Nigeria National Emergency Action Plan – January 2017
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Nigeria's Constitution of 1999
PDF generated: 26 Aug 2021, 16:42 constituteproject.org Nigeria's Constitution of 1999 This complete constitution has been generated from excerpts of texts from the repository of the Comparative Constitutions Project, and distributed on constituteproject.org. constituteproject.org PDF generated: 26 Aug 2021, 16:42 Table of contents Preamble . 5 Chapter I: General Provisions . 5 Part I: Federal Republic of Nigeria . 5 Part II: Powers of the Federal Republic of Nigeria . 6 Chapter II: Fundamental Objectives and Directive Principles of State Policy . 13 Chapter III: Citizenship . 17 Chapter IV: Fundamental Rights . 20 Chapter V: The Legislature . 28 Part I: National Assembly . 28 A. Composition and Staff of National Assembly . 28 B. Procedure for Summoning and Dissolution of National Assembly . 29 C. Qualifications for Membership of National Assembly and Right of Attendance . 32 D. Elections to National Assembly . 35 E. Powers and Control over Public Funds . 36 Part II: House of Assembly of a State . 40 A. Composition and Staff of House of Assembly . 40 B. Procedure for Summoning and Dissolution of House of Assembly . 41 C. Qualification for Membership of House of Assembly and Right of Attendance . 43 D. Elections to a House of Assembly . 45 E. Powers and Control over Public Funds . 47 Chapter VI: The Executive . 50 Part I: Federal Executive . 50 A. The President of the Federation . 50 B. Establishment of Certain Federal Executive Bodies . 58 C. Public Revenue . 61 D. The Public Service of the Federation . 63 Part II: State Executive . 65 A. Governor of a State . 65 B. Establishment of Certain State Executive Bodies . -

PSWG Actors Oct 2016
protectionsector COMPLETED AND W O R K I N G G R O U P NIGERIA: PROTECTION ACTORS ON-GOING ACTIVITIES N I G E R I A Agencies with registered projects in OCHA Online Project Systems (OPS) JAN - OCT 2016 COOPI (Cooperazione Internazionale) DRC (Danish Refugee Council) IOM (International Organization for Migration) POPULATION POPULATION POPULATION REACHED 3,168 REACHED 13,363 REACHED 92,911 IMPLEMENTING PARTNERS IMPLEMENTING PARTNERS IMPLEMENTING PARTNERS YOBE BORNO Direct Implementation YOBE BORNO Direct Implementation YOBE BORNO Direct Implementation 3,168 10,988 66,908 JERE DIKWA MAIDUGURI 28 MAIDUGURI DAMATURU DAMATURU POTISKUM KONDUGA BAMA FIKA GWOZA BENEFICIARIES PER ACTIVITY CHIBOK GOMBE GOMBE MICHIKA GOMBE MUBI 2 Case Referrals NORTH GIRERI GIRERI BENEFICIARIES PER ACTIVITY 54 Capacity Building BENEFICIARIES PER ACTIVITY Unaccompanied and ADAMAWA 947 Multiple Needs ADAMAWA ADAMAWA 2 63 Livelihood Separated Children YOLA YOLA SOUTH NORTHYOLA Unaccompanied and YOLA Protection SOUTH 24 Multiple Needs 2,221 NORTH 82 Separated Children Mainstreaming FUFORE 2,375 25,975 175 Case Referrals 176 Awareness Raising / Sensitization 293 Capacity Building 271 Material Protection Assistance Psychosocial Distress Identification of 92,417 and Mental Disorder 3 6 1,727 Vulnerable Individuals 12 LOCAL GOVERNMENT LOCAL GOVERNMENT LOCAL GOVERNMENT UNIT COVERED UNIT COVERED 10,988 Dangers and Injuries UNIT COVERED NRC IRC (International Rescue Committee) NRC (Norwegian Refugee Council) Mercy Corps POPULATION POPULATION POPULATION REACHED 165,191 REACHED -

World Bank Document
