Prevent Dengue & Chikungunya
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Arizona Arboviral Handbook for Chikungunya, Dengue, and Zika Viruses
ARIZONA ARBOVIRAL HANDBOOK FOR CHIKUNGUNYA, DENGUE, AND ZIKA VIRUSES 7/31/2017 Arizona Department of Health Services | P a g e 1 Arizona Arboviral Handbook for Chikungunya, Dengue, and Zika Viruses Arizona Arboviral Handbook for Chikungunya, Dengue, and Zika Viruses OBJECTIVES .............................................................................................................. 4 I: CHIKUNGUNYA ..................................................................................................... 5 Chikungunya Ecology and Transmission ....................................... 6 Chikungunya Clinical Disease and Case Management ............... 7 Chikungunya Laboratory Testing .................................................. 8 Chikungunya Case Definitions ...................................................... 9 Chikungunya Case Classification Algorithm ............................... 11 II: DENGUE .............................................................................................................. 12 Dengue Ecology and Transmission .............................................. 14 Dengue Clinical Disease and Case Management ...................... 14 Dengue Laboratory Testing ......................................................... 17 Dengue Case Definitions ............................................................ 19 Dengue Case Classification Algorithm ....................................... 23 III: ZIKA .................................................................................................................. -

Chikungunya Fever: Epidemiology, Clinical Syndrome, Pathogenesis
Antiviral Research 99 (2013) 345–370 Contents lists available at SciVerse ScienceDirect Antiviral Research journal homepage: www.elsevier.com/locate/antiviral Review Chikungunya fever: Epidemiology, clinical syndrome, pathogenesis and therapy ⇑ Simon-Djamel Thiberville a,b, , Nanikaly Moyen a,b, Laurence Dupuis-Maguiraga c,d, Antoine Nougairede a,b, Ernest A. Gould a,b, Pierre Roques c,d, Xavier de Lamballerie a,b a UMR_D 190 ‘‘Emergence des Pathologies Virales’’ (Aix-Marseille Univ. IRD French Institute of Research for Development EHESP French School of Public Health), Marseille, France b University Hospital Institute for Infectious Disease and Tropical Medicine, Marseille, France c CEA, Division of Immuno-Virologie, Institute of Emerging Diseases and Innovative Therapies, Fontenay-aux-Roses, France d UMR E1, University Paris Sud 11, Orsay, France article info abstract Article history: Chikungunya virus (CHIKV) is the aetiological agent of the mosquito-borne disease chikungunya fever, a Received 7 April 2013 debilitating arthritic disease that, during the past 7 years, has caused immeasurable morbidity and some Revised 21 May 2013 mortality in humans, including newborn babies, following its emergence and dispersal out of Africa to the Accepted 18 June 2013 Indian Ocean islands and Asia. Since the first reports of its existence in Africa in the 1950s, more than Available online 28 June 2013 1500 scientific publications on the different aspects of the disease and its causative agent have been pro- duced. Analysis of these publications shows that, following a number of studies in the 1960s and 1970s, Keywords: and in the absence of autochthonous cases in developed countries, the interest of the scientific commu- Chikungunya virus nity remained low. -

Dengue Fever and Dengue Hemorrhagic Fever (Dhf)
DENGUE FEVER AND DENGUE HEMORRHAGIC FEVER (DHF) What are DENGUE and DHF? Dengue and DHF are viral diseases transmitted by mosquitoes in tropical and subtropical regions of the world. Cases of dengue and DHF are confirmed every year in travelers returning to the United States after visits to regions such as the South Pacific, Asia, the Caribbean, the Americas and Africa. How is dengue fever spread? Dengue virus is transmitted to people by the bite of an infected mosquito. Dengue cannot be spread directly from person to person. What are the symptoms of dengue fever? The most common symptoms of dengue are high fever for 2–7 days, severe headache, backache, joint pains, nausea and vomiting, eye pain and rash. The rash is frequently not visible in dark-skinned people. Young children typically have a milder illness than older children and adults. Most patients report a non-specific flu-like illness. Many patients infected with dengue will not show any symptoms. DHF is a more severe form of dengue. Initial symptoms are the same as dengue but are followed by bleeding problems such as easy bruising, skin hemorrhages, bleeding from the nose or gums, and possible bleeding of the internal organs. DHF is very rare. How soon after exposure do symptoms appear? Symptoms of dengue can occur from 3-14 days, commonly 4-7 days, after the bite of an infected mosquito. What is the treatment for dengue fever? There is no specific treatment for dengue. Treatment usually involves treating symptoms such as managing fever, general aches and pains. Persons who have traveled to a tropical or sub-tropical region should consult their physician if they develop symptoms. -

