The Radiology of the Pterygoid Canal: Normal and Pathologic Findings
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Anatomic Analysis of the Vidian Canal and the Surrounding
Braz J Otorhinolaryngol. 2019;85(2):136---143 Brazilian Journal of OTORHINOLARYNGOLOGY www.bjorl.org ORIGINAL ARTICLE The anatomic analysis of the vidian canal and the surrounding structures concerning vidian neurectomy ଝ using computed tomography scans a,∗ a b Gülay Ac¸ar , Aynur Emine C¸ic¸ekcibas¸ı , ˙Ibrahim C¸ukurova , c a d Kemal Emre Özen , Muzaffer ¸ekerS , ˙Ibrahim Güler a Necmettin Erbakan University, Meram Faculty of Medicine, Department of Anatomy, Konya, Turkey b Health Sciences University, Izmir Tepecik Trainig and Research Hospital, Department of Otolaryngology-Head and Neck Surgery, Izmir, Turkey c Katip C¸elebi University, Faculty of Medicine, Department of Anatomy, Izmir, Turkey d Selcuk University, Faculty of Medicine, Department of Radiology, Konya, Turkey Received 15 September 2017; accepted 8 November 2017 Available online 26 December 2017 KEYWORDS Abstract Intrasphenoid Introduction: The type of endoscopic approach chosen for vidian neurectomy can be specified septum; by evaluating the vidian canal and the surrounding sphenoid sinus structures. Morphometric Objective: The variations and morphometry of the vidian canal were investigated, focusing on analysis; the functional correlations between them which are crucial anatomical landmarks for preoper- Pterygoid process ative planning. pneumatization; Methods: This study was performed using paranasal multidetector computed tomography Vidian canal; images that were obtained with a section thickening of 0.625 mm of 250 adults. Vidian neurectomy Results: The distributions of 500 vidian canal variants were categorized as follows; Type 1, within the sphenoid corpus (55.6%); Type 2, partially protruding into the sphenoid sinus (34.8%); Type 3, within the sphenoid sinus (9.6%). The pneumatization of the pterygoid process is mostly seen in vidian canal Type 2 (72.4%) and Type 3 (95.8%) (p < 0.001). -

Morfofunctional Structure of the Skull
N.L. Svintsytska V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 Ministry of Public Health of Ukraine Public Institution «Central Methodological Office for Higher Medical Education of MPH of Ukraine» Higher State Educational Establishment of Ukraine «Ukranian Medical Stomatological Academy» N.L. Svintsytska, V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 2 LBC 28.706 UDC 611.714/716 S 24 «Recommended by the Ministry of Health of Ukraine as textbook for English- speaking students of higher educational institutions of the MPH of Ukraine» (minutes of the meeting of the Commission for the organization of training and methodical literature for the persons enrolled in higher medical (pharmaceutical) educational establishments of postgraduate education MPH of Ukraine, from 02.06.2016 №2). Letter of the MPH of Ukraine of 11.07.2016 № 08.01-30/17321 Composed by: N.L. Svintsytska, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor V.H. Hryn, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor This textbook is intended for undergraduate, postgraduate students and continuing education of health care professionals in a variety of clinical disciplines (medicine, pediatrics, dentistry) as it includes the basic concepts of human anatomy of the skull in adults and newborns. Rewiewed by: O.M. Slobodian, Head of the Department of Anatomy, Topographic Anatomy and Operative Surgery of Higher State Educational Establishment of Ukraine «Bukovinian State Medical University», Doctor of Medical Sciences, Professor M.V. -
1A. Internal Auditory Meatus
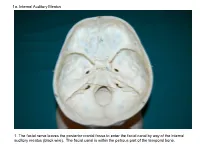
1a. Internal Auditory Meatus 1. The facial nerve leaves the posterior cranial fossa to enter the facial canal by way of the internal auditory meatus (black wire). The facial canal is within the petrous part of the temporal bone. 1b. Internal Auditory Meatus The facial nerve leaves the posterior cranial fossa to enter the facial canal by way of the internal auditory meatus (black wire). 2. Hiatus of the Canal and Groove for the Greater Superficial Petrosal Nerve The greater superficial petrosal nerve leaves the facial canal to enter the middle cranial fossa by way of the hiatus of the canal for the greater superficial petrosal nerve (black wire). 3. Pterygoid Canal at Anterior Lip of the Lacerate Foramen The greater superficial petrosal nerve is joined by the deep petrosal nerve to form the nerve of the pterygoid canal (black and red wire). This nerve leaves the middle cranial fossa to enter the pterygopalatine fossa by way of the pterygoid canal. The posterior opening of the pterygoid canal is at the anterior lip of the lacerate foramen. The greater superficial nerve and the deep petrosal nerve travel within the cavernous sinus. 4. Pterygopalatine Fossa Seen Through the Pterygomaxillary Fissure The anterior opening of the pterygoid canal is into the pterygopalatine fossa (black wire). The pterygopalatine fossa is located medial to the pterygomaxillary fissure and contains the pterygopalatine ganglion. 5. External Auditory Meatus The chorda tympani nerve leaves the facial canal and crosses the middle ear (black wire). It then leaves the middle ear to arrive in the infratemporal fossa by way of the petrotympanic fissure. -

