Longest Bone Discover the Longest Bone in Your Body and Find out What Dinosaur(S) Were the Same Height As You!
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Patellofemoral Syndrome: Evaluation & Management Scott Sevinsky MSPT
Patellofemoral Syndrome: Evaluation & Management Scott Sevinsky MSPT What is Patellofemoral Syndrome? Patellofemoral syndrome (PFS) is a term commonly used to describe a condition where the patella ‘tracks’ or glides improperly between the femoral condyles. This improper tracking causes pain in the anterior knee and may lead to degenerative changes or dislocation of the knee cap. To be more precise the term ‘anterior knee pain’ is suggested to encompass all pain-related problems of the anterior part of the knee. By excluding anterior knee pain due to intra-articular pathology, peripatellar tendinitis or bursitis, plica syndromes, Sinding Larsen’s disease, Osgood Schlatter’s disease, neuromas and other rarely occurring pathologies it is suggested that remaining patients with a clinical presentation of anterior knee pain could be diagnosed with PFPS. The term ‘patellofemoral’ is used as no distinction can be made as to which specific structure of the patella or femur is affected. The term ‘chondromalacia patellae’, defined at the beginning of the 20th century to describe pathological changes of the retropatellar cartilage,7,8 was for half a century, used as a synonym for the syndrome of patellofemoral pain. However, several studies during the last 2 decades have shown a poor correlation between articular cartilage damage and the still not well-defined pain mechanism of retropatellar pain. Review of Knee Anatomy 1. Femur – thigh bone; longest bone in the body. · Lateral femoral condyle larger than medial condyle & projects farther anteriorly. · Medial femoral condyle longer anterior to posterior · Distal surfaces are convex · Intercondylar (trochlear) notch: groove in which the patella glides or ‘tracks’ 2. -

Study Guide Medical Terminology by Thea Liza Batan About the Author
Study Guide Medical Terminology By Thea Liza Batan About the Author Thea Liza Batan earned a Master of Science in Nursing Administration in 2007 from Xavier University in Cincinnati, Ohio. She has worked as a staff nurse, nurse instructor, and level department head. She currently works as a simulation coordinator and a free- lance writer specializing in nursing and healthcare. All terms mentioned in this text that are known to be trademarks or service marks have been appropriately capitalized. Use of a term in this text shouldn’t be regarded as affecting the validity of any trademark or service mark. Copyright © 2017 by Penn Foster, Inc. All rights reserved. No part of the material protected by this copyright may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the copyright owner. Requests for permission to make copies of any part of the work should be mailed to Copyright Permissions, Penn Foster, 925 Oak Street, Scranton, Pennsylvania 18515. Printed in the United States of America CONTENTS INSTRUCTIONS 1 READING ASSIGNMENTS 3 LESSON 1: THE FUNDAMENTALS OF MEDICAL TERMINOLOGY 5 LESSON 2: DIAGNOSIS, INTERVENTION, AND HUMAN BODY TERMS 28 LESSON 3: MUSCULOSKELETAL, CIRCULATORY, AND RESPIRATORY SYSTEM TERMS 44 LESSON 4: DIGESTIVE, URINARY, AND REPRODUCTIVE SYSTEM TERMS 69 LESSON 5: INTEGUMENTARY, NERVOUS, AND ENDOCRINE S YSTEM TERMS 96 SELF-CHECK ANSWERS 134 © PENN FOSTER, INC. 2017 MEDICAL TERMINOLOGY PAGE III Contents INSTRUCTIONS INTRODUCTION Welcome to your course on medical terminology. You’re taking this course because you’re most likely interested in pursuing a health and science career, which entails proficiencyincommunicatingwithhealthcareprofessionalssuchasphysicians,nurses, or dentists. -