Dengue and Yellow Fever
GBL42 11/27/03 4:02 PM Page 262 CHAPTER 42 Dengue and Yellow Fever Dengue, 262 Yellow fever, 265 Further reading, 266 While the most important viral haemorrhagic tor (Aedes aegypti) as well as reinfestation of this fevers numerically (dengue and yellow fever) are insect into Central and South America (it was transmitted exclusively by arthropods, other largely eradicated in the 1960s). Other factors arboviral haemorrhagic fevers (Crimean– include intercontinental transport of car tyres Congo and Rift Valley fevers) can also be trans- containing Aedes albopictus eggs, overcrowding mitted directly by body fluids. A third group of of refugee and urban populations and increasing haemorrhagic fever viruses (Lassa, Ebola, Mar- human travel. In hyperendemic areas of Asia, burg) are only transmitted directly, and are not disease is seen mainly in children. transmitted by arthropods at all. The directly Aedes mosquitoes are ‘peri-domestic’: they transmissible viral haemorrhagic fevers are dis- breed in collections of fresh water around the cussed in Chapter 41. house (e.g. water storage jars).They feed on hu- mans (anthrophilic), mainly by day, and feed re- peatedly on different hosts (enhancing their role Dengue as vectors). Dengue virus is numerically the most important Clinical features arbovirus infecting humans, with an estimated Dengue virus may cause a non-specific febrile 100 million cases per year and 2.5 billion people illness or asymptomatic infection, especially in at risk.There are four serotypes of dengue virus, young children. However, there are two main transmitted by Aedes mosquitoes, and it is un- clinical dengue syndromes: dengue fever (DF) usual among arboviruses in that humans are the and dengue haemorrhagic fever (DHF). -

Antibody-Mediated Enhancement Aggravates Chikungunya Virus
www.nature.com/scientificreports OPEN Antibody-mediated enhancement aggravates chikungunya virus infection and disease severity Received: 14 July 2017 Fok-Moon Lum 1,2, Thérèse Couderc3,4, Bing-Shao Chia1,8, Ruo-Yan Ong1,9, Zhisheng Her1,10, Accepted: 17 January 2018 Angela Chow5, Yee-Sin Leo5, Yiu-Wing Kam1, Laurent Rénia1, Marc Lecuit 3,4,6 & Published: xx xx xxxx Lisa F. P. Ng1,2,7 The arthropod-transmitted chikungunya virus (CHIKV) causes a fu-like disease that is characterized by incapacitating arthralgia. The re-emergence of CHIKV and the continual risk of new epidemics have reignited research in CHIKV pathogenesis. Virus-specifc antibodies have been shown to control virus clearance, but antibodies present at sub-neutralizing concentrations can also augment virus infection that exacerbates disease severity. To explore this occurrence, CHIKV infection was investigated in the presence of CHIKV-specifc antibodies in both primary human cells and a murine macrophage cell line, RAW264.7. Enhanced attachment of CHIKV to the primary human monocytes and B cells was observed while increased viral replication was detected in RAW264.7 cells. Blocking of specifc Fc receptors (FcγRs) led to the abrogation of these observations. Furthermore, experimental infection in adult mice showed that animals had higher viral RNA loads and endured more severe joint infammation in the presence of sub-neutralizing concentrations of CHIKV-specifc antibodies. In addition, CHIKV infection in 11 days old mice under enhancing condition resulted in higher muscles viral RNA load detected and death. These observations provide the frst evidence of antibody-mediated enhancement in CHIKV infection and pathogenesis and could also be relevant for other important arboviruses such as Zika virus. -

Florida Arbovirus Surveillance Week 13: March 28-April 3, 2021
Florida Arbovirus Surveillance Week 13: March 28-April 3, 2021 Arbovirus surveillance in Florida includes endemic mosquito-borne viruses such as West Nile virus (WNV), Eastern equine encephalitis virus (EEEV), and St. Louis encephalitis virus (SLEV), as well as exotic viruses such as dengue virus (DENV), chikungunya virus (CHIKV), Zika virus (ZIKV), and California encephalitis group viruses (CEV). Malaria, a parasitic mosquito-borne disease is also included. During the period of March 28- April 3, 2021, the following arboviral activity was recorded in Florida. WNV activity: No human cases of WNV infection were reported this week. No horses with WNV infection were reported this week. No sentinel chickens tested positive for antibodies to WNV this week. In 2021, positive samples from two sentinel chickens has been reported from two counties. SLEV activity: No human cases of SLEV infection were reported this week. No sentinel chickens tested positive for antibodies to SLEV this week. In 2021, no positive samples have been reported. EEEV activity: No human cases of EEEV infection were reported this week. No horses with EEEV infection were reported this week. No sentinel chickens tested positive for antibodies to EEEV this week. In 2021, positive samples from one horse and 14 sentinel chickens have been reported from four counties. International Travel-Associated Dengue Fever Cases: No cases of dengue fever were reported this week in persons that had international travel. In 2021, one travel-associated dengue fever case has been reported. Dengue Fever Cases Acquired in Florida: No cases of locally acquired dengue fever were reported this week. In 2021, no cases of locally acquired dengue fever have been reported. -

