Techniques for Differentiating Motor and Sensory Fascicles of a Peripheral Nerve—A Review
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Electromagnetic Field and TGF-Β Enhance the Compensatory
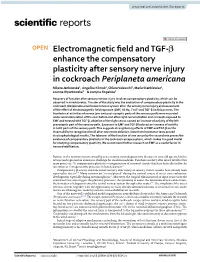
www.nature.com/scientificreports OPEN Electromagnetic feld and TGF‑β enhance the compensatory plasticity after sensory nerve injury in cockroach Periplaneta americana Milena Jankowska1, Angelika Klimek1, Chiara Valsecchi2, Maria Stankiewicz1, Joanna Wyszkowska1* & Justyna Rogalska1 Recovery of function after sensory nerves injury involves compensatory plasticity, which can be observed in invertebrates. The aim of the study was the evaluation of compensatory plasticity in the cockroach (Periplaneta americana) nervous system after the sensory nerve injury and assessment of the efect of electromagnetic feld exposure (EMF, 50 Hz, 7 mT) and TGF‑β on this process. The bioelectrical activities of nerves (pre‑and post‑synaptic parts of the sensory path) were recorded under wind stimulation of the cerci before and after right cercus ablation and in insects exposed to EMF and treated with TGF‑β. Ablation of the right cercus caused an increase of activity of the left presynaptic part of the sensory path. Exposure to EMF and TGF‑β induced an increase of activity in both parts of the sensory path. This suggests strengthening efects of EMF and TGF‑β on the insect ability to recognize stimuli after one cercus ablation. Data from locomotor tests proved electrophysiological results. The takeover of the function of one cercus by the second one proves the existence of compensatory plasticity in the cockroach escape system, which makes it a good model for studying compensatory plasticity. We recommend further research on EMF as a useful factor in neurorehabilitation. Injuries in the nervous system caused by acute trauma, neurodegenerative diseases or even old age are hard to reverse and represent an enormous challenge for modern medicine. -

Journal of Biomechanical Science and Engineering Researches on Biomechanical Properties and Models of Peripheral Nerves
Bulletin of the JSME Vol.12, No.1, 2017 Journal of Biomechanical Science and Engineering 【Review Paper】 Researches on biomechanical properties and models of peripheral nerves - a review Ming-Shaung JU*, Chou-Ching K. LIN** and Cheng-Tao CHANG* *Department of Mechanical Engineering, National Cheng Kung University 1 University Road, Tainan 701, Taiwan (R.O.C.) E-mail: [email protected] **Department of Neurology College of Medicine and University Hospital National Cheng Kung University 1 University Road, Tainan 701, Taiwan (R.O.C.) Received: 14 December 2016; Revised: 11 February 2017; Accepted: 6 March 2017 Abstract The biomechanics of peripheral nerve plays an important role in physiology of the healthy and pathology of the diseased such as the diabetic neuropathy, the cauda equine compression and the carpal tunnel syndrome. The other application is recent development of neural prostheses. The goal of this paper is to review researches done by members of Taiwanese Society of Biomechanics on the biomechanics of peripheral nerves in the past two decades. First, a brief introduction of the anatomy of peripheral nerve is given. Then experiment designs and mechanical models for testing the nerves are presented. The material properties ranged from linear elastic to nonlinear visco-elastic and scales ranged from organ level to tissue level are reviewed. Implications of these studies to clinical problems will be addressed and the challenges and future perspective on biomechanics of peripheral nerve are discussed. Key words: Biomechanics, Peripheral nerve, Review, Diabetic mellitus, Cauda equine 1. Introduction Nervous system plays an important role in the human body it can coordinate voluntary and involuntary actions of other tissues and sub-systems. -