Luxating Patella
LUXATING PATELLA What is a luxating patella? The patella, or kneecap, is normally located in the center of the knee joint. The term luxating means, “out of place” or “dislocated”. Therefore, a luxating patella is a kneecap that moves out of its normal location. What causes this? The muscles of the thigh attach to the top of the kneecap. There is a ligament, the patellar ligament, running from the bottom of the kneecap to a point on the tibia just below the knee joint. When the thigh muscles contract, force is transmitted through the patella and patellar ligament to a point on the top of the tibia. This results in extension or straightening of the knee. The patella stays in the center of the leg because the point of attachment of the patellar ligament is on the midline and because the patella slides in a groove on the lower end of the femur (the bone between the knee and the hip). The patella luxates because the point of attachment of the patellar ligament is not on the midline of the tibia. It is almost always located too far medial (toward the middle of the body). As the thigh muscles contract, the force is pulled medial. After several months or years of this abnormal movement, the inner side of the groove in the femur wears down. Once the side of the groove wears down, the patella is then free to dislocate. When this occurs, the dog has difficulty bearing weight on the leg. It may learn how to kick the leg and snap the patella back into its normal location. -
Intramedullary Nailing for Femur Fracture Management a Guide for Parents
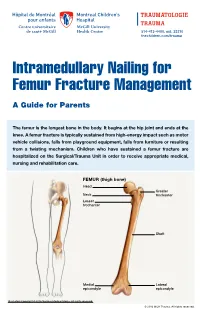
514-412-4400, ext. 23310 thechildren.com/trauma Intramedullary Nailing for Femur Fracture Management A Guide for Parents The femur is the longest bone in the body. It begins at the hip joint and ends at the knee. A femur fracture is typically sustained from high-energy impact such as motor vehicle collisions, falls from playground equipment, falls from furniture or resulting from a twisting mechanism. Children who have sustained a femur fracture are hospitalized on the Surgical/Trauma Unit in order to receive appropriate medical, nursing and rehabilitation care. FEMUR (thigh bone) Head Greater Neck trochanter Lesser trochanter Shaft Medial Lateral epicondyle epicondyle Illustration Copyright © 2016 Nucleus Medical Media, All rights reserved. © 2016 MCH Trauma. All rights reserved. FEMUR FRACTURE MANAGEMENT The pediatric Orthopedic Surgeon will assess your child in order to determine the optimal treatment method. Treatment goals include: achieving proper bone realignment, rapid healing, and the return to normal daily activities. The treatment method chosen is primarily based on the child’s age but also taken into consideration are: fracture type, location and other injuries sustained if applicable. Prior to the surgery, your child may be placed in skin traction. This will ensure the bone is in an optimal healing position until it is surgically repaired. Occasionally, traction may be used for a longer period of time. The surgeon will determine if this management is needed based on the specific fracture type and/or location. ELASTIC/FLEXIBLE INTRAMEDULLARY NAILING This surgery is performed by the Orthopedic Surgeon in the Operating Room under general anesthesia. The surgeon will usually make two small incisions near the knee joint in order to insert two flexible titanium rods (intramedullary nails) Flexible through the femur. -

Unilateral Proximal Focal Femoral Deficiency, Fibular Aplasia, Tibial
The Egyptian Journal of Medical Human Genetics (2014) 15, 299–303 Ain Shams University The Egyptian Journal of Medical Human Genetics www.ejmhg.eg.net www.sciencedirect.com CASE REPORT Unilateral proximal focal femoral deficiency, fibular aplasia, tibial campomelia and oligosyndactyly in an Egyptian child – Probable FFU syndrome Rabah M. Shawky a,*, Heba Salah Abd Elkhalek a, Shaimaa Gad a, Shaimaa Abdelsattar Mohammad b a Pediatric Department, Genetics Unit, Ain Shams University, Egypt b Radio Diagnosis Department, Ain Shams University, Egypt Received 2 March 2014; accepted 18 March 2014 Available online 30 April 2014 KEYWORDS Abstract We report a fifteen month old Egyptian male child, the third in order of birth of healthy Short femur; non consanguineous parents, who has normal mentality, normal upper limbs and left lower limb. Limb anomaly; The right lower limb has short femur, and tibia with anterior bowing, and an overlying skin dimple. FFU syndrome; The right foot has also oligosyndactyly (three toes), and the foot is in vulgus position. There is lim- Proximal focal femoral ited abduction at the hip joint, full flexion and extension at the knee, limited dorsiflexion and plan- deficiency; tar flexion at the ankle joint. The X-ray of the lower limb and pelvis shows proximal focal femoral Fibular aplasia; deficiency, absent right fibula with shortening of the right tibia and anterior bowing of its distal Tibial campomelia; third. The acetabulum is shallow. He has a family history of congenital cyanotic heart disease. Oligosyndactyly Our patient represents most probably the first case of femur fibula ulna syndrome (FFU) in Egypt with unilateral right leg affection. -