Dissection and Exposure of the Whole Course of Deep Nerves in Human Head Specimens After Decalcification
Hindawi Publishing Corporation International Journal of Otolaryngology Volume 2012, Article ID 418650, 7 pages doi:10.1155/2012/418650 Research Article Dissection and Exposure of the Whole Course of Deep Nerves in Human Head Specimens after Decalcification Longping Liu, Robin Arnold, and Marcus Robinson Discipline of Anatomy and Histology, University of Sydney, Anderson Stuart Building F13, Sydney, NSW 2006, Australia Correspondence should be addressed to Marcus Robinson, [email protected] Received 29 July 2011; Revised 10 November 2011; Accepted 12 December 2011 AcademicEditor:R.L.Doty Copyright © 2012 Longping Liu et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. The whole course of the chorda tympani nerve, nerve of pterygoid canal, and facial nerves and their relationships with surrounding structures are complex. After reviewing the literature, it was found that details of the whole course of these deep nerves are rarely reported and specimens displaying these nerves are rarely seen in the dissecting room, anatomical museum, or atlases. Dissections were performed on 16 decalcified human head specimens, exposing the chorda tympani and the nerve connection between the geniculate and pterygopalatine ganglia. Measurements of nerve lengths, branching distances, and ganglia size were taken. The chorda tympani is a very fine nerve (0.44 mm in diameter within the tympanic cavity) and approximately 54 mm in length. The mean length of the facial nerve from opening of internal acoustic meatus to stylomastoid foramen was 52.5 mm. -

Atlas of the Facial Nerve and Related Structures
Rhoton Yoshioka Atlas of the Facial Nerve Unique Atlas Opens Window and Related Structures Into Facial Nerve Anatomy… Atlas of the Facial Nerve and Related Structures and Related Nerve Facial of the Atlas “His meticulous methods of anatomical dissection and microsurgical techniques helped transform the primitive specialty of neurosurgery into the magnificent surgical discipline that it is today.”— Nobutaka Yoshioka American Association of Neurological Surgeons. Albert L. Rhoton, Jr. Nobutaka Yoshioka, MD, PhD and Albert L. Rhoton, Jr., MD have created an anatomical atlas of astounding precision. An unparalleled teaching tool, this atlas opens a unique window into the anatomical intricacies of complex facial nerves and related structures. An internationally renowned author, educator, brain anatomist, and neurosurgeon, Dr. Rhoton is regarded by colleagues as one of the fathers of modern microscopic neurosurgery. Dr. Yoshioka, an esteemed craniofacial reconstructive surgeon in Japan, mastered this precise dissection technique while undertaking a fellowship at Dr. Rhoton’s microanatomy lab, writing in the preface that within such precision images lies potential for surgical innovation. Special Features • Exquisite color photographs, prepared from carefully dissected latex injected cadavers, reveal anatomy layer by layer with remarkable detail and clarity • An added highlight, 3-D versions of these extraordinary images, are available online in the Thieme MediaCenter • Major sections include intracranial region and skull, upper facial and midfacial region, and lower facial and posterolateral neck region Organized by region, each layered dissection elucidates specific nerves and structures with pinpoint accuracy, providing the clinician with in-depth anatomical insights. Precise clinical explanations accompany each photograph. In tandem, the images and text provide an excellent foundation for understanding the nerves and structures impacted by neurosurgical-related pathologies as well as other conditions and injuries. -