Dengue Fever/Severe Dengue Fever/Chikungunya Fever! Report on Suspicion of Infection During Business Hours
Dengue Fever/Severe Dengue Fever/Chikungunya Fever! Report on suspicion of infection during business hours PROTOCOL CHECKLIST Enter available information into Merlin upon receipt of initial report Review background information on the disease (see Section 2), case definitions (see Section 3 for dengue and for chikungunya), and laboratory testing (see Section 4) Forward specimens to the Florida Department of Health (DOH) Bureau of Public Health Laboratories (BPHL) for confirmatory laboratory testing (as needed) Inform local mosquito control personnel of suspected chikungunya or dengue case as soon as possible (if applicable) Inform state Arbovirus Surveillance Coordinator on suspicion of locally acquired arbovirus infection Contact provider (see Section 5A) Interview case-patient Review disease facts (see Section 2) Mode of transmission Ask about exposure to relevant risk factors (see Section 5. Case Investigation) History of travel, outdoor activities, and mosquito bites two weeks prior to onset History of febrile illness or travel for household members or other close contacts in the month prior to onset History of previous arbovirus infection or vaccination (yellow fever, Japanese encephalitis) Provide education on transmission and prevention (see Section 6) Awareness of mosquito-borne diseases Drain standing water at least weekly to stop mosquitoes from multiplying Discard items that collect water and are not being used Cover skin with clothing or Environmental Protection Agency (EPA)-registered repellent such as DEET (N,N-diethyl-meta-toluamide) Use permethrin on clothing (not skin) according to manufacturer’s directions Cover doors and windows with intact screens to keep mosquitoes out of the house Enter additional data obtained from interview into Merlin (see Section 5D) Arrange for a convalescent specimen to be taken (if necessary) Dengue/Chikungunya Guide to Surveillance and Investigation Dengue Fever/Severe Dengue/Chikungunya 1. -

Combatting Malaria, Dengue and Zika Using Nuclear Technology by Nicole Jawerth and Elodie Broussard
Infectious Diseases Combatting malaria, dengue and Zika using nuclear technology By Nicole Jawerth and Elodie Broussard A male Aedes species mosquito. iseases such as malaria, dengue and transcription–polymerase chain reaction (Photo: IAEA) Zika, spread by various mosquito (RT–PCR) (see page 8). Experts across the Dspecies, are wreaking havoc on millions of world have been trained and equipped by lives worldwide. To combat these harmful the IAEA to use this technique for detecting, and often life-threatening diseases, experts tracking and studying pathogens such as in many countries are turning to nuclear and viruses. The diagnostic results help health nuclear-derived techniques for both disease care professionals to provide treatment and detection and insect control. enable experts to track the viruses and take action to control their spread. Dengue and Zika When a new outbreak of disease struck in The dengue virus and Zika virus are mainly 2015 and 2016, physicians weren’t sure of spread by Aedes species mosquitoes, which its cause, but RT–PCR helped to determine are most common in tropical regions. In most that the outbreak was the Zika virus and not cases, the dengue virus causes debilitating another virus such as dengue. RT–PCR was flu-like symptoms, but all four strains of the used to detect the virus in infected people virus also have the potential to cause severe, throughout the epidemic, which was declared life-threatening diseases. In the case of the Zika a public health emergency of international virus, many infected people are asymptomatic concern by the World Health Organization or only have mild symptoms; however, the virus (WHO) in January 2016. -

