Stress Fractures in the Foot and Ankle of Athletes Fratura Por Estresse No Pé E Tornozelo De Atletas Authors: Asano LYJ, Duarte Jr
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Skeletal Foot Structure
Foot Skeletal Structure The disarticulated bones of the left foot, from above (The talus and calcaneus remain articulated) 1 Calcaneus 2 Talus 3 Navicular 4 Medial cuneiform 5 Intermediate cuneiform 6 Lateral cuneiform 7 Cuboid 8 First metatarsal 9 Second metatarsal 10 Third metatarsal 11 Fourth metatarsal 12 Fifth metatarsal 13 Proximal phalanx of great toe 14 Distal phalanx of great toe 15 Proximal phalanx of second toe 16 Middle phalanx of second toe 17 Distal phalanx of second toe Bones of the tarsus, the back part of the foot Talus Calcaneus Navicular bone Cuboid bone Medial, intermediate and lateral cuneiform bones Bones of the metatarsus, the forepart of the foot First to fifth metatarsal bones (numbered from the medial side) Bones of the toes or digits Phalanges -- a proximal and a distal phalanx for the great toe; proximal, middle and distal phalanges for the second to fifth toes Sesamoid bones Two always present in the tendons of flexor hallucis brevis Origin and meaning of some terms associated with the foot Tibia: Latin for a flute or pipe; the shin bone has a fanciful resemblance to this wind instrument. Fibula: Latin for a pin or skewer; the long thin bone of the leg. Adjective fibular or peroneal, which is from the Greek for pin. Tarsus: Greek for a wicker frame; the basic framework for the back of the foot. Metatarsus: Greek for beyond the tarsus; the forepart of the foot. Talus (astragalus): Latin (Greek) for one of a set of dice; viewed from above the main part of the talus has a rather square appearance. -

Patellofemoral Syndrome: Evaluation & Management Scott Sevinsky MSPT
Patellofemoral Syndrome: Evaluation & Management Scott Sevinsky MSPT What is Patellofemoral Syndrome? Patellofemoral syndrome (PFS) is a term commonly used to describe a condition where the patella ‘tracks’ or glides improperly between the femoral condyles. This improper tracking causes pain in the anterior knee and may lead to degenerative changes or dislocation of the knee cap. To be more precise the term ‘anterior knee pain’ is suggested to encompass all pain-related problems of the anterior part of the knee. By excluding anterior knee pain due to intra-articular pathology, peripatellar tendinitis or bursitis, plica syndromes, Sinding Larsen’s disease, Osgood Schlatter’s disease, neuromas and other rarely occurring pathologies it is suggested that remaining patients with a clinical presentation of anterior knee pain could be diagnosed with PFPS. The term ‘patellofemoral’ is used as no distinction can be made as to which specific structure of the patella or femur is affected. The term ‘chondromalacia patellae’, defined at the beginning of the 20th century to describe pathological changes of the retropatellar cartilage,7,8 was for half a century, used as a synonym for the syndrome of patellofemoral pain. However, several studies during the last 2 decades have shown a poor correlation between articular cartilage damage and the still not well-defined pain mechanism of retropatellar pain. Review of Knee Anatomy 1. Femur – thigh bone; longest bone in the body. · Lateral femoral condyle larger than medial condyle & projects farther anteriorly. · Medial femoral condyle longer anterior to posterior · Distal surfaces are convex · Intercondylar (trochlear) notch: groove in which the patella glides or ‘tracks’ 2. -
The Patellofemoral Joint Alignment in Patients with Symptomatic Accessory Navicular Bone
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Firenze University Press: E-Journals IJAE Vol. 121, n. 2: 148-158, 2016 ITALIAN JOURNAL OF ANATOMY AND EMBRYOLOGY Research article - Basic and applied anatomy The patellofemoral joint alignment in patients with symptomatic accessory navicular bone Heba M. Kalbouneh1,*, Abdullah O. Alkhawaldah2, Omar A. Alajoulin2, Mohammad I. Alsalem1 1 Department of Anatomy, Faculty of Medicine, University of Jordan, Amman, Jordan 2 Foot and Ankle Orthopedic Clinic, King Hussein Medical Center, Amman, Jordan Abstract Quadriceps angle (Q angle) provides useful information about the alignment of the patellofem- oral joint. The aim of the present study was to assess a possible link between malalignment of the patellofemoral joint and symptomatic accessory navicular (AN) bone as an underlying cause in early adolescence using Q angle measurements. This study was performed on patients presenting to the Foot and Ankle Clinic at the Jorda- nian Royal Medical Services because of pain on the medial side of the foot that worsened with activities or shoe wearing, with no history of knee pain, between September 2013 and April 2015. The Q angle was measured using a goniometer in 27 early adolescents aged 10-18 years diagnosed clinically and radiologically with symptomatic AN bone, only seven patients had associated pes planus deformity; the data were compared with age appropriate normal arched feet without AN. Navicular drop test (NDT) was used to assess the amount of foot pronation. The mean Q angle value among male and female patients with symptomatic AN with/with- out pes planus was significantly higher than in controls with normal arched feet without AN (p<0.05). -