Dissection and Exposure of the Whole Course of Deep Nerves in Human Head Specimens After Decalcification
Hindawi Publishing Corporation International Journal of Otolaryngology Volume 2012, Article ID 418650, 7 pages doi:10.1155/2012/418650 Research Article Dissection and Exposure of the Whole Course of Deep Nerves in Human Head Specimens after Decalcification Longping Liu, Robin Arnold, and Marcus Robinson Discipline of Anatomy and Histology, University of Sydney, Anderson Stuart Building F13, Sydney, NSW 2006, Australia Correspondence should be addressed to Marcus Robinson, [email protected] Received 29 July 2011; Revised 10 November 2011; Accepted 12 December 2011 AcademicEditor:R.L.Doty Copyright © 2012 Longping Liu et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. The whole course of the chorda tympani nerve, nerve of pterygoid canal, and facial nerves and their relationships with surrounding structures are complex. After reviewing the literature, it was found that details of the whole course of these deep nerves are rarely reported and specimens displaying these nerves are rarely seen in the dissecting room, anatomical museum, or atlases. Dissections were performed on 16 decalcified human head specimens, exposing the chorda tympani and the nerve connection between the geniculate and pterygopalatine ganglia. Measurements of nerve lengths, branching distances, and ganglia size were taken. The chorda tympani is a very fine nerve (0.44 mm in diameter within the tympanic cavity) and approximately 54 mm in length. The mean length of the facial nerve from opening of internal acoustic meatus to stylomastoid foramen was 52.5 mm. -

Lecture 7 Anatomy the PTERYGOPALATINE FOSSA
د.احمد فاضل القيسي Lecture 7 Anatomy THE PTERYGOPALATINE FOSSA The pterygopalatine fossa lies beneath the posterior surface of the maxilla and the pterygoid process of the sphenoid bone. The pterygopalatine fossa contains the maxillary nerve, the maxillary artery (third part) and the pterygopalatine parasympathetic ganglion. Boundaries Anteriorly: posterior surface of maxilla. Posteriorly: anterior margin of pterygoid process below and greater wing of sphenoid above. Medially: perpendicular plate of palatine bone. Superiorly: greater wing of sphenoid. Laterally: communicates with infratemporal fossa through pterygomaxillary fissure Communications and openings: 1. The pterygomaxillary fissure: transmits the maxillary artery from the infratemporal fossa, the posterior superior alveolar branches of the maxillary division of the trigeminal nerve and the sphenopalatine veins. 2. The inferior orbital fissure: transmits the infraorbital and zygomatic branches of the maxillary nerve, the orbital branches of the pterygopalatine ganglion and the infraorbital vessels. 3. The foramen rotundum from the middle cranial fossa, occupying the greater wing of the sphenoid bone and transmit the maxillary division of the trigeminal nerve 4. The pterygoid canal from the region of the foramen lacerum at the base of the skull. The pterygoid canal transmits the greater petrosal and deep petrosal nerves (which combine to form the nerve of the pterygoid canal) and an accompanying artery derived from the maxillary artery. 5. The sphenopalatine foramen lying high up on the medial wall of the fossa.This foramen communicates with the lateral wall of the nasal cavity. It transmits the nasopalatine and posterior superior nasal nerves (from the pterygopalatine ganglion) and the sphenopalatine vessels. 6. The opening of a palatine canal found at the base of the fossa. -