Peripheral Nerve Regeneration and Muscle Reinnervation
International Journal of Molecular Sciences Review Peripheral Nerve Regeneration and Muscle Reinnervation Tessa Gordon Department of Surgery, University of Toronto, Division of Plastic Reconstructive Surgery, 06.9706 Peter Gilgan Centre for Research and Learning, The Hospital for Sick Children, Toronto, ON M5G 1X8, Canada; [email protected]; Tel.: +1-(416)-813-7654 (ext. 328443) or +1-647-678-1314; Fax: +1-(416)-813-6637 Received: 19 October 2020; Accepted: 10 November 2020; Published: 17 November 2020 Abstract: Injured peripheral nerves but not central nerves have the capacity to regenerate and reinnervate their target organs. After the two most severe peripheral nerve injuries of six types, crush and transection injuries, nerve fibers distal to the injury site undergo Wallerian degeneration. The denervated Schwann cells (SCs) proliferate, elongate and line the endoneurial tubes to guide and support regenerating axons. The axons emerge from the stump of the viable nerve attached to the neuronal soma. The SCs downregulate myelin-associated genes and concurrently, upregulate growth-associated genes that include neurotrophic factors as do the injured neurons. However, the gene expression is transient and progressively fails to support axon regeneration within the SC-containing endoneurial tubes. Moreover, despite some preference of regenerating motor and sensory axons to “find” their appropriate pathways, the axons fail to enter their original endoneurial tubes and to reinnervate original target organs, obstacles to functional recovery that confront nerve surgeons. Several surgical manipulations in clinical use, including nerve and tendon transfers, the potential for brief low-frequency electrical stimulation proximal to nerve repair, and local FK506 application to accelerate axon outgrowth, are encouraging as is the continuing research to elucidate the molecular basis of nerve regeneration. -

How Is the Brain Organized?
p CHAPTER 2 How Is the Brain Organized? An Overview of Brain Structure The Functional Organization Brain Terminology of the Brain The Brain’s Surface Features Principle 1: The Sequence of Brain Processing The Brain’s Internal Features Is “In Integrate Out” Microscopic Inspection: Cells and Fibers Principle 2: Sensory and Motor Divisions Exist Focus on Disorders: Meningitis and Throughout the Nervous System Encephalitis Principle 3: The Brain’s Circuits Are Crossed Focus on Disorders: Stroke Principle 4: The Brain Is Both Symmetrical and Asymmetrical Principle 5: The Nervous System Works A Closer Look at Neuroanatomy Through Excitation and Inhibition The Cranial Nervous System Principle 6: The Central Nervous System Has The Spinal Nervous System Multiple Levels of Function The Internal Nervous System Principle 7: Brain Systems Are Organized Both Focus on Disorders: Magendie, Bell, and Bell’s Hierarchically and in Parallel Palsy Principle 8: Functions in the Brain Are Both Localized and Distributed A. Klehr / Stone Images Micrograph: Carolina Biological Supply Co. / Phototake 36 I p hen buying a new car, people first inspect the In many ways, examining a brain for the first time is outside carefully, admiring the flawless finish similar to looking under the hood of a car. We have a vague W and perhaps even kicking the tires. Then they sense of what the brain does but no sense of how the parts open the hood and examine the engine, the part of the car that we see accomplish these tasks. We may not even be responsible for most of its behavior—and misbehavior. able to identify many of the parts. -

