Climate Change and Health Risks in Senegal
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Road Travel Report: Senegal
ROAD TRAVEL REPORT: SENEGAL KNOW BEFORE YOU GO… Road crashes are the greatest danger to travelers in Dakar, especially at night. Traffic seems chaotic to many U.S. drivers, especially in Dakar. Driving defensively is strongly recommended. Be alert for cyclists, motorcyclists, pedestrians, livestock and animal-drawn carts in both urban and rural areas. The government is gradually upgrading existing roads and constructing new roads. Road crashes are one of the leading causes of injury and An average of 9,600 road crashes involving injury to death in Senegal. persons occur annually, almost half of which take place in urban areas. There are 42.7 fatalities per 10,000 vehicles in Senegal, compared to 1.9 in the United States and 1.4 in the United Kingdom. ROAD REALITIES DRIVER BEHAVIORS There are 15,000 km of roads in Senegal, of which 4, Drivers often drive aggressively, speed, tailgate, make 555 km are paved. About 28% of paved roads are in fair unexpected maneuvers, disregard road markings and to good condition. pass recklessly even in the face of oncoming traffic. Most roads are two-lane, narrow and lack shoulders. Many drivers do not obey road signs, traffic signals, or Paved roads linking major cities are generally in fair to other traffic rules. good condition for daytime travel. Night travel is risky Drivers commonly try to fit two or more lanes of traffic due to inadequate lighting, variable road conditions and into one lane. the many pedestrians and non-motorized vehicles sharing the roads. Drivers commonly drive on wider sidewalks. Be alert for motorcyclists and moped riders on narrow Secondary roads may be in poor condition, especially sidewalks. -

Calcium Phosphate of Kolda Reasons to Invest?
CALCIUM PHOSPHATE OF KOLDA REASONS TO INVEST? Phosphates have been the main mineral used in Senegal with a good contribution to the country's GDP. For example, the use of phosphates began in 1949 for aluminum Thiès. Besides this western part, there is a deposit in Matam in the north, some indices in the central region (Kaolack, Fatick, Diourbel, Louga, Kaffrine) and southern (Kolda and Ziguinchor). This paper aims to study the host country, its legal framework and geological order to justify the exploitation and utilization of calcium phosphate in Kolda. CALCIUM PHOSPHATE OF KOLDA OVERVIEW OF SENEGAL Situated in the extreme west of the African continent, Senegal is located between 12 ° 8:16 ° 41 north latitude and 11 ° 21 and 17 ° 32 west longitude. The country is bordered by the Atlantic Ocean to the west, Mauritania to the north, La ré gion dé Mali to the east, Guinea Bissau Guinea to the south and the KoldaThé région of southeast. The Gambia is an enclave in southern Senegal in Kolda length within which penetrates deeply. With an area of La région de Kolda The Kolda region has 3 196,722 km2, Senegal, with Dakar as capital, has 12 million compte trois (03) inhabitants distributed evenly so the 14 administrative departments, 9 districts départements, neuf (09) regions (density of 61.1 ² hab / km and the population and 31 rural growth rate: 2.34 %). arrondissements neuf communities. With an (09) communes et trente area of 21011 km ², une (31) communautés Kolda has 847,243 rurales. Avec une inhabitants with a superficie de 21011 km², density of 40 inhabitants Kolda compte 847243 / km ². -