PROCUREMENT PLAN (Textual Part) Project information: Country: Nigeria Public Disclosure Authorized Project Name: Multi-Sectoral Crisis Recovery Project for North East Nigeria (MCRP) P- Number: P157891 Project Implementation Agency: MCRP PCU (Federal and States) Date of the Procurement Plan: Updated -December 22, 2017. Period covered by this Procurement Plan: From 01/12/2018 – 30/06/2019. Preamble Public Disclosure Authorized In accordance with paragraph 5.9 of the “World Bank Procurement Regulations for IPF Borrowers” (July 2016) (“Procurement Regulations”) the Bank’s Systematic Tracking and Exchanges in Procurement (STEP) system will be used to prepare, clear and update Procurement Plans and conduct all procurement transactions for the Project. This textual part along with the Procurement Plan tables in STEP constitute the Procurement Plan for the Project. The following conditions apply to all procurement activities in the Procurement Plan. The other elements of the Procurement Plan as required under paragraph 4.4 of the Procurement Regulations are set forth in STEP. The Bank’s Standard Procurement Documents: shall be used for all contracts subject to international competitive procurement and those contracts as specified in the Procurement Plan tables in STEP. Public Disclosure Authorized National Procurement Arrangements: In accordance with paragraph 5.3 of the Procurement Regulations, when approaching the national market (as specified in the Procurement Plan tables in STEP), the country’s own procurement procedures may be used. When the Borrower uses its own national open competitive procurement arrangements as set forth in the FGN Public Procurement Act 2007; such arrangements shall be subject to paragraph 5.4 of the Procurement Regulations. -

Drought Occurrences and Its Implications on the Households in Yobe State, Nigeria Jude Nwafor Eze
Eze Geoenvironmental Disasters (2018) 5:18 Geoenvironmental Disasters https://doi.org/10.1186/s40677-018-0111-7 RESEARCH Open Access Drought occurrences and its implications on the households in Yobe state, Nigeria Jude Nwafor Eze Abstract The study assesses the extent of droughts and its implications on the households in the study area. This is to highlight the need to integrate drought adaptation options into the government development plans. Strategies for drought adaptation options in the study area have often been made without experimental foundations placed on the extent of drought and its implications on the households. To achieve this, the study employed Normalized Rainfall Index (NRI) to determine the extent of droughts and its implications on the households, which has much to offer in terms of policy decisions. The study also utilized questionnaire administrated to 400 households to determine the annual income from different occupations that yielded more income to the people in the study area using one-way analysis of variance (ANOVA). The NRI shows that the study area was characterized by mild to severe drought events. The first (1986–1995) and third (2006–2017) decades experienced high incidences of droughts, while the second decade (1996–2005), witnessed the least incidences of droughts. The result of the economic activities of the households reveals that 65% of the total household respondents were involved in farming, while 35% were involved in non-farming activities as their major source of livelihood. The analysis of variance on the economic activities that generated more income to the households in Yobe State shows that farming activities provided more opportunities for income generation. -

PSWG Actors Nov 2016