Bones Can Tell Us More Compiled By: Nancy Volk
Bones Can Tell Us More Compiled By: Nancy Volk Strong Bones Sometimes only a few bones are found in a location in an archeological dig. VOCABULARY A few bones can tell about the height of a person. This is possible due to the Femur ratios of the bones. It has been determined that there are relationships between the femur, tibia, humerus, and radius and a person’s height. Humerus Radius Here is a little help to identify these four bones and formulas to assist with Tibia determining the height of a person based on bone length. Humerus Femur: Humerus: The thigh is the region of the femur. The arm bone most people call the From the hip bone to the knee bone. upper arm. It is found from the elbow to the shoulder joints. Inside This Packet Radius Strong Bones 1 New York State Standards 1 Activity: Bone Relationships 2 Information for the Teacher 4 Tibia: Radius: The larger and stronger of the two bones The bone found in the forearm that New York State Standards in the leg below the knee bone. extends from the side of the elbow to Middle School In vertebrates It is recognized as the the wrist. Standard 4: Living Environment strongest weight bearing bone in the Idea 1: 1.2a, 1.2b, 1.2e, 1.2f body. Life Sciences - Post Module 3 Middle School Page 1 Activity: Bone Relationships MATERIALS NEEDED Skeleton Formulas: Tape Measure Bone relationship is represented by the following formulas: Directions and formulas P represents the person’s height. The last letter of each formula stands for the Calculator known length of the bone (femur, tibia, humerus, or radius) through measurement. -

Normative Values for Femoral Length, Tibial Length, Andthe Femorotibial
Article Normative Values for Femoral Length, Tibial Length, and the Femorotibial Ratio in Adults Using Standing Full-Length Radiography Stuart A Aitken MaineGeneral Medical Center, 35 Medical Center Parkway, Augusta, ME 04330, USA; [email protected] Abstract: Knowledge of the normal length and skeletal proportions of the lower limb is required as part of the evaluation of limb length discrepancy. When measuring limb length, modern standing full-length digital radiographs confer a level of clinical accuracy interchangeable with that of CT imaging. This study reports a set of normative values for lower limb length using the standing full-length radiographs of 753 patients (61% male). Lower limb length, femoral length, tibial length, and the femorotibial ratio were measured in 1077 limbs. The reliability of the measurement method was tested using the intra-class correlation (ICC) of agreement between three observers. The mean length of 1077 lower limbs was 89.0 cm (range 70.2 to 103.9 cm). Mean femoral length was 50.0 cm (39.3 to 58.4 cm) and tibial length was 39.0 cm (30.8 to 46.5 cm). The median side-to-side difference was 0.4 cm (0.2 to 0.7, max 1.8 cm) between 324 paired limbs. The mean ratio of femoral length to tibial length for the study population was 1.28:1 (range 1.16 to 1.39). A moderately strong inverse linear relationship (r = −0.35, p < 0.001, Pearson’s) was identified between tibial length and the Citation: Aitken, S.A. Normative corresponding femorotibial ratio. -