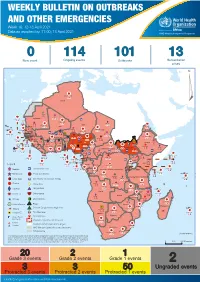
Week 16: 12-18 April 2021
WEEKLY BULLETIN ON OUTBREAKS AND OTHER EMERGENCIES Week 16: 12-18 April 2021 Data as reported by: 17:00; 18 April 2021 REGIONAL OFFICE FOR Africa WHO Health Emergencies Programme 0 114 101 13 New event Ongoing events Outbreaks Humanitarian crises 119 642 3 155 Algeria ¤ 36 13 110 0 5 694 170 Mauritania 7 2 13 070 433 110 0 7 0 Niger 17 129 453 Mali 3 491 10 567 0 6 0 2 079 4 4 706 169 Eritrea Cape Verde 39 782 1 091 Chad Senegal 5 074 189 61 0 Gambia 27 0 3 0 20 466 191 973 5 Guinea-Bissau 847 17 7 0 Burkina Faso 236 49 242 028 3 370 0 164 233 2 061 Guinea 13 129 154 12 38 397 1 3 712 66 1 1 23 12 Benin 30 0 Nigeria 1 873 72 0 Ethiopia 540 2 481 5 6 188 15 Sierra Leone Togo 3 473 296 61 731 919 52 14 Ghana 5 787 75 Côte d'Ivoire 10 473 114 14 484 479 63 0 40 0 Liberia 17 0 South Sudan Central African Republic 916 2 45 0 97 17 25 0 21 612 260 45 560 274 91 709 771 Cameroon 7 0 28 676 137 5 330 13 151 653 2 481 655 2 43 0 119 12 6 1 488 6 4 028 79 12 533 7 259 106 Equatorial Guinea Uganda 542 8 Sao Tome and Principe 32 11 2 066 85 41 378 338 Kenya Legend 7 611 95 Gabon Congo 2 012 73 Rwanda Humanitarian crisis 2 275 35 23 888 325 Measles 21 858 133 Democratic Republic of the Congo 10 084 137 Burundi 3 612 6 Monkeypox Ebola virus disease Seychelles 28 956 745 235 0 420 29 United Republic of Tanzania Lassa fever Skin disease of unknown etiology 190 0 4875 25 509 21 Cholera Yellow fever 1 349 5 6 257 229 24 389 561 cVDPV2 Dengue fever 90 918 1 235 Comoros Angola Malawi COVID-19 Chikungunya 33 941 1 138 862 0 3 815 146 Zambia 133 0 Mozambique -

Teranga Development Strategy
TERANGA DEVELOPMENT STRATEGY FEBRUARY 2014 PREPARED BY TABLE OF CONTENTS 1.0 INTRODUCTION 4 1.1 PURPOSE OF THE TDS 5 1.2 OUR PRIORITY OUTCOMES 7 1.3 OUR FOCUS AREA 8 1.4 MYTHODOLOGY 10 1.5 DOCUMENT STRUCTURE 14 2.0 OUR MINE OPERATION 15 2.1 THE SABODALA GOLD OPERATION 16 2.2 OUR FUTURE GROWTH 18 3.0 UNDERSTANDING OUR REGION 20 3.1 INTRODUCTION 21 3.2 GOVERNANCE 22 3.3 DEVELOPMENT PLANNING 27 3.4 AGRICULTURE AND LIVELIHOOD 31 3.5 EDUCATION 38 3.6 ENERGY AND INFRASTRUCTURE 46 3.7 TRANSPORTATION INFRASTRUCTURE 50 3.8 HEALTH, SAFETY AND SECURITY 53 3.9 WATER INFRASTRUCTURE 66 3.10 SANITATION INFRASTRUCTURE 70 3.11 HOUSING 72 3.12 ENVIRONMENT AND CONSERVATION 74 4.0 OUR VISION FOR OUR ROLE IN THE REGION 79 5.0 A SPATIAL STRUCTURE TO SUPPORT REGIONAL DEVELOPMENT 81 5.1 INTRODUCTION 82 5.2 THE GOLD DISTRICT CONCEPTUAL SPATIAL PLAN 87 2 6.0 OUR ACTIONS 92 6.1 INTRODUCTION 93 6.2 JOBS AND PEOPLE DEVELOPMENT 94 6.3 LAND ACQUISITION 102 6.4 PROCUREMENT 106 6.5 HEALTH, SAFETY AND SECURITY 110 6.6 MINE-RELATED INFRASTRUCTURE 116 6.7 WORKER HOUSING 119 6.8 COMMUNITY RELATIONS 121 6.9 MINE CLOSURE AND REHABILITATION 125 6.10 FINANCIAL PAYMENTS AND INVESTMENTS 129 LIST OF ACRONYMS 143 TERANGA DEVELOPMENT STRATEGY 3 SECTION 1 INTRODUCTION 4 1.1 PURPOSE OF THE TDS As the first gold mine in Senegal, Teranga has a unique opportunity to set the industry standard for socially responsible mining in the country. -
K O L D a 2 0