Casper Ryan Thesis.Pdf (10.61Mb)
Development of a 3D Learning Resource of the Pterygopalatine Fossa Using Cone Beam Computed Tomography For Dental Students By Ryan James Casper A THESIS Submitted to the Faculty of the Graduate School in partial fulfillment of the requirements for the Degree of Master of Science in the Department of Oral Biology Omaha, Nebraska April 25th 2012 Abstract The pterygopalatine fossa is a pyramidal shaped fossa located between the infratemporal fossa and the nasal cavity. The major contents include the maxillary division of the trigeminal nerve, the pterygopalatine ganglion, and branches of the 3rd part of the maxillary artery. The fossa is very difficult for students to visualize in textbooks and the gross laboratory. The increasing use of cone beam computed tomography (CBCT) in dentistry has increased the ability of dental clinicians to visualize anatomical structures in multiple dimensions. The purpose of this study was to develop a 3D learning resource of the pterygopalatine fossa using CBCT for dental students. Anonymized CBCT files were selected from a series of patients with normal anatomy. All of the scans had been performed at 0.3 mm resolution and were reconstructed using Osirix version 3.9.2 in axial, coronal, and sagittal planes. Digital images of a dry skull specimen and cadaveric dissection of the pterygopalatine fossa were collected using a Canon Powershot ELPH 100 HS. Final Cut version 10.0 was used to create a multimedia learning resource. A multimedia learning resource for the pterygopalatine fossa was created using CBCT videos, CBCT images, cadaver photographs, and skull photographs. The CBCT videos and images incorporated axial, sagittal, and coronal planes of the pterygopalatine fossa. -
Craniumcranium
CRANIUMCRANIUM THETHE SKULLSKULL R.R. DrugaDruga InstituteInstitute ofof Anatomy,Anatomy, 2nd2nd andand 1st1st MedicalMedical FacultyFaculty NEUROCRANIUMNEUROCRANIUM SPLANCHNOCRANIUMSPLANCHNOCRANIUM CRANIUM,CRANIUM, THETHE SKULLSKULL II MostMost highlyhighly modifiedmodified regionregion inin thethe axialaxial skeletonskeleton TheThe neurocraniumneurocranium –– developeddeveloped fromfrom aa seriesseries ofof cartilagescartilages ventralventral toto thethe brainbrain (base)(base) FromFrom mesenchymemesenchyme overover thethe domedome ofof thethe headhead (calvaria(calvaria oror calva)calva) CranialCranial cavitycavity SplanchnocraniumSplanchnocranium –– branchialbranchial apparatusapparatus (cartilaginous(cartilaginous elements)elements) havehave beenbeen replacedreplaced byby overlyingoverlying dermaldermal bonesbones BranchialBranchial apparatusapparatus TheThe mandibularmandibular regionregion andand thethe neckneck areare formedformed byby sixsix pairedpaired branchialbranchial archesarches (cart.(cart. barsbars supportingsupporting thethe gillgill apparatus).apparatus). InIn thethe tetrapodstetrapods branchialbranchial archesarches werewere modifiedmodified andand persistpersist inin thethe facialfacial (maxilla,(maxilla, mandibula)mandibula) andand neckneck skeletonskeleton (laryngeal(laryngeal cartilages)cartilages) Derivatives of cartilagines of the branchial arches 1st arch = Meckel cart., mandibula, malleus 2nd arch = Reichert cart., stapes, styloid proc.,stylohyoid lig. 3rd arch = hyoid bone 4th and 6th arch = laryngeal -

Topographic Anatomy of the Head
O. V. Korencov, G. F. Tkach TOPOGRAPHIC ANATOMY OF THE HEAD Study guide Ministry of Education and Science of Ukraine Ministry of Health of Ukraine Sumy State University O. V. Korencov, G. F. Tkach TOPOGRAPHIC ANATOMY OF THE HEAD Study guide Recommended by Academic Council of Sumy State University Sumy Sumy State University 2016 УДК 611.91(075.3) ББК 54.54я73 K66 Reviewers: L. V. Phomina – Doctor of Medical Sciences, Professor of Vinnytsia National Medical University named after M. I. Pirogov; M. V. Pogorelov – Doctor of Medical Sciences, Professor of Sumy State University Recommended for publication by Academic Council of Sumy State University as а study guide (minutes № 5 of 11.02.2016) Korencov O. V. K66 Topographic anatomy of the head : study guide / O. V. Korencov, G. F. Tkach. – Sumy : Sumy State University, 2016. – 81 р. ISBN 978-966-657-607-4 This manual is intended for the students of medical higher educational institutions of IV accreditation level, who study Human Anatomy in the English language. Посібник рекомендований для студентів вищих медичних навчальних закладів IV рівня акредитації, які вивчають анатомію людини англійською мовою. УДК 611.91(075.3) ББК 54.54я73 © Korencov O. V., Tkach G. F., 2016 ISBN 978-966-657-607-4 © Sumy State University, 2016 TOPOGRAPHIC ANATOMY OF THE HEAD The head is subdivided into two following departments: the brain and facialohes. They are shared by line from the glabella to the supraorbital edge along the zygomatic arch to the outer ear canal. The brain part consists of fornix and base of the skull. The fornix is divided into fronto- parieto-occipital region, paired temporal and mastoid area. -