Congenital Abnormalities of the Femur
Arch Dis Child: first published as 10.1136/adc.36.188.410 on 1 August 1961. Downloaded from CONGENITAL ABNORMALITIES OF THE FEMUR BY P. A. RING From the Royal College of Surgeons (RECEIVED FOR PUBLICATION NOVEMBER 25, 1960) Congenital defects of the femur vary from simple tion of its incidence is difficult to obtain, but it hypoplasia of the bone to complete absence. appears to be the commonest congenital defect Classification of these defects has been suggested causing major abnormalities of limb growth. by Nilsonne (1928) and by Mouchet and Ibos (1928), but neither has met with general acceptance. In more recent years Golding (1939, 1948) has demon- Clinical Features strated the close association of the short femur with There is no evidence that this is a familial disorder, congenital coxa vara, and has emphasized that and careful inquiry of the parents has revealed no these are variations of the same underlying abnor- evidence of other congenital disorders within the mality. The clinical distinction between the various immediate family. The history of the pregnancy types of femoral defect is important as a guide to and delivery has failed to indicate any significant the prognosis of limb development. infection or abnormality at this time. In most From an examination of patients with congenital patients the abnormality is apparent at birth, but abnormalities of the femur the following classifica- where the inequality of leg length is slight, the by copyright. tion is suggested: diagnosis may not be made until the child begins to 1. Simple femoral hypoplasia. walk. To ordinary clinical testing the abnormality 2. -

Case Report: Atypical Metatarsal Fracture in a Patient on Long- Term Bisphosphonate Therapy
November 2019. Volume 6. Number 4 Case Report: ATypical Metatarsal Fracture in a Patient on Long- Term Bisphosphonate Therapy Bijan Valiollahi1 , Mostafa Salehpour1 , Hamidreza Bashari1 , Shoeib Majdi1 , Mehdi Mohammadpour1 * 1. Bone and Joint Reconstruction Research Center, Shafa Orthopedic Hospital, Iran University of Medical Sciences, Tehran, Iran. Use your device to scan and read the article online Citation Valiollahi B, Salehpour M, Bashari H, Majdi Sh, Mohammadpour M. ATypical Metatarsal Fracture in a Patient on Long-Term Bisphosphonate Therapy. Journal of Research in Orthopedic Science. 2019; 6(4):25-30. http://dx.doi.org/10.32598/ JROSJ.6.4.67 : http://dx.doi.org/10.32598/JROSJ.6.4.67 A B S T R A C T Bisphosphonates, more particularly alendronate, are a popular category of drugs in the treatment Article info: of postmenopausal and corticosteroid-induced osteoporosis. The present study contends that the Received: 13 May 2019 long-term consumption of bisphosphonates causes not only subtrochanteric and femoral shaft Revised: 27 May 2019 fractures but also pathological fractures at other musculoskeletal sites. This report presents a Accepted: 16 Sep 2019 rare case of alendronate-induced pathological metatarsal fracture in a 59-year-old female with a Available Online: 01 Nov 2019 history of cuboid fracture following a twisting with abnormal Bone Mineral Density (BMD) (T score: −3.5; lumbar spine and −2.6; proximal femur). Keywords: Alendronate, Pathologic Fracture, Metatarsal 1. Introduction ally, drugs such as bisphosphonates contribute to devel- oping bone fractures. tress fractures occur as a result of repetitive loading and unloading of a bone [1]. In- Bisphosphonates are preferred drugs in postmenopaus- creased strain or frequency of compression al and corticosteroid-induced osteoporosis [6]. -

Stress Fractures in the Foot and Ankle of Athletes Fratura Por Estresse No Pé E Tornozelo De Atletas Authors: Asano LYJ, Duarte Jr
GUIDELINES IN FOCUS ASANO LYJ ET al. Stress fractures in the foot and ankle of athletes FRATURA POR ESTRESSE NO PÉ E TORNOZELO DE ATLETAS Authors: Asano LYJ, Duarte Jr. A, Silva APS http://dx.doi.org/10.1590/1806-9282.60.06.006 The Guidelines Project, an initiative of the Brazilian Medical Association, aims to combine information from the medical field in order to standar- dize procedures to assist the reasoning and decision-making of doctors. The information provided through this project must be assessed and criticized by the physician responsible for the conduct that will be adopted, de- pending on the conditions and the clinical status of each patient. DESCRIPTION OF THE EVIDENCE COLLECTION INTRODUCTION METHOD Stress fractures were described for the first time in 1855 To develop this guideline, the Medline electronic databa- by Breihaupt among soldiers reporting plantar pain and se (1966 to 2012) was consulted via PubMed, as a primary edema following long marches.1 For athletes, the first cli- base. The search for evidence came from actual clinical nical description was given by Devas in 1958, based so- scenarios and used keywords (MeSH terms) grouped in lely on the results of simple X-rays.2 Stress injuries are the following syntax: “Stress fractures”, “Foot”, “Ankle”, common among athletes and military recruits, accoun- “Athletes”, “Professional”, “Military recruit”, “Immobili- ting for approximately 10% of all orthopedic injuries.3 zation”, “Physiotherapy”, “Rest”, “Rehabilitation”, “Con- It is defined as a solution for partial or complete con- ventional treatment”, “Surgery treatment”. The articles tinuity of a bone as a result of excessive or repeated loads, were selected by orthopedic specialists after critical eva- at submaximal intensity, resulting in greater reabsorp- luation of the strength of scientific evidence, and publi- tion faced with an insufficient formation of bone tissue.1 cations of greatest strength were used for recommenda- Although stress fractures may affect all types of bone tion. -

