Dissection and Exposure of the Whole Course of Deep Nerves in Human Head Specimens After Decalcification
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Level of Superior Colliculus ° Edinger- Westphal Nucleus ° Pretectal Nucleus: Close to the Lateral Part of the Superior Colliculus
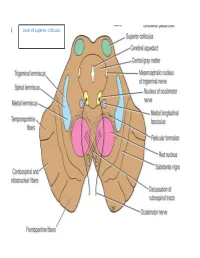
Level of superior colliculus ° Edinger- Westphal nucleus ° pretectal nucleus: close to the lateral part of the superior colliculus. Red nucleus • Rounded mass of gray matter • Situated bt cerebral aqueduct and substantia nigra • Reddish blue(vascularity & iron containing pigment) • Afferents from: cerebral cortex,cerebellum,substa ntia nigra, thalamic nuclei, spinal cord • Efferent to: spinal cord, reticular formation. thalamus and substantia nigra • involved in motor coordination. Crus cerebri • Corticospinal & corticonuclear fibers (middle) • Frontopontine fibers (medial) • Temporopontine fibers (lateral) these descending tracts connect the cerebral cortex with spinal cord, cranial nerves nuclei, pons & cerebellum Level at superior colliculus ° Superior colliculus ° Occulomotor nucleus (posterior to MLF) ° Occulomotor n emerges through red nucleus ° Edinger-Westphal nucleus ° pretectal nucleus: close to the lateral part of the superior colliculus. ° MLF ° Medial , trigeminal, spinal leminiscus ( no lateral leminiscus) ° Red nucleus ° Substantia nigra ° Crus cerebri ° RF Substantia nigra ° Large motor nucleus ° is a brain structure located in the midbrain ° plays an important role in reward, addiction, and movement. ° Substantia nigra is Latin for "black substance" due to high levels of melanin ° has connections with basal ganglia ,cerebral cortex ° Concerned with muscle tone ° Parkinson's disease is caused by the death of neurons in the substantia nigra Oculomotor Nerve (III) • Main oculomotor nucleus • Accessory parasympathetic nucleus -

The Anatomic Analysis of the Vidian Canal and the Surrounding
Braz J Otorhinolaryngol. 2019;85(2):136---143 Brazilian Journal of OTORHINOLARYNGOLOGY www.bjorl.org ORIGINAL ARTICLE The anatomic analysis of the vidian canal and the surrounding structures concerning vidian neurectomy ଝ using computed tomography scans a,∗ a b Gülay Ac¸ar , Aynur Emine C¸ic¸ekcibas¸ı , ˙Ibrahim C¸ukurova , c a d Kemal Emre Özen , Muzaffer ¸ekerS , ˙Ibrahim Güler a Necmettin Erbakan University, Meram Faculty of Medicine, Department of Anatomy, Konya, Turkey b Health Sciences University, Izmir Tepecik Trainig and Research Hospital, Department of Otolaryngology-Head and Neck Surgery, Izmir, Turkey c Katip C¸elebi University, Faculty of Medicine, Department of Anatomy, Izmir, Turkey d Selcuk University, Faculty of Medicine, Department of Radiology, Konya, Turkey Received 15 September 2017; accepted 8 November 2017 Available online 26 December 2017 KEYWORDS Abstract Intrasphenoid Introduction: The type of endoscopic approach chosen for vidian neurectomy can be specified septum; by evaluating the vidian canal and the surrounding sphenoid sinus structures. Morphometric Objective: The variations and morphometry of the vidian canal were investigated, focusing on analysis; the functional correlations between them which are crucial anatomical landmarks for preoper- Pterygoid process ative planning. pneumatization; Methods: This study was performed using paranasal multidetector computed tomography Vidian canal; images that were obtained with a section thickening of 0.625 mm of 250 adults. Vidian neurectomy Results: The distributions of 500 vidian canal variants were categorized as follows; Type 1, within the sphenoid corpus (55.6%); Type 2, partially protruding into the sphenoid sinus (34.8%); Type 3, within the sphenoid sinus (9.6%). The pneumatization of the pterygoid process is mostly seen in vidian canal Type 2 (72.4%) and Type 3 (95.8%) (p < 0.001). -