Nervous System Central Nervous System Peripheral Nervous System
Peripheral Nervous System Involuntary reflexes (spinal cord); Organization of Nervous System: voluntary actions (higher brain centers) Nervous system Integration Central nervous system Peripheral nervous system (CNS) (PNS) Motor Sensory output input Brain Spinal cord Motor division Sensory division (efferent) (afferent) Autonomic nervous system Somatic nervous system (involuntary; smooth & cardiac muscle) (voluntary; skeletal muscle) Sympathetic division Parasympathetic division Peripheral Nervous System Motor Units: Motor Unit: A single motor neuron and all the muscle fibers innervated by it (motor unit = all-or-none) Motor unit size dictates control: Fine Control / Rapid Reaction: 1-10 fibers / MU (e.g., ocular muscles) Gross Control / Slow Reaction: 1000’s fibers / MU (e.g., quadriceps) Recruitment: Addition of motor units to produce smooth, steady muscle tension (multiple fiber summation) Motoneuron Pool: Set of motor neurons innervating Small large motor units activated… muscle fibers within the same muscle • Varying thresholds Motor units overlap; provides coordination Marieb & Hoehn – Figure 9.13 1 Peripheral Nervous System Types of Motor Neurons: 1) Alpha () motor neurons: • Give rise to large Type A alpha (A) motor nerve fibers (~ 14 µm diameter) • Innervate extrafusal skeletal muscle fibers (generate force) 2) Gamma () motor neurons: • Give rise to small Type A gamma (Aγ) motor nerve fibers (~ 5 µm diameter) • Innervate intrafusal muscle fibers (small, specialized fibers – muscle spindle) What is the length of the muscle? Proper -
The Nervous System Unit One: Source
UNIT ONE THE NERVOUS SYSTEM Unit One: The Nervous System UNC-CH Brain Explorers May be reproduced for non-profit educational use only. Please credit source. 3 UNIT ONE THE NERVOUS SYSTEM Unit One: The Nervous System UNC-CH Brain Explorers May be reproduced for non-profit educational use only. Please credit source. 4 THE NERVOUS SYSTEM UNIFYING SUMMARY KEY POINTS CONCEPTS FULL BODY TRACING • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • Models help us understand and In the Full Body Tracing students • All our thooughts, movements, explain the world.* work together as a class to create sensations and emotions are • Systems are made of parts which a model of the nervous system. controlled by the nervous system. connect to create the whole.* The outline of a student’s body is • We have a Central Nervous • The brain receives informational traced on a large piece of paper. System (brain and spinal cord) signals from all parts of the body. A cardboard cut out of the brain and Peripheral Nervous System The brain sends signals to all parts and spinal cord are placed in the (nerves extending from the spinal of the body to influence what they outline to represent the central cord to limbs, trunk, face, organs do.* nervous system. Two colors of and throughout.) • Humans have systems for yarn, representing the motor and • Sensory nerves communicate digestion, circulation, movement sensory nerves, are used to create information from the body to the and coordination. These systems motor and sensory pathways of brain and motor nerves, from the interact with one another.* the peripheral nervous system. brain to the body. -

685 Mechanisms and Controllers of Eccrine Sweating in Humans Manabu Shiba
[Frontiers in Bioscience S2, 685-696, January 1, 2010] Mechanisms and controllers of eccrine sweating in humans Manabu Shibasaki1, Craig G. Crandall2,3 1Department of Environmental and Life Sciences, Nara Women's University Graduate School of Humanities and Sciences, Nara Japan, 2Department of Internal Medicine, University of Texas Southwestern Medical Center, Dallas, TX, 3Institute for Exercise and Environmental Medicine, Texas Health Presbyterian Hospital of Dallas, TX TABLE OF CONTENTS 1. Abstract 2. Introduction and historical perspective 3. Neural pathway from the brain to sweat gland 4. Non-thermal modulators of sweat rate 4.1. Effect of exercise in modulating sweat rate 4.2. Effect of baroreceptors in modulating sweat rate 4.3. Effect of body fluid status and osmolality on sweat rate 5. Summary 6. Acknowledgement 7. References 1. ABSTRACT 2. INTRODUCTION AND HISTORICAL PERSPECTIVE Human body temperature is regulated within a very narrow range. When exposed to hyperthermic conditions, via Evaporative heat loss is critical for human survival in environmental factors and/or increased metabolism, heat a hot environment, particularly when environmental dissipation becomes vital for survival. In humans, the temperature is higher than skin temperature. Exercise or primary mechanism of heat dissipation, particularly when exposure to a hot environment elevates internal and skin ambient temperature is higher than skin temperature, is temperatures, and subsequently increases sweat rate and evaporative heat loss secondary to sweat secretion from skin blood flow. Historically it was thought that skin eccrine glands. While the primary controller of sweating is temperature was more important than internal temperature the integration between internal and skin temperatures, a in the control of sweating (24, 109). -