REPUBLIQUE DU SENEGAL Un Peuple – Un But – Une Foi ------------------ MINISTERE DE L’ECONOMIE, DES FINANCES ET DU PLAN K ------------------ AGENCE NATIONALE DE LA STATISTIQUE ET DE LA DEMOGRAPHIE ------------------ Service Régional de la Statistique et de la Démographie de Kolda O L D A 2 0 SITUATION ECONOMIQUE ET SOCIALE REGIONALE 2014 1 4 Mai 2017 COMITE DE DIRECTION Directeur Général Aboubacar Sédikh BEYE Directeur Général Adjoint Babacar NDIR Conseiller à l’Action Régionale Mamadou DIENG COMITE DE REDACTION Chef du Service Régional Mamanding DIEDHIOU Adjoint chef de service Hadime SANE COMITE DE LECTURE Seckène SENE Direction Générale Abdoulaye Mamadou TALL Direction Générale Mamadou DIENG Direction Générale Saliou MBENGUE OPCV El Hadji Malick GUEYE DMIS Mamadou BAH DMIS Alain François DIATTA DMIS Amadou Fall DIOUF DSDS Adjibou Oppa BARRY DSDS Atoumane FALL DSDS Jean Rodrigue MALOU DSDS Bintou DIACK LY DSECN Momath CISSE CGP Awa CISSOKHO FAYE DSDS Ramlatou DIALLO DSECN Oumar DIOP DMIS Ndeye Aida FAYE TALL DSDS Ndeye Binta DIEME COLY DSDS Mamadou AMOUZOU OPCV AGENCE NATIONALE DE LA STATISTIQUE ET DELA DEMOGRAPHIE Rocade Fann –Bel-air–Cerf-volant – Dakar Sénégal. B.P. 116 Dakar R.P. - Sénégal Téléphone (221) 33 869 21 39 - Fax (221) 33 824 36 15 Site web : www.ansd.sn ; Email: [email protected] Distribution : Division de la Documentation, de la Diffusion et des Relations avec les Usagers Service Régional de la Statistique et de la Démographie de Kolda Adresse : quartier Bouna KANE rue de Ziguinchor Tél :33 996 10 32 B.P. :103 ii TABLE DES MATIERES TABLE DES MATIERES ____________________________________________________________ 3 ABREVIATIONS, SIGLES ET ACRONYMES _____________________________________________ 6 Chapitre I : PRESENTATION DE LA REGION DE KOLDA ___________________________________ 8 I.1. -

I. Project Context and Development Objectives ...5
Document of The World Bank FOR OFFICIAL USE ONLY Public Disclosure Authorized Report No: ICR00005096 IMPLEMENTATION COMPLETION AND RESULTS REPORT IDA-47370; IDA-57310 ON CREDITS Public Disclosure Authorized IN THE AMOUNT OF SDR 71.9 MILLION (US$105 MILLION EQUIVALENT) TO THE REPUBLIC OF SENEGAL Public Disclosure Authorized FOR A SENEGAL: TRANSPORT AND URBAN MOBILITY PROJECT June 17, 2020 Transport Global Practice Africa Region Public Disclosure Authorized This document has a restricted distribution and may be used by recipients only in the performance of their official duties. Its contents may not otherwise be disclosed without World Bank authorization. CURRENCY EQUIVALENTS (Exchange Rate Effective April 30, 2020) Currency Unit = CFA Francs ( XO F) XOF 603= US$1 US$ 1.37= SDR 1 FISCAL YEAR July 1 – June 30 ABBREVIATIONS AND ACRONYMS AFTU Urban Transport Financing Association (Association de Financement des Transports Urbains) AGEROUTE Road Management Agency (Agence des Travaux et de Gestion des Routes) AF Additional Financing BRT Bus Rapid Transit CAS Country Assistance Strategy CEREEQ Experimental Research Centre for Equipment Studies CETUD Dakar Urban Transport Council (Conseil Exécutif des Transports Urbains de Dakar) CGQA Air Quality Management Center CPF Country Partnership Framework CPS Country Partnership Strategy DDD Dakar Mass Transit Company (Dakar-Dem-Dik) DGI Infrastructure General Directorate DR Directorate of Roads (Direction des Routes) DTR Directorate of Road Transports (Direction des Transports Routiers) DTT Directorate -
Mapping of Child Protection Accountability Mechanisms in Armed Conflict in Africa