Medial Lateral Malleolus
Acutrak 2® Headless Compression Screw System 4.7 mm and 5.5 mm Screws Supplemental Use Guide—Medial & Lateral Malleolus Acumed® is a global leader of innovative orthopaedic and medical solutions. We are dedicated to developing products, service methods, and approaches that improve patient care. Acumed® Acutrak 2® Headless Compression Screw System—4.7 mm and 5.5 mm This guide is intended for supplemental use only and is not intended to be used as a stand-alone surgical technique. Reference the Acumed Acutrak 2 Headless Compression Screw System Surgical Technique (SPF00-02) for more information. Definition Indicates critical information about a potential serious outcome to the Warning patient or the user. Indicates instructions that must be followed in order to ensure the proper Caution use of the device. Note Indicates information requiring special attention. Acumed® Acutrak 2® Headless Compression System—Supplemental Use Guide—Medial & Lateral Malleolus Table of Contents System Features ...........................................2 Surgical Techniques ........................................ 4 Fibula Fracture (Weber A and B Fractures) Surgical Technique: Acutrak 2®—5.5 .......................4 Medial Malleolus Surgical Technique: Acutrak 2®—4.7 ......................10 Ordering Information ......................................16 Acumed® Acutrak 2® Headless Compression System—Supplemental Use Guide—Medial & Lateral Malleolus System Features Headless screw design is intended to minimize soft tissue irritation D Acutrak 2 Screws Diameter -

Assessment, Management and Decision Making in the Treatment Of
Pediatric Ankle Fractures Anthony I. Riccio, MD Texas Scottish Rite Hospital for Children Update 07/2016 Pediatric Ankle Fractures The Ankle is the 2nd most Common Site of Physeal Injury in Children 10-25% of all Physeal Injuries Occur About the Ankle Pediatric Ankle Fractures Primary Concerns Are: • Anatomic Restoration of Articular Surface • Restoration of Symmetric Ankle Mortise • Preservation of Physeal Growth • Minimize Iatrogenic Physeal Injury • Avoid Fixation Across Physis in Younger Children Salter Harris Classification Prognosis and Treatment of Pediatric Ankle Fractures is Often Dictated by the Salter Harris Classification of Physeal Fractures Type I and II Fractures: Often Amenable to Closed Tx / Lower Risk of Physeal Arrest Type III and IV: More Likely to Require Operative Tx / Higher Risk of Physeal Arrest Herring JA, ed. Tachdjian’s Pediatric Orthopaedics, 5th Ed. 2014. Elsevier. Philadelphia, PA. ISOLATED DISTAL FIBULA FRACTURES Distal Fibula Fractures • The Physis is Weaker than the Lateral Ankle Ligaments – Children Often Fracture the Distal Fibula but…. – …ligamentous Injuries are Not Uncommon • Mechanism of Injury = Inversion of a Supinated Foot • SH I and II Fractures are Most Common – SH I Fractures: Average Age = 10 Years – SH II Fractures: Average Age = 12 Years Distal Fibula Fractures Lateral Ankle Tenderness SH I Distal Fibula Fracture vs. Lateral Ligamentous Injury (Sprain) Distal Fibula Fractures • Sankar et al (JPO 2008) – 37 Children – All with Open Physes, Lateral Ankle Tenderness + Normal Films – 18%: Periosteal -