protectionsector COMPLETED AND W O R K I N G G R O U P NIGERIA: PROTECTION ACTORS ON-GOING ACTIVITIES N I G E R I A Agencies with registered projects in OCHA Online Project Systems (OPS) JAN - NOV 2016 COOPI (Cooperazione Internazionale) DRC (Danish Refugee Council) IOM (International Organization for Migration) POPULATION POPULATION POPULATION REACHED 3,305 REACHED 14,505 REACHED 112,221 IMPLEMENTING PARTNERS IMPLEMENTING PARTNERS IMPLEMENTING PARTNERS YOBE BORNO Direct Implementation YOBE BORNO Direct Implementation YOBE BORNO Direct Implementation 3,305 11,088 82,312 JERE DIKWA MAIDUGURI 68 MAIDUGURI DAMATURU DAMATURU POTISKUM KONDUGA BAMA FIKA GWOZA BENEFICIARIES PER ACTIVITY CHIBOK GOMBE GOMBE MICHIKA GOMBE MUBI NORTH GIRERI 2 Case Referrals GIRERI BENEFICIARIES PER ACTIVITY BENEFICIARIES PER ACTIVITY 32 Livelihood Unaccompanied and ADAMAWA 947 Multiple Needs ADAMAWA ADAMAWA 2 Protection Separated Children 28 YOLA Mainstreaming YOLA SOUTH NORTHYOLA Unaccompanied and YOLA SOUTH Multiple Needs 2,358 NORTH 24 Separated Children 248 Capacity Building FUFORE 3,417 29,841 175 Case Referrals 381 Awareness Raising / Sensitization 333 Capacity Building Identification of 388 Vulnerable Individuals 111,687 Psychosocial Distress 1,267 Material Protection and Mental Disorder 3 6 Assistance 12 LOCAL GOVERNMENT LOCAL GOVERNMENT LOCAL GOVERNMENT UNIT COVERED UNIT COVERED 10,988 Dangers and Injuries UNIT COVERED NRC IRC (International Rescue Committee) NRC (Norwegian Refugee Council) Mercy Corps POPULATION POPULATION POPULATION REACHED 332,790 REACHED -

States and Lcdas Codes.Cdr
PFA CODES 28 UKANEFUN KPK AK 6 CHIBOK CBK BO 8 ETSAKO-EAST AGD ED 20 ONUIMO KWE IM 32 RIMIN-GADO RMG KN KWARA 9 IJEBU-NORTH JGB OG 30 OYO-EAST YYY OY YOBE 1 Stanbic IBTC Pension Managers Limited 0021 29 URU OFFONG ORUKO UFG AK 7 DAMBOA DAM BO 9 ETSAKO-WEST AUC ED 21 ORLU RLU IM 33 ROGO RGG KN S/N LGA NAME LGA STATE 10 IJEBU-NORTH-EAST JNE OG 31 SAKI-EAST GMD OY S/N LGA NAME LGA STATE 2 Premium Pension Limited 0022 30 URUAN DUU AK 8 DIKWA DKW BO 10 IGUEBEN GUE ED 22 ORSU AWT IM 34 SHANONO SNN KN CODE CODE 11 IJEBU-ODE JBD OG 32 SAKI-WEST SHK OY CODE CODE 3 Leadway Pensure PFA Limited 0023 31 UYO UYY AK 9 GUBIO GUB BO 11 IKPOBA-OKHA DGE ED 23 ORU-EAST MMA IM 35 SUMAILA SML KN 1 ASA AFN KW 12 IKENNE KNN OG 33 SURULERE RSD OY 1 BADE GSH YB 4 Sigma Pensions Limited 0024 10 GUZAMALA GZM BO 12 OREDO BEN ED 24 ORU-WEST NGB IM 36 TAKAI TAK KN 2 BARUTEN KSB KW 13 IMEKO-AFON MEK OG 2 BOSARI DPH YB 5 Pensions Alliance Limited 0025 ANAMBRA 11 GWOZA GZA BO 13 ORHIONMWON ABD ED 25 OWERRI-MUNICIPAL WER IM 37 TARAUNI TRN KN 3 EDU LAF KW 14 IPOKIA PKA OG PLATEAU 3 DAMATURU DTR YB 6 ARM Pension Managers Limited 0026 S/N LGA NAME LGA STATE 12 HAWUL HWL BO 14 OVIA-NORTH-EAST AKA ED 26 26 OWERRI-NORTH RRT IM 38 TOFA TEA KN 4 EKITI ARP KW 15 OBAFEMI OWODE WDE OG S/N LGA NAME LGA STATE 4 FIKA FKA YB 7 Trustfund Pensions Plc 0028 CODE CODE 13 JERE JRE BO 15 OVIA-SOUTH-WEST GBZ ED 27 27 OWERRI-WEST UMG IM 39 TSANYAWA TYW KN 5 IFELODUN SHA KW 16 ODEDAH DED OG CODE CODE 5 FUNE FUN YB 8 First Guarantee Pension Limited 0029 1 AGUATA AGU AN 14 KAGA KGG BO 16 OWAN-EAST -

344157-Eng.Pdf (1.882Mb)