Morfofunctional Structure of the Skull
N.L. Svintsytska V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 Ministry of Public Health of Ukraine Public Institution «Central Methodological Office for Higher Medical Education of MPH of Ukraine» Higher State Educational Establishment of Ukraine «Ukranian Medical Stomatological Academy» N.L. Svintsytska, V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 2 LBC 28.706 UDC 611.714/716 S 24 «Recommended by the Ministry of Health of Ukraine as textbook for English- speaking students of higher educational institutions of the MPH of Ukraine» (minutes of the meeting of the Commission for the organization of training and methodical literature for the persons enrolled in higher medical (pharmaceutical) educational establishments of postgraduate education MPH of Ukraine, from 02.06.2016 №2). Letter of the MPH of Ukraine of 11.07.2016 № 08.01-30/17321 Composed by: N.L. Svintsytska, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor V.H. Hryn, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor This textbook is intended for undergraduate, postgraduate students and continuing education of health care professionals in a variety of clinical disciplines (medicine, pediatrics, dentistry) as it includes the basic concepts of human anatomy of the skull in adults and newborns. Rewiewed by: O.M. Slobodian, Head of the Department of Anatomy, Topographic Anatomy and Operative Surgery of Higher State Educational Establishment of Ukraine «Bukovinian State Medical University», Doctor of Medical Sciences, Professor M.V. -
1A. Internal Auditory Meatus
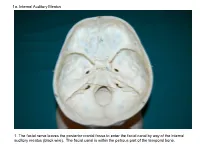
1a. Internal Auditory Meatus 1. The facial nerve leaves the posterior cranial fossa to enter the facial canal by way of the internal auditory meatus (black wire). The facial canal is within the petrous part of the temporal bone. 1b. Internal Auditory Meatus The facial nerve leaves the posterior cranial fossa to enter the facial canal by way of the internal auditory meatus (black wire). 2. Hiatus of the Canal and Groove for the Greater Superficial Petrosal Nerve The greater superficial petrosal nerve leaves the facial canal to enter the middle cranial fossa by way of the hiatus of the canal for the greater superficial petrosal nerve (black wire). 3. Pterygoid Canal at Anterior Lip of the Lacerate Foramen The greater superficial petrosal nerve is joined by the deep petrosal nerve to form the nerve of the pterygoid canal (black and red wire). This nerve leaves the middle cranial fossa to enter the pterygopalatine fossa by way of the pterygoid canal. The posterior opening of the pterygoid canal is at the anterior lip of the lacerate foramen. The greater superficial nerve and the deep petrosal nerve travel within the cavernous sinus. 4. Pterygopalatine Fossa Seen Through the Pterygomaxillary Fissure The anterior opening of the pterygoid canal is into the pterygopalatine fossa (black wire). The pterygopalatine fossa is located medial to the pterygomaxillary fissure and contains the pterygopalatine ganglion. 5. External Auditory Meatus The chorda tympani nerve leaves the facial canal and crosses the middle ear (black wire). It then leaves the middle ear to arrive in the infratemporal fossa by way of the petrotympanic fissure. -

Atlas of the Facial Nerve and Related Structures
Rhoton Yoshioka Atlas of the Facial Nerve Unique Atlas Opens Window and Related Structures Into Facial Nerve Anatomy… Atlas of the Facial Nerve and Related Structures and Related Nerve Facial of the Atlas “His meticulous methods of anatomical dissection and microsurgical techniques helped transform the primitive specialty of neurosurgery into the magnificent surgical discipline that it is today.”— Nobutaka Yoshioka American Association of Neurological Surgeons. Albert L. Rhoton, Jr. Nobutaka Yoshioka, MD, PhD and Albert L. Rhoton, Jr., MD have created an anatomical atlas of astounding precision. An unparalleled teaching tool, this atlas opens a unique window into the anatomical intricacies of complex facial nerves and related structures. An internationally renowned author, educator, brain anatomist, and neurosurgeon, Dr. Rhoton is regarded by colleagues as one of the fathers of modern microscopic neurosurgery. Dr. Yoshioka, an esteemed craniofacial reconstructive surgeon in Japan, mastered this precise dissection technique while undertaking a fellowship at Dr. Rhoton’s microanatomy lab, writing in the preface that within such precision images lies potential for surgical innovation. Special Features • Exquisite color photographs, prepared from carefully dissected latex injected cadavers, reveal anatomy layer by layer with remarkable detail and clarity • An added highlight, 3-D versions of these extraordinary images, are available online in the Thieme MediaCenter • Major sections include intracranial region and skull, upper facial and midfacial region, and lower facial and posterolateral neck region Organized by region, each layered dissection elucidates specific nerves and structures with pinpoint accuracy, providing the clinician with in-depth anatomical insights. Precise clinical explanations accompany each photograph. In tandem, the images and text provide an excellent foundation for understanding the nerves and structures impacted by neurosurgical-related pathologies as well as other conditions and injuries. -