Multiplanar CT Analysis of Fifth Metatarsal Morphology
FAIXXX10.1177/1071100715623041Foot & Ankle InternationalDeSandis et al 623041research-article2015 Article Foot & Ankle International® 2016, Vol. 37(5) 528 –536 Multiplanar CT Analysis of Fifth Metatarsal © The Author(s) 2015 Reprints and permissions: sagepub.com/journalsPermissions.nav Morphology: Implications for Operative DOI: 10.1177/1071100715623041 Management of Zone II Fractures fai.sagepub.com Bridget DeSandis, BA1, Conor Murphy, MD2, Andrew Rosenbaum, MD1, Matthew Levitsky, BA1, Quinn O’Malley1, Gabrielle Konin, MD1, and Mark Drakos, MD1 Abstract Background: Percutaneous internal fixation is currently the method of choice treating proximal zone II fifth metatarsal fractures. Complications have been reported due to poor screw placement and inadequate screw sizing. The purpose of this study was to define the morphology of the fifth metatarsal to help guide surgeons in selecting the appropriate screw size preoperatively. Methods: Multiplanar analysis of fifth metatarsal morphology was completed using computed tomographic (CT) scans from 241 patients. Specific parameters were analyzed and defined in anteroposterior (AP), lateral, and oblique views including metatarsal length, distance from the base to apex of curvature, apex medullary canal width, apex height, and fifth metatarsal angle. Results: The average metatarsal length in the AP view was 71.4 ± 6.1 mm and in the lateral view 70.4 ± 6.0 mm, with 95% of patients having lengths between 59.3 and 83.5 mm and 58.4 and 82.4 mm, respectively. The average canal width at the apex of curvature was 4.1 ± 0.9 mm in the AP view and 5.3 ± 1.1 mm in the lateral view, with 95% of patients having widths between 2.2 and 5.9 mm and 3.2 and 7.5 mm, respectively. -

Rethinking the Evolution of the Human Foot: Insights from Experimental Research Nicholas B
© 2018. Published by The Company of Biologists Ltd | Journal of Experimental Biology (2018) 221, jeb174425. doi:10.1242/jeb.174425 REVIEW Rethinking the evolution of the human foot: insights from experimental research Nicholas B. Holowka* and Daniel E. Lieberman* ABSTRACT presumably owing to their lack of arches and mobile midfoot joints Adaptive explanations for modern human foot anatomy have long for enhanced prehensility in arboreal locomotion (see Glossary; fascinated evolutionary biologists because of the dramatic differences Fig. 1B) (DeSilva, 2010; Elftman and Manter, 1935a). Other studies between our feet and those of our closest living relatives, the great have documented how great apes use their long toes, opposable apes. Morphological features, including hallucal opposability, toe halluces and mobile ankles for grasping arboreal supports (DeSilva, length and the longitudinal arch, have traditionally been used to 2009; Holowka et al., 2017a; Morton, 1924). These observations dichotomize human and great ape feet as being adapted for bipedal underlie what has become a consensus model of human foot walking and arboreal locomotion, respectively. However, recent evolution: that selection for bipedal walking came at the expense of biomechanical models of human foot function and experimental arboreal locomotor capabilities, resulting in a dichotomy between investigations of great ape locomotion have undermined this simple human and great ape foot anatomy and function. According to this dichotomy. Here, we review this research, focusing on the way of thinking, anatomical features of the foot characteristic of biomechanics of foot strike, push-off and elastic energy storage in great apes are assumed to represent adaptations for arboreal the foot, and show that humans and great apes share some behavior, and those unique to humans are assumed to be related underappreciated, surprising similarities in foot function, such as to bipedal walking. -