GOMBE STATE C.D.T.I.PROJECT. I ORIGINAL: English COUNTRY/NOTF: NIGERIA Proiect Name: NOTF/APOC- WHO CDTI PROJECT GOMBE STATE. Aporoval vear: December 1999 Launchins vear: March 2000 Reportinq period (Month/Year): l't January 2006 - 31't December 2006 Proiectvearofthisreoort: (circleone)l 2 3 4 5(6)78 9 10 Date submitted: January 2007 NGDO nartner: UNICEF. vlz Fc: Acx -,:r To: { Sitt rsb l b? I AHE t BFo I t Fo I ' For hfcrmgilon ; g ro,5i R. i l I 0 8 JU|N 2007 I ffifu, I )/- d.gaKbna- I #rE# t ANNUAL PROJECT TECHNICAL REPORT SUBMITTED TO TECHNICAL CONSULTATTVE COMMITTEE (TCC) I g.i $u{ v t ry AFRICANPROGRAMME FOR ONCHOCERCIASIS CONTROL (APOC) ANNUAL PROJECT TECHNICAL REPORT TO TECHNICAL CONSULTATIVE COMMITTEE (TCC) ENDORSEMENT Please confirm you have read this report by signing in the appropriate space. OFFICERS to sign the report: Country: _NIGERIA National Coordinator Name: P. O PEARCE (MRS) s-t ) vtL- Signahre: .. W.t.\ z'- L5 -)/--\- L.' Date: ..?.iI I Zonal Oncho Coordinator Name: P. O PEARCE (MRS). Signature: . W*:!{- Date: ...L i. l,; I z vuV This report has been prepared by Name : HARUNA ALI D Designation Signature Date Table of contents ACRoNYMS.......... ..... vt DEFTNITIONS""""' "'vlr FOLLOW UP ON TCC RECOMMENDATIONS.. .........1 EXECUTTVE SUMMARY........... ....................2 SECTION 1: BACKGROUND INFOR]VIATION....... ..........."'."""'3 1.1. GnNpneI- INFORMATION....... .... J 1.1.1 Description of the prolect (briefly) 3 1.1.2. Partnership... 5 1.2. PopuLerroN 6 SECTION 2: IMPLEMENTATION OF CDTI....... ...""'8 2.1. Turmt,rxrB oF ACTIVITIES...... - --.. .....8 2.2 Arvocacv ......11 23 2.4. -

E-Vouchers in Conflict Situations APPROACHES and LESSONS LEARNED from NORTHEAST NIGERIA (AUGUST 2016 - SEPTEMBER 2017)
STUDY BRIEF A CRS community mobilizer uses a fingerprint scanner for beneficiary e-voucher registration. With e-vouchers, people can purchase food and living supplies, such as jerry cans, soap and cooking utensils. Photo by Dooshima Tsee/CRS E-vouchers in Conflict Situations APPROACHES AND LESSONS LEARNED FROM NORTHEAST NIGERIA (AUGUST 2016 - SEPTEMBER 2017) I. OVERVIEW volatile security and physical accessibility, as well This case study presents a detailed description of as in regions where markets are active, through the 1 the utilization of electronic vouchers (or e-vouchers) setup of a closed-loop system. for the delivery of emergency relief. In these pages, we hope to provide a snapshot for humanitarian II. CONTEXT response peers on best practices, lessons learned Now in its eighth year, the Lake Chad Basin crisis and recommendations for the implementation of spans the countries of Cameroon, Chad, Niger and e-voucher programming during an emergency Nigeria. In Nigeria alone, it is estimated that the response, based on projects carried out by Catholic conflict has affected 14 million people, including Relief Services (CRS) and implementing partners (IPs) in support of internally displaced persons (IDPs) and vulnerable host communities in Northeast 1 A closed-loop system is a system in which the institution Nigeria. The following principles and practices that issues the payment card is the same institution that can be adapted to diverse contexts, and may be provides the acquiring infrastructure, and in which the card or password can only be used on the acquiring infrastructure particularly useful in areas with limited connectivity, of that one institution. -
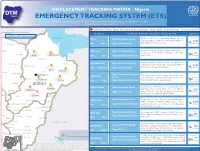
ETS) IOM OIM the DTM Emergency Tracking Tool (ETS) Is Deployed to Track and Provide Up-To-Date Information on Sudden Displacement and Return Movements