Dissection and Exposure of the Whole Course of Deep Nerves in Human Head Specimens After Decalcification
Hindawi Publishing Corporation International Journal of Otolaryngology Volume 2012, Article ID 418650, 7 pages doi:10.1155/2012/418650 Research Article Dissection and Exposure of the Whole Course of Deep Nerves in Human Head Specimens after Decalcification Longping Liu, Robin Arnold, and Marcus Robinson Discipline of Anatomy and Histology, University of Sydney, Anderson Stuart Building F13, Sydney, NSW 2006, Australia Correspondence should be addressed to Marcus Robinson, [email protected] Received 29 July 2011; Revised 10 November 2011; Accepted 12 December 2011 AcademicEditor:R.L.Doty Copyright © 2012 Longping Liu et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. The whole course of the chorda tympani nerve, nerve of pterygoid canal, and facial nerves and their relationships with surrounding structures are complex. After reviewing the literature, it was found that details of the whole course of these deep nerves are rarely reported and specimens displaying these nerves are rarely seen in the dissecting room, anatomical museum, or atlases. Dissections were performed on 16 decalcified human head specimens, exposing the chorda tympani and the nerve connection between the geniculate and pterygopalatine ganglia. Measurements of nerve lengths, branching distances, and ganglia size were taken. The chorda tympani is a very fine nerve (0.44 mm in diameter within the tympanic cavity) and approximately 54 mm in length. The mean length of the facial nerve from opening of internal acoustic meatus to stylomastoid foramen was 52.5 mm. -

NEUROANATOMY of the VISUAL PATHWAYS Magrane Basic Science Course June 2018
NEUROANATOMY OF THE VISUAL PATHWAYS Magrane Basic Science Course June 2018 **It is important for me to acknowledge the extensive input from Dr. Lola Hudson and Dr. Karen Munana to both these notes and the Power Point presentation.** CENTRAL NERVOUS SYSTEM All 5 divisions of the brain are involved with ocular function and/or adnexa in either conscious pathways or reflex pathways. The 5 divisions are the telencephalon (cerebral hemispheres), diencephalon (thalamus, hypothalamus), mesencephalon (midbrain), metencephalon (cerebellum and pons) and myelencephalon (medulla oblongata). The telencephalon and diencephalon together can be referred to as the prosencephalon (forebrain), and the metencephalon and myelencephalon can be referred to as the rhombencephalon (hindbrain). These 3 larger divisions (prosencephalon, mesencephalon and rhombencephalon) relate to the embryology of the brain from three original neural tube vesicles. The more cranial spinal cord is also involved with ocular function through sensory innervation into the cervical spinal cord and through sympathetic autonomic function particularly in the cranial thoracic spinal cord. PERIPHERAL NERVOUS SYSTEM The majority of the 12 pairs of cranial nerves (CN) have some involvement with ocular function: CNs II, III, IV, V (ophthalmic and maxillary branches), VI, VII and VIII including appropriate sensory and autonomic ganglia of these CNs. TELENCEPHALON (cerebrum=cerebral hemispheres=cerebral cortex) Telencephalon is the site of awareness, initiation of voluntary movements and perception of stimuli. The cerebrum functions in perception and integration of vision as well as voluntary control of eye/eyelid movements. The occipital lobes and the motor cortex of the frontal/parietal lobes are the primary regions involved in ocular and eyelid function. -