Study Guide Medical Terminology by Thea Liza Batan About the Author
Study Guide Medical Terminology By Thea Liza Batan About the Author Thea Liza Batan earned a Master of Science in Nursing Administration in 2007 from Xavier University in Cincinnati, Ohio. She has worked as a staff nurse, nurse instructor, and level department head. She currently works as a simulation coordinator and a free- lance writer specializing in nursing and healthcare. All terms mentioned in this text that are known to be trademarks or service marks have been appropriately capitalized. Use of a term in this text shouldn’t be regarded as affecting the validity of any trademark or service mark. Copyright © 2017 by Penn Foster, Inc. All rights reserved. No part of the material protected by this copyright may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the copyright owner. Requests for permission to make copies of any part of the work should be mailed to Copyright Permissions, Penn Foster, 925 Oak Street, Scranton, Pennsylvania 18515. Printed in the United States of America CONTENTS INSTRUCTIONS 1 READING ASSIGNMENTS 3 LESSON 1: THE FUNDAMENTALS OF MEDICAL TERMINOLOGY 5 LESSON 2: DIAGNOSIS, INTERVENTION, AND HUMAN BODY TERMS 28 LESSON 3: MUSCULOSKELETAL, CIRCULATORY, AND RESPIRATORY SYSTEM TERMS 44 LESSON 4: DIGESTIVE, URINARY, AND REPRODUCTIVE SYSTEM TERMS 69 LESSON 5: INTEGUMENTARY, NERVOUS, AND ENDOCRINE S YSTEM TERMS 96 SELF-CHECK ANSWERS 134 © PENN FOSTER, INC. 2017 MEDICAL TERMINOLOGY PAGE III Contents INSTRUCTIONS INTRODUCTION Welcome to your course on medical terminology. You’re taking this course because you’re most likely interested in pursuing a health and science career, which entails proficiencyincommunicatingwithhealthcareprofessionalssuchasphysicians,nurses, or dentists. -

Free Vascularized Fibula Graft with Femoral Allograft Sleeve for Lumbar Spine Defects After Spondylectomy of Malignant Tumors Acasereport
1 COPYRIGHT Ó 2020 BY THE JOURNAL OF BONE AND JOINT SURGERY,INCORPORATED Free Vascularized Fibula Graft with Femoral Allograft Sleeve for Lumbar Spine Defects After Spondylectomy of Malignant Tumors ACaseReport Michiel E.R. Bongers, MD, John H. Shin, MD, Sunita D. Srivastava, MD, Christopher R. Morse, MD, Sang-Gil Lee, MD, and Joseph H. Schwab, MD, MS Investigation performed at Massachusetts General Hospital, Boston, Massachusetts Abstract Case: We present a 65-year-old man with an L4 conventional chordoma. Total en bloc spondylectomy (TES) of the involved vertebral bodies and surrounding soft tissues with reconstruction of the spine using a free vascularized fibula autograft (FVFG) is a proven technique, limiting complications and recurrence. However, graft fracture has occurred only in the lumbar spine in our institutional cases. We used a technique in our patient to ensure extra stability and support, with the addition of a femoral allograft sleeve encasing the FVFG. Conclusions: Our technique for the reconstruction of the lumbar spine after TES of primary malignant spinal disease using a femoral allograft sleeve encasing the FVFG is viable to consider. he treatment of primary malignant neoplasms of the spine mended a magnetic resonance imaging (MRI), but the request currently mainly relies on surgery, often in conjunction with was denied by the insurance company, and the patient T 1-3 radiotherapy .Totalen bloc spondylectomy (TES) is a widely underwent a course of physical therapy with no benefitand accepted surgical technique and has lower reported recurrence rates progression of back pain and radiculopathy. Four months compared with patients who undergo intralesional surgery3,4. -

