleh fibroblast merupakan penyebab kelainan pada morfea dan mekanisme terjadinya aktivitas fibroblast yang berlebihan ini masih belum diketahui, meskipun beberapa mekanisme pernah diajukan. Morfe tipe plak biasanya bersifat ringan dan dapat sembuh dengan sendirinya. Morfea tipe plak yang penampilan klinisnya menyerupai lupus eritematosus sistemik, misalnya meliputi alopesia dan ulkus mukosa di mulut, jarang dijumpai. Sebuah kasus morfea tipe plak pada wanita berusia 20 tahun dibahas. Pasien ini diobati dengan imunosupresan dan antioksidan local maupun sistemik. Kondisi paisen membaik tanpa disertai efek samping yang berarti. Kata kunci: morfea, tipe plak. ABSTRACT Morphea is an uncommon connective tissue disease with the most prominent feature being thickening or fibrosis of the dermal without internal organ involvement. It is also known as a part of localized scleroderma. Based on clinical presentation and depth of tissue involvement, morphea is classified into several forms, and about two thirds of adults with morphea have plaque type. -

Oral Pathology Unmasking Gastrointestinal Disease
Journal of Dental Health Oral Disorders & Therapy Review Article Open Access Oral pathology unmasking gastrointestinal disease Abstract Volume 5 Issue 5 - 2016 Different ggastrointestinal disorders, such as Gastroesophageal Reflux Disease (GERD), Celiac Disease (CD) and Crohn’s disease, may manifest with alterations of the oral cavity Fumagalli LA, Gatti H, Armano C, Caruggi S, but are often under and misdiagnosed both by physicians and dentists. GERD can cause Salvatore S dental erosions, which are the main oral manifestation of this disease, or other multiple Department of Pediatric, Università dell’Insubria, Italy affections involving both hard and soft tissues such as burning mouth, aphtous oral ulcers, Correspondence: Silvia Salvatore, Pediatric Department of erythema of soft palate and uvula, stomatitis, epithelial atrophy, increased fibroblast number Pediatric, Università dell’Insubria, Via F. Del Ponte 19, 21100 in chorion, xerostomia and drooling. CD may be responsible of recurrent aphthous stomatitis Varese, Italy, Tel 0039 0332 299247, Fax 0039 0332 235904, (RAS), dental enamel defects, delayed eruption of teeth, atrophic glossitis and angular Email chelitis. Crohn’s disease can occur with several oral manifestations like indurated tag-like lesions, clobbestoning, mucogingivitis or, less specifically, with RAS, angular cheilitis, Received: October 30, 2016 | Published: December 12, 2016 reduced salivation, halitosis, dental caries and periodontal involvement, candidiasis, odynophagia, minor salivary gland enlargement, perioral -

PRACTICAL CLINICAL COURSES V3969 Common Frustrating Oral
PRACTICAL CLINICAL COURSES A Service of the Gordon J. Christensen Career Development Program V3969 Common Frustrating Oral Diseases – Diagnosis & Treatment John A. Svirsky, DDS, MEd Gordon J. Christensen, DDS, MSD, PhD Materials Included C.E. Instruction Sheet Products List Clinician Responsible Goals & Objectives Overview References AGD Post-Test Non-SLS Toothpastes Therapy – Treatments 1 Gordon J. Christensen PRACTICAL CLINICAL COURSES PROCEDURE FOR RECEIVING ACADEMY OF GENERAL DENTISTRY AND STATE CREDIT FOR DVDS 1. Complete the enclosed Post-Test.* For each CE Video Purchased, one test is included. If additional tests are needed, the following fees will apply: $25 per test for 1 additional dentist; $10 per test for each auxiliary (dental assistants, hygienists, lab technicians - no limit on auxiliary tests). Fees can be paid either by check or credit card when tests are submitted to Practical Clinical Courses. 2. Complete the demographic information located at the end of the test. Type of Credit: a. If the applicant selects “State,” PCC will send a certificate of verification to the applicant. The applicant must then submit this certificate to his/her state board to obtain credit. b. If the applicant selects “AGD,” PCC will submit credit information to the Academy of General Dentistry and confirmation to the applicant that it has been submitted. (The applicant may check their AGD transcript for verification – please allow 30 days.) c. If the applicant selects “Both,” PCC will complete a. & b. above. 3. Return the Post-Test portion via mail, fax, or email. Our contact information is as follows: Practical Clinical Courses 3707 N Canyon Road Suite 3D Provo, UT 84604 Fax: (801) 226-8637 [email protected] 4. -