DISPLACEMENT TRACKING MATRIX - Nigeria DTM Nigeria EMERGENCY TRACKING SYSTEM (ETS) IOM OIM The DTM Emergency Tracking Tool (ETS) is deployed to track and provide up-to-date information on sudden displacement and return movements CHAD SNAPSHOT: Pulka, Bama, Monguno, Gubio, Konduga, Dikwa, Mafa, Chibok, Gwoza - February 10, 2017 NIGER Checkpoint Characteristic of movement (January 27 - February 10, 2017) Population LOCATIONS WITH IDP MOVEMENT Lake chad Estimate PULKA Type of movement: Arrivals Inow of IDPs from neighboring villages due to ongoing military activity in nearby Ngoshi village in 3,000 Gwoza LGA . Shelters are needed. persons Yunusari LGA: Gwoza Trigger: military activity Estimate Bursari BAMA Town Type of movement: Arrivals A total of 67 People returned to Nigeria from cameroon on January 29 (19 IDPs) & February 2 (48 IDPs) 67 Geidam Gubio Monguno LGA: Bama Trigger: Newly accessible areas respectively. persons Nganzai Estimate MONGUNO Town Type of movement: Arrivals Ongoing military oensive in Marte has opened up Tarmua Ngala villages previously inaccessible causing daily inux of Magumeri 8,000 LGA: Monguno Trigger: military activity IDPs towards Monguno from Marte. persons Mafa Jere Dikwa Fune Damaturu Maiduguri Type of movement: Anticipated Estimate GUBIO Town The military announced last week that people could Potiskum returns start returning to Ngetra, Kingowa, Feto, Zowo and Returns Kaga are Konduga Bama LGA: Gubio Trigger: Newly accessible areas Ardimin Wards. Returns are anticipated. anticipated Gujba Fika BORNO Estimate KONDUGA Town Type of movement: Arrivals Galtimari area of Konduga has received about 1,200 Gwoza individuals from Kawuri Village from the 27th of Damboa 1,827 Nafada Gulani LGA: Konduga Trigger: military activity January till date. -

Northeast Nigeria
Humanitarian Access SCORE Report: Northeast Nigeria Survey on the Coverage, Operational Reach, and Effectiveness of Humanitarian Aid Humanitarian Access SCORE Report: Northeast Nigeria Survey on the Coverage, Operational Reach, and Effectiveness of Humanitarian Aid Abby Stoddard, Paul Harvey, Monica Czwarno, and Meriah-Jo Breckenridge January 2020 www.humanitarianoutcomes.org www.aidworkersecurity.org SCORE reports Under the CORE research programme, supported by the Office of US Foreign Disaster Assistance (OFDA)/United States Agency for International Development (USAID), Humanitarian Outcomes is conducting remote surveys of crisis-affected populations in hard-to-reach areas to gain their perspectives on access to aid and the effectiveness of the humanitarian response. The results of the surveys on coverage, operational reach, and effectiveness (SCORE), together with key informant interviews and other contextual data, help identify the humanitarian actors that have achieved the greatest presence and coverage. Humanitarian Outcomes designed a survey instrument, containing a mix of closed- and open-ended questions to target populations in particular geographic locations through random dialling to mobile phones. Our survey provider partner, GeoPoll, trains enumerators to conduct computer-assisted telephone interviews. Surveys conducted to date include the six states of northeast Nigeria, and four provinces in Afghanistan. Further SCORE reports are planned for Afghanistan and Central African Republic. The survey instrument and downloadable -
Food Issues Demographic, Urban, Migration and Security Challenges