Common Stress Fractures BRENT W
COVER ARTICLE PRACTICAL THERAPEUTICS Common Stress Fractures BRENT W. SANDERLIN, LCDR, MC, USNR, Naval Branch Medical Clinic, Fort Worth, Texas ROBERT F. RASPA, CAPT, MC, USN, Naval Hospital Jacksonville, Jacksonville, Florida Lower extremity stress fractures are common injuries most often associated with partic- ipation in sports involving running, jumping, or repetitive stress. The initial diagnosis can be made by identifying localized bone pain that increases with weight bearing or repet- itive use. Plain film radiographs are frequently unrevealing. Confirmation of a stress frac- ture is best made using triple phase nuclear medicine bone scan or magnetic resonance imaging. Prevention of stress fractures is most effectively accomplished by increasing the level of exercise slowly, adequately warming up and stretching before exercise, and using cushioned insoles and appropriate footwear. Treatment involves rest of the injured bone, followed by a gradual return to the sport once free of pain. Recent evidence sup- ports the use of air splinting to reduce pain and decrease the time until return to full par- ticipation or intensity of exercise. (Am Fam Physician 2003;68:1527-32. Copyright© 2003 American Academy of Family Physicians) tress fractures are among the involving repetitive use of the arms, such most common sports injuries as baseball or tennis. Stress fractures of and are frequently managed the ribs occur in sports such as rowing. by family physicians. A stress Upper extremity and rib stress fractures fracture should be suspected in are far less common than lower extremity Sany patient presenting with localized stress fractures.1 bone or periosteal pain, especially if he or she recently started an exercise program Etiology and Pathophysiology or increased the intensity of exercise. -

Luxating Patella
LUXATING PATELLA What is a luxating patella? The patella, or kneecap, is normally located in the center of the knee joint. The term luxating means, “out of place” or “dislocated”. Therefore, a luxating patella is a kneecap that moves out of its normal location. What causes this? The muscles of the thigh attach to the top of the kneecap. There is a ligament, the patellar ligament, running from the bottom of the kneecap to a point on the tibia just below the knee joint. When the thigh muscles contract, force is transmitted through the patella and patellar ligament to a point on the top of the tibia. This results in extension or straightening of the knee. The patella stays in the center of the leg because the point of attachment of the patellar ligament is on the midline and because the patella slides in a groove on the lower end of the femur (the bone between the knee and the hip). The patella luxates because the point of attachment of the patellar ligament is not on the midline of the tibia. It is almost always located too far medial (toward the middle of the body). As the thigh muscles contract, the force is pulled medial. After several months or years of this abnormal movement, the inner side of the groove in the femur wears down. Once the side of the groove wears down, the patella is then free to dislocate. When this occurs, the dog has difficulty bearing weight on the leg. It may learn how to kick the leg and snap the patella back into its normal location. -
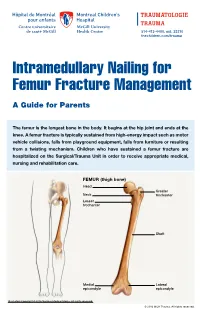
Intramedullary Nailing for Femur Fracture Management a Guide for Parents
514-412-4400, ext. 23310 thechildren.com/trauma Intramedullary Nailing for Femur Fracture Management A Guide for Parents The femur is the longest bone in the body. It begins at the hip joint and ends at the knee. A femur fracture is typically sustained from high-energy impact such as motor vehicle collisions, falls from playground equipment, falls from furniture or resulting from a twisting mechanism. Children who have sustained a femur fracture are hospitalized on the Surgical/Trauma Unit in order to receive appropriate medical, nursing and rehabilitation care. FEMUR (thigh bone) Head Greater Neck trochanter Lesser trochanter Shaft Medial Lateral epicondyle epicondyle Illustration Copyright © 2016 Nucleus Medical Media, All rights reserved. © 2016 MCH Trauma. All rights reserved. FEMUR FRACTURE MANAGEMENT The pediatric Orthopedic Surgeon will assess your child in order to determine the optimal treatment method. Treatment goals include: achieving proper bone realignment, rapid healing, and the return to normal daily activities. The treatment method chosen is primarily based on the child’s age but also taken into consideration are: fracture type, location and other injuries sustained if applicable. Prior to the surgery, your child may be placed in skin traction. This will ensure the bone is in an optimal healing position until it is surgically repaired. Occasionally, traction may be used for a longer period of time. The surgeon will determine if this management is needed based on the specific fracture type and/or location. ELASTIC/FLEXIBLE INTRAMEDULLARY NAILING This surgery is performed by the Orthopedic Surgeon in the Operating Room under general anesthesia. The surgeon will usually make two small incisions near the knee joint in order to insert two flexible titanium rods (intramedullary nails) Flexible through the femur.