Traumatic Injury to Peripheral Nerves
AAEM MINIMONOGRAPH 28 ABSTRACT: This article reviews the epidemiology and classification of traumatic peripheral nerve injuries, the effects of these injuries on nerve and muscle, and how electrodiagnosis is used to help classify the injury. Mecha- nisms of recovery are also reviewed. Motor and sensory nerve conduction studies, needle electromyography, and other electrophysiological methods are particularly useful for localizing peripheral nerve injuries, detecting and quantifying the degree of axon loss, and contributing toward treatment de- cisions as well as prognostication. © 2000 American Association of Electrodiagnostic Medicine. Published by John Wiley & Sons, Inc. Muscle Nerve 23: 863–873, 2000 TRAUMATIC INJURY TO PERIPHERAL NERVES LAWRENCE R. ROBINSON, MD Department of Rehabilitation Medicine, University of Washington, Seattle, Washington 98195 USA EPIDEMIOLOGY OF PERIPHERAL NERVE TRAUMA company central nervous system trauma, not only Traumatic injury to peripheral nerves results in con- compounding the disability, but making recognition siderable disability across the world. In peacetime, of the peripheral nerve lesion problematic. Of pa- peripheral nerve injuries commonly result from tients with peripheral nerve injuries, about 60% have 30 trauma due to motor vehicle accidents and less com- a traumatic brain injury. Conversely, of those with monly from penetrating trauma, falls, and industrial traumatic brain injury admitted to rehabilitation accidents. Of all patients admitted to Level I trauma units, 10 to 34% have associated peripheral nerve 7,14,39 centers, it is estimated that roughly 2 to 3% have injuries. It is often easy to miss peripheral nerve peripheral nerve injuries.30,36 If plexus and root in- injuries in the setting of central nervous system juries are also included, the incidence is about 5%.30 trauma. -

Peripheral Nerve Injury: Principles for Repair and Regeneration M.F
Send Orders for Reprints to [email protected] The Open Orthopaedics Journal, 2014, 8, (Suppl 1: M10) 199-203 199 Open Access Peripheral Nerve Injury: Principles for Repair and Regeneration M.F. Griffin1, M. Malahias1, S. Hindocha*,2 and Wasim S. Khan3 1Plastic Surgery Department, Good Hope Hospital, West Midlands, B75 7RR, UK 2Plastic Surgery Department, Whiston Hospital, Liverpool, L35 5DR, UK 3University College London Institute of Orthopaedics & Musculoskeletal Sciences, Royal National Orthopaedic Hospital, Stanmore, London, HA7 4LP, UK Abstract: Peripheral Nerve Injuries are one of the most common causes of hand dysfunction caused by upper limb trauma but still current management has remained suboptimal. This review aims to explain the traditional view of pathophysiology of nerve repair and also describe why surgical management is still inadequate in using the new biological research that has documented the changes that occur after the nerve injury, which, could cause suboptimal clinical outcomes. Subsequently presentation and diagnosis will be described for peripheral nerve injuries. When traditional surgical repair using end-to-end anastomosis is not adequate nerve conduits are required with the gold standard being the autologous nerve. Due to associated donor site morbidity and poor functional outcome documented with autologous nerve repair several new advancements for alternatives to bridge the gap are being investigated. We will summarise the new and future advancements of non-biological and biological replacements as well as gene therapy, which are being considered as the alternatives for peripheral nerve repair. Keywords: Anastamosis, biological replacements, clinical outcome, nerve repair, peripheral nerves. INTRODUCTION perineurium; which contributes to nerve strength and maintains the intra-fascicular pressure. -

Development of a Functional in Vitro 3D Model of the Peripheral Nerve
University of Central Florida STARS Electronic Theses and Dissertations, 2004-2019 2018 Development of a Functional In Vitro 3D Model of the Peripheral Nerve Wesley Anderson University of Central Florida Part of the Disease Modeling Commons Find similar works at: https://stars.library.ucf.edu/etd University of Central Florida Libraries http://library.ucf.edu This Doctoral Dissertation (Open Access) is brought to you for free and open access by STARS. It has been accepted for inclusion in Electronic Theses and Dissertations, 2004-2019 by an authorized administrator of STARS. For more information, please contact [email protected]. STARS Citation Anderson, Wesley, "Development of a Functional In Vitro 3D Model of the Peripheral Nerve" (2018). Electronic Theses and Dissertations, 2004-2019. 5946. https://stars.library.ucf.edu/etd/5946 DEVELOPMENT OF A FUNCTIONAL IN VITRO 3D MODEL OF THE PERIPHERAL NERVE by WESLEY ALLEN ANDERSON B.S. UNIVERSITY OF CENTRAL FLORIDA, 2011 M.S. UNIVERSITY OF CENTRAL FLORIDA, 2013 A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy in the Burnett School of Biomedical Sciences in the College of Medicine at the University of Central Florida Orlando, Florida Summer Term 2018 Major Professor: Stephen Lambert © 2018 Wesley Anderson ii ABSTRACT Peripheral neuropathies, affect approximately 20 million people in the United States and are often a complication of conditions such as diabetes that can result in amputation of affected areas such as the feet and toes. In vitro methodologies to facilitate the understanding and treatment of these disorders often lack the cellular and functional complexity required to accurately model peripheral neuropathies. -