Clinical Anatomy of Greater Petrosal Nerve and Its Surgical Importance
[Downloaded free from http://www.indianjotol.org on Monday, August 18, 2014, IP: 218.241.189.21] || Click here to download free Android application for this journal ORIGINAL ARTICLE Clinical anatomy of greater petrosal nerve and its surgical importance Prashant E Natekar, Fatima M De Souza Department of Anatomy, Goa Medical College, Bambolim, Goa, India Background: Surgical approach towards greater petrosal nerve has to be done with caution as many surgeons ABSTRACT are unfamiliar with the anatomy of the facial nerve. The anatomical landmarks selected must be reliable and above all easy to identify for identification of the greater petrosal nerve so as to avoid injury to the structures in the middle cranial fossa. Observation and Results: The present study is carried out on 100 temporal bones by examining the following measurements of the right and the left sides a) length of the hiatus for grater petrosal superficial nerve b) distance from superior petrosal sinus c) distance from lateral margin of middle cranial fossa d) arcuate eminence and e) distance from exit to the foramen ovale. Conclusion: The anatomical landmarks selected must be reliable and above all easy to identify. Bony structures are more suitable than soft tissue or cartilaginous landmarks because of their rigid and reliable location. These anatomical landmarks will definitely help the surgeon while performing vidian nerve neurectomy and also the anatomical relationship of the facial nerve in temporal bone. The middle fossa approach involves a temporal craniotomy in cases of perineural spread of adenoid cystic carcinomas hence these anatomical landmarks will serve as useful guide for the surgeons and radiologists. -

NASAL ANATOMY Elena Rizzo Riera R1 ORL HUSE NASAL ANATOMY
NASAL ANATOMY Elena Rizzo Riera R1 ORL HUSE NASAL ANATOMY The nose is a highly contoured pyramidal structure situated centrally in the face and it is composed by: ü Skin ü Mucosa ü Bone ü Cartilage ü Supporting tissue Topographic analysis 1. EXTERNAL NASAL ANATOMY § Skin § Soft tissue § Muscles § Blood vessels § Nerves ² Understanding variations in skin thickness is an essential aspect of reconstructive nasal surgery. ² Familiarity with blood supplyà local flaps. Individuality SKIN Aesthetic regions Thinner Thicker Ø Dorsum Ø Radix Ø Nostril margins Ø Nasal tip Ø Columella Ø Alae Surgical implications Surgical elevation of the nasal skin should be done in the plane just superficial to the underlying bony and cartilaginous nasal skeleton to prevent injury to the blood supply and to the nasal muscles. Excessive damage to the nasal muscles causes unwanted immobility of the nose during facial expression, so called mummified nose. SUBCUTANEOUS LAYER § Superficial fatty panniculus Adipose tissue and vertical fibres between deep dermis and fibromuscular layer. § Fibromuscular layer Nasal musculature and nasal SMAS § Deep fatty layer Contains the major superficial blood vessels and nerves. No fibrous fibres. § Periosteum/ perichondrium Provide nutrient blood flow to the nasal bones and cartilage MUSCLES § Greatest concentration of musclesàjunction of upper lateral and alar cartilages (muscular dilation and stenting of nasal valve). § Innervation: zygomaticotemporal branch of the facial nerve § Elevator muscles § Depressor muscles § Compressor -