The Foramen Lacerum: Surgical Anatomy and Relevance for Endoscopic Endonasal Approaches
LABORATORY INVESTIGATION J Neurosurg 131:1571–1582, 2019 The foramen lacerum: surgical anatomy and relevance for endoscopic endonasal approaches Wei-Hsin Wang, MD,1,3 Stefan Lieber, MD,1 Roger Neves Mathias, MD,1 Xicai Sun, MD, PhD,1 Paul A. Gardner, MD,1 Carl H. Snyderman, MD, MBA,2 Eric W. Wang, MD,2 and Juan C. Fernandez-Miranda, MD1 1Department of Neurological Surgery, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania; 2Department of Otolaryngology, University of Pittsburgh, Pennsylvania; and 3Department of Neurosurgery, Taipei Veterans General Hospital, School of Medicine, National Yang-Ming University, Taipei, Taiwan OBJECTIVE The foramen lacerum is a relevant skull base structure that has been neglected for many years. From the endoscopic endonasal perspective, the foramen lacerum is a key structure due to its location at the crossroad between the sagittal and coronal planes. The objective of this study was to provide a detailed investigation of the surgical anatomy of the foramen lacerum and its adjacent structures based on anatomical dissections and imaging studies, propose sev- eral relevant key surgical landmarks, and demonstrate the surgical technique for its full exposure with several illustrative cases. METHODS Ten colored silicone-injected anatomical specimens were dissected using a transpterygoid approach to the foramen lacerum region in a stepwise manner. Five similar specimens were used for a comparative transcranial ap- proach. The osseous anatomy was examined in 32 high-resolution multislice CT studies and 1 disarticulated skull. Rep- resentative cases were selected to illustrate the application of the findings. RESULTS The pterygosphenoidal fissure is the synchondrosis between the lacerum process of the pterygoid bone and the floor of the sphenoid bone. -

Extended Endoscopic Endonasal Approach to the Pterygopalatine Fossa: Anatomical Study and Clinical Considerations
Neurosurg Focus 19 (1):E5, 2005 Extended endoscopic endonasal approach to the pterygopalatine fossa: anatomical study and clinical considerations LUIGI M. CAVALLO, M.D., PH.D., ANDREA MESSINA, M.D., PAUL GARDNER, M.D., FELICE ESPOSITO, M.D., AMIN B. KASSAM, M.D., PAOLO CAPPABIANCA, M.D., ENRICO DE DIVITIIS, M.D., AND MANFRED TSCHABITSCHER, M.D. Department of Neurological Sciences, Division of Neurosurgery, Università degli Studi di Napoli Federico II, Naples, Italy; Microsurgical and Endoscopic Anatomy Study Group, University of Vienna, Austria; and Center for Image-Guided and Minimally Invasive Neurosurgery, Department of Neurosurgery, University of Pittsburgh Medical Center-Presbyterian, Pittsburgh, Pennsylvania Object. The pterygopalatine fossa is an area located deep in the skull base. The microsurgical transmaxillary–trans- antral route is usually chosen to remove lesions in this region. The increasing use of the endoscope in sinonasal func- tional surgery has more recently led to the advent of the endoscope for the treatment of tumors located in the pterygo- palatine fossa as well. Methods. An anatomical dissection of three fresh cadaveric heads (six pterygopalatine fossas) and three dried skull base specimens was performed to evaluate the feasibility of the approach and to illustrate the surgical landmarks that are useful for operations in this complex region. The endoscopic endonasal approach allows a wide exposure of the pterygopalatine fossa. Furthermore, with the same access (that is, through the nostril) it is possible to expose regions contiguous with the pterygopalatine fossa, either to visualize more surgical landmarks or to accomplish a better lesion removal. Conclusions. In this anatomical study the endoscopic endonasal approach to the pterygopalatine fossa has been found to be a safe approach for the removal of lesions in this region.