How Does the Brain Produce Movement?
p CHAPTER 10 How Does the Brain Produce Movement? The Hierarchical Control The Basal Ganglia and of Movement the Cerebellum The Forebrain and Movement Initiation The Basal Ganglia and Movement Force The Brainstem and Species-Typical Movement Focus on Disorders: Tourette’s Syndrome Focus on Disorders: Autism The Cerebellum and Movement Skill The Spinal Cord and Movement Execution Focus on Disorders: Paraplegia The Organization of the Somatosensory System The Organization of the Somatosensory Receptors and Sensory Perception Motor System Dorsal-Root Ganglion Neurons The Motor Cortex The Somatosensory Pathways to the Brain The Corticospinal Tracts Spinal-Cord Responses to Somatosensory Input The Motor Neurons The Vestibular System and Balance The Control of Muscles Exploring the Somatosensory The Motor Cortex and Skilled System Movements The Somatosensory Homunculus Investigating Neural Control of Skilled Movements The Effects of Damage to the Somatosensory Cortex The Control of Skilled Movements in Other Species The Somatosensory Cortex and Complex How Motor Cortex Damage Affects Skilled Movement Movements Kevork Djansezian/AP Photo Micrograph: Dr. David Scott/Phototake 354 I p amala is a female Indian elephant that lives at the In one way, however, Kamala uses this versatile trunk zoo in Calgary, Canada. Her trunk, which is really very unusually for an elephant (Onodera & Hicks, 1999). K just a greatly extended upper lip and nose, con- She is one of only a few elephants in the world that paints sists of about 2000 fused muscles. A pair of nostrils runs its with its trunk (Figure 10-1). Like many artists, she paints length and fingerlike projections are located at its tip. -

Fascicular Anatomy of Human Femoral Nerve: Implications for Neural Prostheses Using Nerve Cuff Electrodes
Volume 46, Number 7, 2009 JRRDJRRD Pages 973–984 Journal of Rehabilitation Research & Development Fascicular anatomy of human femoral nerve: Implications for neural prostheses using nerve cuff electrodes Kenneth J. Gustafson, PhD;1–2* Gilles C. J. Pinault, MD;2–3 Jennifer J. Neville, MD;4 Ishaq Syed, MD;4 John A. Davis Jr, MD;5 Jesse Jean-Claude, MD;2–3 Ronald J. Triolo, PhD1–2,5 1Department of Biomedical Engineering, Case Western Reserve University, Cleveland, OH; 2Louis Stokes Cleveland Department of Veterans Affairs Medical Center, Cleveland, OH; 3Department of Surgery, 4School of Medicine, and 5Department of Orthopedics, Case Western Reserve University, Cleveland, OH Abstract—Clinical interventions to restore standing or stepping ing or walking after paralysis resulting from upper motor by using nerve cuff stimulation require a detailed knowledge of neuron damage secondary to spinal cord injury (SCI), or femoral nerve neuroanatomy. We harvested eight femoral nerves peripheral nerve damage due to trauma, require a detailed with all distal branches and characterized the branching patterns knowledge of the morphology and fascicular anatomy of the and diameters. The fascicular representation of each distal nerve femoral nerve. However, the fascicular anatomy and spe- was identified and traced proximally to create fascicle maps of the cific dimensions of the human femoral nerve have not been compound femoral nerve in four cadaver specimens. Distal nerves fully described and must be quantitatively documented. were consistently represented as individual fascicles or distinct groups of fascicles in the compound femoral nerve. Branch-free The femoral nerve originates from the second, third, length of the compound femoral nerve was 1.50 +/– 0.47 cm and fourth lumbar spinal nerves and innervates the anterior (mean +/– standard deviation).