1 LIST OF ACRONYMS Save the Children Somalia MAPPING OF CHILD PROTECTION ACCOUNTABILITY MECHANISMS IN ARMED CONFLICT IN AFRICA SAVE THE CHILDREN 1 MAPPING OF CHILD PROTECTION ACCOUNTABILITY MECHANISMS IN ARMED CONFLICT IN AFRICA ARMED CONFLICT IN MECHANISMS IN ACCOUNTABILITY MAPPING OF CHILD PROTECTION Save the Children Somalia 2 SAVE THE CHILDREN Save the Children is the world’s leading independent organisation for children. Save the Children works in more than 120 countries. We save children’s lives. We fight for their rights. We help them fulfil their potential. 1 LIST OF ACRONYMS Our vision A world in which every child attains the right to survival, protection, development and participation. Our mission To inspire breakthroughs in the way the world treats children and to achieve immediate and lasting change in their lives. We will stay true to our values of accountability, ambition, collaboration, creativity and integrity. Published by: Save the Children International East and Southern Africa Regional Office Regional Programming Unit Protecting Children in Conflict P.O. Box 19423-00202 Nairobi, Kenya Cellphone: +254 711 090 000 [email protected] www.savethechildren.net Save the Children East & Southern Africa Region SaveTheChildren E&SA @ESASavechildren https://www.youtube.com/channel/ UCYafJ7mw4EutPvYSkpnaruQ Project Lead: Anthony Njoroge Technical Lead: Fiona Otieno Reviewers: Simon Kadima, Joram Kibigo, Maryline Njoroge, Alexandra Chege, Mory Camara, Måns Welander, Anta Fall, Liliane Coulibaly, and Rita Kirema. © Save the Children International August 2019 Photos: Save the Children SAVE THE CHILDREN 3 Save the Children is the world’s leading independent organisation for children. Save the Children works in more than 120 countries. -
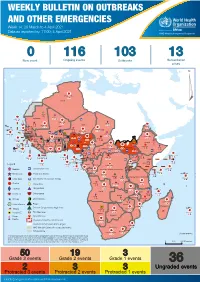
Weekly Bulletin on Outbreaks
WEEKLY BULLETIN ON OUTBREAKS AND OTHER EMERGENCIES Week 14: 29 March to 4 April 2021 Data as reported by: 17:00; 4 April 2021 REGIONAL OFFICE FOR Africa WHO Health Emergencies Programme 0 116 103 13 New event Ongoing events Outbreaks Humanitarian crises 117 622 3 105 Algeria ¤ 36 13 110 0 5 420 164 Mauritania 7 2 10 501 392 110 0 7 0 Niger 17 927 449 Mali 3 334 10 567 0 6 0 2 079 4 4 595 165 Eritrea Cape Verde 38 520 1 037 Chad Senegal 4 918 185 59 0 Gambia 27 0 3 0 17 125 159 9 761 45 Guinea-Bissau 796 17 7 0 Burkina Faso 225 46 215 189 2 963 0 162 593 2 048 Guinea 12 817 150 12 38 397 1 3 662 66 1 1 23 12 Benin 30 0 Nigeria 1 873 71 0 Ethiopia 420 14 481 5 6 188 15 Sierra Leone Togo 3 473 296 53 920 779 52 14 Ghana 5 245 72 Côte d'Ivoire 10 098 108 14 484 479 63 0 40 0 Liberia 17 0 South Sudan Central African Republic 916 2 45 0 25 0 19 670 120 43 180 237 90 287 740 Cameroon 7 0 28 676 137 5 330 13 138 988 2 224 1 952 87 655 2 51 22 43 0 112 12 6 1 488 6 3 988 79 11 187 6 902 102 Equatorial Guinea Uganda 542 8 Sao Tome and Principe 32 11 2 042 85 41 016 335 Kenya Legend 7 100 90 Gabon Congo 18 504 301 Rwanda Humanitarian crisis 2 212 34 22 482 311 Measles 18 777 111 Democratic Republic of the Congo 9 681 135 Burundi 2 964 6 Monkeypox Ebola virus disease Seychelles 27 930 739 1 525 0 420 29 United Republic of Tanzania Lassa fever Skin disease of unknown etiology 189 0 4 084 20 509 21 Cholera Yellow fever 1 349 5 6 257 229 22 631 542 cVDPV2 Dengue fever 88 930 1 220 Comoros Angola Malawi COVID-19 Chikungunya 33 661 1 123 862 0 3 719 146 -

Mali's Infrastructure