Distribution of Oral Ulceration Cases in Oral Medicine Integrated Installation of Universitas Padjadjaran Dental Hospital
Padjadjaran Journal of Dentistry. 2020;32(3):237-242. Distribution of oral ulceration cases in Oral Medicine Integrated Installation of Universitas Padjadjaran Dental Hospital Dewi Zakiawati1*, Nanan Nur'aeny1, Riani Setiadhi1 1*Department of Oral Medicine, Faculty of Dentistry Universitas Padjadjaran, Indonesia ABSTRACT Introduction: Oral ulceration defines as discontinuity of the oral mucosa caused by the damage of both epithelium and lamina propria. Among other types of lesions, ulceration is the most commonly found lesion in the oral mucosa, especially in the outpatient unit. Oral Medicine Integrated Installation (OMII) Department in Universitas Padjadjaran Dental Hospital serves as the centre of oral health and education services, particularly in handling outpatient oral medicine cases. This research was the first study done in the Department which aimed to observe the distribution of oral ulceration in OMII Department university Dental Hospital. The data is essential in studying the epidemiology of the diseases. Methods: The research was a descriptive study using the patient’s medical data between 2010 and 2012. The data were recorded with Microsoft® Excel, then analysed and presented in the table and diagram using GraphPad Prism® Results: During the study, the distribution of oral ulceration cases found in OMII Department was 664 which comprises of traumatic ulcers, recurrent aphthous stomatitis, angular cheilitis, herpes simplex, herpes labialis, and herpes zoster. Additionally, more than 50% of the total case was recurrent aphthous stomatitis, with a precise number of 364. Conclusion: It can be concluded that the OMII Department in university Dental Hospital had been managing various oral ulceration cases, with the most abundant cases being recurrent aphthous stomatitis. -

Oral Manifestations of Pemphigus Vulgaris
Journal of Clinical & Experimental Dermatology Research - Open Access Research Article OPEN ACCESS Freely available online doi:10.4172/2155-9554.1000112 Oral Manifestations of Pemphigus Vulgaris: Clinical Presentation, Differential Diagnosis and Management Antonio Bascones-Martinez1*, Marta Munoz-Corcuera2, Cristina Bascones-Ilundain1 and German Esparza-Gómez1 1DDS, PhD, Medicine and Bucofacial Surgery Department, Dental School, Complutense University of Madrid, Spain 2DDS, PhD Student, Medicine and Bucofacial Surgery Department, Dental School, Complutense University of Madrid, Spain Abstract Pemphigus vulgaris is a chronic autoimmune mucocutaneous disease characterized by the formation of intraepithelial blisters. It results from an autoimmune process in which antibodies are produced against desmoglein 1 and desmoglein 3, normal components of the cell membrane of keratinocytes. The first manifestations of pemphigus vulgaris appear in the oral mucosa in the majority of patients, followed at a later date by cutaneous lesions. The diagnosis is based on clinical findings and laboratory analyses, and it is usually treated by the combined administration of corticosteroids and immunosuppressants. Detection of the oral lesions can result in an earlier diagnosis. We review the oral manifestations of pemphigus vulgaris as well as the differential diagnosis, treatment, and prognosis of oral lesions in this uncommon disease. Keywords: Pemphigus; Oral mucosa; Autoimmune bullous disease and have a molecular weight of 130 and 160 KDa, respectively [1,7,9,13]. The binding of antibodies to desmoglein at mucosal or Introduction cutaneous level gives rise to the loss of cell adhesion, with separation of epithelial layers (acantholysis) and the consequent appearance of Pemphigus vulgaris (PV) is the most frequently observed blisters on skin or mucosae [1,3]. -
Nodular Morphea
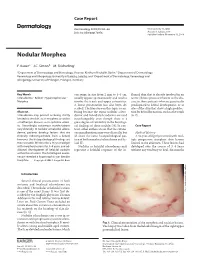
Case Report Dermatology 2009;218:63–66 Received: July 13, 2008 DOI: 10.1159/000173976 Accepted: July 23, 2008 Published online: November 13, 2008 Nodular Morphea a b c F. Kauer J.C. Simon M. Sticherling a b Department of Dermatology and Venerology, Vivantes Klinikum Neukölln, Berlin , Department of Dermatology, c Venerology and Allergology, University of Leipzig, Leipzig , and Department of Dermatology, Venerology and Allergology, University of Erlangen, Erlangen , Germany Key Words can range in size from 2 mm to 4–5 cm, flamed skin that is already involved in an -Scleroderma ؒ Keloid ؒ Hypertrophic scar ؒ usually appear spontaneously and tend to active fibrotic process inherent to the dis Morphea involve the trunk and upper extremities. ease in those patients who are genetically A linear presentation has also been de- predisposed to keloid development, or at scribed. The literature on this topic is con- sites of the skin that show a high predilec- Abstract fusing because the terms ‘nodular sclero- tion for keloid formation, such as the trunk Scleroderma may present as being strictly derma’ and ‘keloidal scleroderma’ are used [6, 7] . limited to the skin, as in morphea, or within interchangeably even though there is a a multiorgan disease, as in systemic sclero- great degree of variability in the histologi- sis. Accordingly, cutaneous manifestations cal findings of these nodules [4] . In con- C a s e R e p o r t vary clinically. In nodular or keloidal sclero- trast, other authors stress that the cutane- derma, patients develop lesions that are ous manifestations may vary clinically, but Medical History clinically indistinguishable from a keloid; all share the same histopathological pat- A 16-year-old girl presented with mul- however, the histopathological findings are tern of both morphea/scleroderma and ke- tiple progressive morpheic skin lesions more variable.