No.2, NOVEMBER 2016 MAPS & FACTS FOOD ISSUES DEMOGRAPHIC, URBAN, MIGRATION AND SECURITY CHALLENGES www.food-security.net SAHEL AND WEST AFRICA Club UEMOA Secretariat ABOUT THE RPCA Promoting dialogue and co-ordination, building a coherent and shared understanding of the food and nutrition situation, and nurturing decision-making: these objectives have been at the heart of the Food Crisis Prevention Network’s (RPCA) mission for over 30 years. Created in 1984, the RPCA is an international network for co-operation and co-ordination under the political leadership of the Commissions of the Economic Community of West African States (ECOWAS) and the West African Economic and Monetary Union (UEMOA). Co-ordinated jointly by the Permanent Inter-State Committee for Drought Control in the Sahel (CILSS) and the Sahel and West Africa Club Secretariat (SWAC/OECD), the RPCA brings together the region’s key food and nutrition security stakeholders: representatives of Sahelian and West African countries, regional organisations, regional and international information systems, bilateral and multilateral co-operation agencies, humanitarian agencies and international NGOs, agricultural professional organisations, civil society and the private sector. This document, as well as any data and map included herein, are without prejudice to the status of or sovereignty over any territory, to the delimitation of international frontiers and boundaries and to the name of any territory, city or area. We encourage the use of our maps. Please include the SWAC’s copyright, and inform or contact us for specific requests: [email protected] Photos: Nutrition training, Ouagadougou, Burkina Faso, 2016 © OECD/SWAC CONTENTS DEMOGRAPHIC TRENDS P. -

Artboard 1Yobe State COVID-19 Risk
Nigeria: Yobe State - COVID-19 Risk Map for LGAs Number of Local Partners Government Area Presence NGOs/UN 17 14 Agencies LGAs with ongoing Partners including activities International NGOs, National NGOs and UN Agencies 11/3 KARASUWA (4 Partners) YUSUFARI (4 Partners) YUNUSARI (4 Partners) CRS, UNFPA, UNICEF, WHO CRS, UNFPA, UNICEF, WHO MSF-Spain, UNFPA, UNICEF, WHO MACHINA (4 Partners) YUSUFARI GEIDAM (4 Partners) CRS, UNFPA, UNICEF, WHO YUNUSARI MACHINA CRS, UNFPA, UNICEF,WHO NGURU KARASUWA BADE BURSARI (5 Partners) NGURU (6 Partners) BURSARI CRS, FHI360, IHVN, UNFPA, CRS, FHI360, GESDI, UNFPA, BADE GEIDAM UNICEF, WHO UNICEF, WHO JAKUSKO TARMUA (5 Partners) BADE (6 Partners) TARMUA GESDI, NEYIF, UNFPA, AAH, FHI360, GESDI, UNFPA, UNICEF, WHO UNICEF, WHO DAMATURU NANGERE DAMATURU (8 Partners) JAKUSKO (4 Partners) POTISKUM FHI360, IHVN, IRC, MC, NRC, COOPI, UNFPA, UNICEF, MSF-Spain, UNFPA, UNICEF, WHO FUNE WHO FIKA GUJBA GUJBA (8 Partners) NANGERE (3 Partners) AAH, ICRC, IRC, NRC/IFRC, UNFPA, UNICEF, WHO GULANI MC, UNFPA, UNICEF, WHO GULANI (8 Partners) POTISKUM (5 Partners) AAH, ICRC, IRC, NRC/IFRC, AAH, FHI360, UNFPA, MC, UNFPA, UNICEF, WHO UNICEF, WHO FIKA (5 Partners) FUNE (5 Partners) FHI360, GESDI, UNFPA, . CRS, NRC/IFRC, UNFPA, UNICEF, WHO UNICEF, WHO ORGANIZATION ACRONYMS IHVN Institute of Human Virology of Nigeria COVID-19: Risk Level AAH Action Against Hunger IRC International Rescue Commitee COOPI COOperazione Internationale MC Malaria Consortium Medium Risk CRS Catholic Relief Services MSF - Spain Medecin Sans Frontieres Spain High Risk FHI 360 Family Health International NEYIF North East Youth Initiative For Development L NRCS Nigerian Red Cross Society Very High Risk GESDI Green Environmental Sustainability & Development Initiative UNFPA United Nations Population Fund ICRC International Committee of the Red Cross UNICEF United Nations Children's Emergency Fund IFRC International Federation of Red Cross & WHO World Health Organization Red Crescent Societies OUR PARTNERS.