Lecture 7 Anatomy the PTERYGOPALATINE FOSSA
د.احمد فاضل القيسي Lecture 7 Anatomy THE PTERYGOPALATINE FOSSA The pterygopalatine fossa lies beneath the posterior surface of the maxilla and the pterygoid process of the sphenoid bone. The pterygopalatine fossa contains the maxillary nerve, the maxillary artery (third part) and the pterygopalatine parasympathetic ganglion. Boundaries Anteriorly: posterior surface of maxilla. Posteriorly: anterior margin of pterygoid process below and greater wing of sphenoid above. Medially: perpendicular plate of palatine bone. Superiorly: greater wing of sphenoid. Laterally: communicates with infratemporal fossa through pterygomaxillary fissure Communications and openings: 1. The pterygomaxillary fissure: transmits the maxillary artery from the infratemporal fossa, the posterior superior alveolar branches of the maxillary division of the trigeminal nerve and the sphenopalatine veins. 2. The inferior orbital fissure: transmits the infraorbital and zygomatic branches of the maxillary nerve, the orbital branches of the pterygopalatine ganglion and the infraorbital vessels. 3. The foramen rotundum from the middle cranial fossa, occupying the greater wing of the sphenoid bone and transmit the maxillary division of the trigeminal nerve 4. The pterygoid canal from the region of the foramen lacerum at the base of the skull. The pterygoid canal transmits the greater petrosal and deep petrosal nerves (which combine to form the nerve of the pterygoid canal) and an accompanying artery derived from the maxillary artery. 5. The sphenopalatine foramen lying high up on the medial wall of the fossa.This foramen communicates with the lateral wall of the nasal cavity. It transmits the nasopalatine and posterior superior nasal nerves (from the pterygopalatine ganglion) and the sphenopalatine vessels. 6. The opening of a palatine canal found at the base of the fossa. -

The Radiology of the Pterygoid Canal: Normal and Pathologic Findings
479 The Radiology of the Pterygoid Canal: Normal and Pathologic Findings I. Pandolfo 1 To better define the normal anatomy and pathologic features of the pterygoid canal, M. Gaeta 100 normal subjects and 38 patients with disease of the parana sal sinuses, nasopharynx, A. Blandino and base of the skull were studied with pluridirectional tomography. Particular attention M. Longo was given to the normal radiographic appearance of the pterygoid canal as well as to its anatomic variants and its relationship to the paranasal sinuses. Three radiographic signs of involvement of the pterygoid canal were detected: disappearance, enlargement, and narrowing. Moreover, a brief correlation between pluridirectional tomography and CT was made. Diagnostic accuracy in evaluating the bony lesions is the same with both techniques, but CT is superior to pluridirectional tomography in evaluating involvement of the soft tissues. The gross anatomy of the pterygoid or vidian canal has been well described in a fundamental paper by Radoievitch and Jovanovitch [1]. In the radiologic literature, conversely, there are few reports on this topic [2]. The purpose of this study was to carry out a detailed analysis of the normal radiographic anatomy and the most common pathologic appearances of the pterygoid canal. The pterygoid canal is a straight or curvilinear bony duct situated between the pterygoid process and the sphenoid sinus. It is directed forward and medially and connects the foramen lacerum with the pterygopalatine fossa [1 , 2]. The width of the canal is variable because the canal widens as it extends forward (Fig . 1). In fact, the average width of its anterior opening is 2.5 mm , versus 1 mm for the posterior opening. -

Casper Ryan Thesis.Pdf (10.61Mb)
Development of a 3D Learning Resource of the Pterygopalatine Fossa Using Cone Beam Computed Tomography For Dental Students By Ryan James Casper A THESIS Submitted to the Faculty of the Graduate School in partial fulfillment of the requirements for the Degree of Master of Science in the Department of Oral Biology Omaha, Nebraska April 25th 2012 Abstract The pterygopalatine fossa is a pyramidal shaped fossa located between the infratemporal fossa and the nasal cavity. The major contents include the maxillary division of the trigeminal nerve, the pterygopalatine ganglion, and branches of the 3rd part of the maxillary artery. The fossa is very difficult for students to visualize in textbooks and the gross laboratory. The increasing use of cone beam computed tomography (CBCT) in dentistry has increased the ability of dental clinicians to visualize anatomical structures in multiple dimensions. The purpose of this study was to develop a 3D learning resource of the pterygopalatine fossa using CBCT for dental students. Anonymized CBCT files were selected from a series of patients with normal anatomy. All of the scans had been performed at 0.3 mm resolution and were reconstructed using Osirix version 3.9.2 in axial, coronal, and sagittal planes. Digital images of a dry skull specimen and cadaveric dissection of the pterygopalatine fossa were collected using a Canon Powershot ELPH 100 HS. Final Cut version 10.0 was used to create a multimedia learning resource. A multimedia learning resource for the pterygopalatine fossa was created using CBCT videos, CBCT images, cadaver photographs, and skull photographs. The CBCT videos and images incorporated axial, sagittal, and coronal planes of the pterygopalatine fossa.