A Missed Ipsilateral Femoral Neck Fracture in A
Special Case Report Series JOT CASE REPORTS www.jorthotrauma.com JOURNALOF ORTHOPAEDIC TRAUMA OFFICIAL JOURNAL OF Orthopaedic Trauma Association Belgian Orthopaedic Trauma Association Canadian Orthopaedic Trauma Society Foundation for Orthopedic Trauma International Society for Fracture Repair The Japanese Society for Fracture Repair Missed Ipsilateral Femoral Neck Fracture in a Young Patient With a Femoral Shaft Fracture Anthony V. Florschutz, MD, PhD,* Derek J. Donegan, MD,† George Haidukewych, MD,* Mark Munro, MD,‡ and Frank A. Liporace, MD§ Summary: Ipsilateral femoral neck-shaft fractures are uncommon INTRODUCTION but significant injuries that can present a diagnostic difficulty with Femoral neck fractures are associated with up to 9% of ipsilateral respect to recognition of femoral neck component. Although there femoral shaft fractures. Between 20% and 50% of these fractures are are improved diagnostic methodologies, identification of a faction reported to be missed on initial presentation, and although there are of these fractures will be delayed or missed even when the most improved diagnostic methodologies, identification of a faction of sensitive protocols are used. As such, it is essential for treating these fractures will be delayed or missed even when the most surgeons to be attentive to the potential associated femoral neck sensitive protocols are used.1 Although this associated pattern of fracture when managing femoral shaft fractures and consider its fractures is not regularly encountered, it is common enough that possibility -

Patellofemoral Syndrome (PFS)
Scott Gudeman, MD 1260 Innovation Pkwy., Suite 100 Greenwood, IN 46143 317.884.5161 OrthoIndy.com ScottGudemanMD.com Patellofemoral Syndrome (PFS) Knee Anatomy The patella is a moveable bone in front of the knee wrapped inside a large tendon that connects the quadriceps (thigh) muscles to the tibia (lower leg bone). A healthy patella moves smoothly in a groove on the lower end of the femur. If the patella is moving incorrectly through this groove, Patellofemoral Syndrome (PFS) could form. Many muscle groups and ligaments control the triangular-shaped patella. The patella is coated on its bottom with a smooth covering called articular cartilage. The patella and the femur form a joint, called the patellofemoral joint, that is made up of muscles, soft tissue attachments and the groove where the patella rests. What is Patellofemoral Syndrome (PFS)? PFS is the medical name for a condition that causes pain in and around the kneecap. The patella (kneecap) is designed to move smoothly over a groove on the femur (thigh bone). When the patella is not moving or “tracking” properly over the femur, PFS can develop. This knee problem commonly appears in runners and athletes but non-athletes can also be affected. For the pediatric population, PFS can be jump-started during times of growth. PFS can strike at any age to any population. Causes of Patellofemoral Syndrome • Muscle imbalances in the quadriceps can cause the patella to move improperly through the groove in the femur. If one or more of the quadriceps muscles are weak, a muscle imbalance could occur. This imbalance pulls the patella off its track through the groove.