COUNTRY REPORT Mali’s Infrastructure: A Continental Perspective Cecilia M. Briceño-Garmendia, Carolina Dominguez and Nataliya Pushak JUNE 2011 © 2011 The International Bank for Reconstruction and Development / The World Bank 1818 H Street, NW Washington, DC 20433 USA Telephone: 202-473-1000 Internet: www.worldbank.org E-mail: [email protected] All rights reserved A publication of the World Bank. The World Bank 1818 H Street, NW Washington, DC 20433 USA The findings, interpretations, and conclusions expressed herein are those of the author(s) and do not necessarily reflect the views of the Executive Directors of the International Bank for Reconstruction and Development / The World Bank or the governments they represent. The World Bank does not guarantee the accuracy of the data included in this work. The boundaries, colors, denominations, and other information shown on any map in this work do not imply any judgment on the part of The World Bank concerning the legal status of any territory or the endorsement or acceptance of such boundaries. Rights and permissions The material in this publication is copyrighted. Copying and/or transmitting portions or all of this work without permission may be a violation of applicable law. The International Bank for Reconstruction and Development / The World Bank encourages dissemination of its work and will normally grant permission to reproduce portions of the work promptly. For permission to photocopy or reprint any part of this work, please send a request with complete information to the Copyright Clearance Center Inc., 222 Rosewood Drive, Danvers, MA 01923 USA; telephone: 978-750-8400; fax: 978-750-4470; Internet: www.copyright.com. -

Cdm-Ar-Pdd) (Version 05)
CLEAN DEVELOPMENT MECHANISM PROJECT DESIGN DOCUMENT FORM for A/R CDM project activities (CDM-AR-PDD) (VERSION 05) TABLE OF CONTENTS SECTION A. General description of the proposed A/R CDM project activity 2 SECTION B. Duration of the project activity / crediting period 19 SECTION C. Application of an approved baseline and monitoring methodology 20 SECTION D. Estimation of ex ante actual net GHG removals by sinks, leakage, and estimated amount of net anthropogenic GHG removals by sinks over the chosen crediting period 26 SECTION E. Monitoring plan 33 SECTION F. Environmental impacts of the proposed A/R CDM project activity 43 SECTION G. Socio-economic impacts of the proposed A/R CDM project activity 44 SECTION H. Stakeholders’ comments 45 ANNEX 1: CONTACT INFORMATION ON PARTICIPANTS IN THE PROPOSED A/R CDM PROJECT ACTIVITY 50 ANNEX 2: INFORMATION REGARDING PUBLIC FUNDING 51 ANNEX 3: BASELINE INFORMATION 51 ANNEX 4: MONITORING PLAN 51 ANNEX 5: COORDINATES OF PROJECT BOUNDARY 52 ANNEX 6: PHASES OF PROJECT´S CAMPAIGNS 78 ANNEX 7: SCHEDULE OF CINEMA-MEETINGS 81 ANNEX 8: STATEMENTS OF THE DNA 86 ANNEX 9: LETTER OF THE MINISTRY OF ENVIRONMENT REGARDING EIA 88 ANNEX 10: RARE AND ENDANGERED SPECIES 89 ANNEX 11: ELIGIBILITY ASSESSMENT PHASES 91 SECTION A. General description of the proposed A/R CDM project activity A.1. Title of the proposed A/R CDM project activity: >> Title: Oceanium mangrove restoration project Version of the document: 01 Date of the document: November 10 2010. A.2. Description of the proposed A/R CDM project activity: >> The proposed A/R CDM project activity plans to establish 1700 ha of mangrove plantations on currently degraded wetlands in the Sine Saloum and Casamance deltas, Senegal. -
Weekly Bulletin on Outbreaks
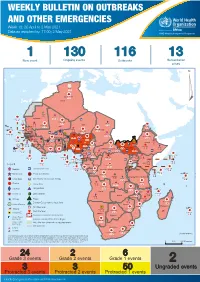
WEEKLY BULLETIN ON OUTBREAKS AND OTHER EMERGENCIES Week 18: 26 April to 2 May 2021 Data as reported by: 17:00; 2 May 2021 REGIONAL OFFICE FOR Africa WHO Health Emergencies Programme 1 130 116 13 New event Ongoing events Outbreaks Humanitarian crises 64 0 122 522 3 270 Algeria ¤ 36 13 612 0 5 901 175 Mauritania 7 2 13 915 489 110 0 7 0 Niger 18 448 455 Mali 3 671 10 567 0 6 0 2 079 4 4 828 170 Eritrea Cape Verde 40 433 1 110 Chad Senegal 5 074 189 61 0 Gambia 27 0 3 0 24 368 224 1 069 5 Guinea-Bissau 847 17 7 0 Burkina Faso 236 49 258 384 3 726 0 165 167 2 063 Guinea 13 319 157 12 3 736 67 1 1 23 12 Benin 30 0 Nigeria 1 873 72 0 Ethiopia 540 2 556 5 6 188 15 Sierra Leone Togo 3 473 296 52 14 Ghana 70 607 1 064 6 411 88 Côte d'Ivoire 10 583 115 14 484 479 65 0 40 0 Liberia 17 0 South Sudan Central African Republic 1 029 2 49 0 97 17 25 0 22 333 268 46 150 287 92 683 779 Cameroon 7 0 28 676 137 843 20 3 1 160 422 2 763 655 2 91 0 123 12 6 1 488 6 4 057 79 13 010 7 694 112 Equatorial Guinea Uganda 1 0 542 8 Sao Tome and Principe 32 11 2 066 85 41 973 342 Kenya Legend 7 821 99 Gabon Congo 2 012 73 Rwanda Humanitarian crisis 2 310 35 25 253 337 Measles 23 075 139 Democratic Republic of the Congo 11 016 147 Burundi 4 046 6 Monkeypox Ebola virus disease Seychelles 29 965 768 235 0 420 29 United Republic of Tanzania Lassa fever Skin disease of unknown etiology 191 0 5 941 26 509 21 Cholera Yellow fever 63 1 6 257 229 26 993 602 cVDPV2 Dengue fever 91 693 1 253 Comoros Angola Malawi COVID-19 Leishmaniasis 34 096 1 148 862 0 3 840 146 Zambia 133 -

Senegal Country Development Cooperation Strategy Original Dates: April 2, 2012 – April 2, 2017 Extended Through: April 2, 2019 Extended On: May 4, 2017
SENEGAL COUNTRY DEVELOPMENT COOPERATION STRATEGY ORIGINAL DATES: APRIL 2, 2012 – APRIL 2, 2017 EXTENDED THROUGH: APRIL 2, 2019 EXTENDED ON: MAY 4, 2017 May 2017 This publication was produced by the United States Agency for International Development. It was prepared by USAID/Senegal. SENEGAL COUNTRY DEVELOPMENT COOPERATION STRATEGY ORIGINAL DATES: APRIL 2, 2012 – APRIL 2, 2017 EXTENDED THROUGH: APRIL 2, 2019 EXTENDED ON: MAY 4, 2017 1 CONTENTS CONTENTS ................................................................................................................................................. 2 ACRONYMS ................................................................................................................................................ 3 1. DEVELOPMENT CONTEXT, CHALLENGES AND OPPORTUNITIES ....................................... 5 2. USAID/SENEGAL DEVELOPMENT OBJECTIVES ........................................................................ 10 3. MONITORING, EVALUATION AND LEARNING ........................................................................ 39 ANNEX A. M&E TABLE .......................................................................................................................... 43 2 ACRONYMS Abbreviations and acronyms have been kept to a minimum in the text of this document. Where abbreviations or acronyms have been used, they are accompanied by their full expression the first time they appear, unless they are commonly used and generally understood abbreviations such as NGO, kg., etc. However, in order to