Dengue Fever (Breakbone Fever, Dengue Hemorrhagic Fever)
Division of Disease Control What Do I Need to Know? Dengue Fever (breakbone fever, dengue hemorrhagic fever) What is Dengue Fever? Dengue fever is a serious form of mosquito-borne disease caused one of four closely related viruses called Flaviviruses. They are named DENV 1, DENV 2, DENV 3, or DENV 4. The disease is found in most tropical and subtropical areas (including some islands in the Caribbean, Mexico, most countries of South and Central America, the Pacific, Asia, parts of tropical Africa and Australia). Almost all cases reported in the continental United States are in travelers who have recently returned from countries where the disease circulates. Dengue is endemic to the U.S. territories of Puerto Rico, the Virgin Islands, and Guam and in recent years non-travel related cases have been found in Texas, Florida, and Hawaii. Who is at risk for Dengue Fever? Dengue fever may occur in people of all ages who are exposed to infected mosquitoes. The disease occurs in areas where the mosquitos that carry dengue circulate, usually during the rainy seasons when mosquito populations are at high numbers. What are the symptoms of Dengue Fever? Dengue fever is characterized by the rapid development of fever that may last from two to seven days, intense headache, joint and muscle pain and a rash. The rash develops on the feet or legs three to four days after the beginning of the fever. Some people with dengue develop dengue hemorrhagic fever (DHF). Symptoms of DHF are characteristic of internal bleeding and include: severe abdominal pain, red patches on skin, bleeding from nose or gums, black stools, vomiting blood, drowsiness, cold and clammy skin and difficulty breathing. -
Weekly Bulletin on Outbreaks
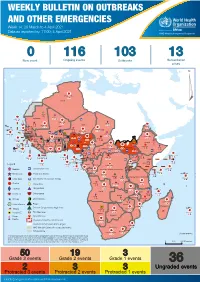
WEEKLY BULLETIN ON OUTBREAKS AND OTHER EMERGENCIES Week 14: 29 March to 4 April 2021 Data as reported by: 17:00; 4 April 2021 REGIONAL OFFICE FOR Africa WHO Health Emergencies Programme 0 116 103 13 New event Ongoing events Outbreaks Humanitarian crises 117 622 3 105 Algeria ¤ 36 13 110 0 5 420 164 Mauritania 7 2 10 501 392 110 0 7 0 Niger 17 927 449 Mali 3 334 10 567 0 6 0 2 079 4 4 595 165 Eritrea Cape Verde 38 520 1 037 Chad Senegal 4 918 185 59 0 Gambia 27 0 3 0 17 125 159 9 761 45 Guinea-Bissau 796 17 7 0 Burkina Faso 225 46 215 189 2 963 0 162 593 2 048 Guinea 12 817 150 12 38 397 1 3 662 66 1 1 23 12 Benin 30 0 Nigeria 1 873 71 0 Ethiopia 420 14 481 5 6 188 15 Sierra Leone Togo 3 473 296 53 920 779 52 14 Ghana 5 245 72 Côte d'Ivoire 10 098 108 14 484 479 63 0 40 0 Liberia 17 0 South Sudan Central African Republic 916 2 45 0 25 0 19 670 120 43 180 237 90 287 740 Cameroon 7 0 28 676 137 5 330 13 138 988 2 224 1 952 87 655 2 51 22 43 0 112 12 6 1 488 6 3 988 79 11 187 6 902 102 Equatorial Guinea Uganda 542 8 Sao Tome and Principe 32 11 2 042 85 41 016 335 Kenya Legend 7 100 90 Gabon Congo 18 504 301 Rwanda Humanitarian crisis 2 212 34 22 482 311 Measles 18 777 111 Democratic Republic of the Congo 9 681 135 Burundi 2 964 6 Monkeypox Ebola virus disease Seychelles 27 930 739 1 525 0 420 29 United Republic of Tanzania Lassa fever Skin disease of unknown etiology 189 0 4 084 20 509 21 Cholera Yellow fever 1 349 5 6 257 229 22 631 542 cVDPV2 Dengue fever 88 930 1 220 Comoros Angola Malawi COVID-19 Chikungunya 33 661 1 123 862 0 3 719 146 -

Guiding Dengue Vaccine Development Using Knowledge Gained from the Success of the Yellow Fever Vaccine
Cellular & Molecular Immunology (2016) 13, 36–46 ß 2015 CSI and USTC. All rights reserved 1672-7681/15 $32.00 www.nature.com/cmi REVIEW Guiding dengue vaccine development using knowledge gained from the success of the yellow fever vaccine Huabin Liang, Min Lee and Xia Jin Flaviviruses comprise approximately 70 closely related RNA viruses. These include several mosquito-borne pathogens, such as yellow fever virus (YFV), dengue virus (DENV), and Japanese encephalitis virus (JEV), which can cause significant human diseases and thus are of great medical importance. Vaccines against both YFV and JEV have been used successfully in humans for decades; however, the development of a DENV vaccine has encountered considerable obstacles. Here, we review the protective immune responses elicited by the vaccine against YFV to provide some insights into the development of a protective DENV vaccine. Cellular & Molecular Immunology (2016) 13, 36–46; doi:10.1038/cmi.2015.76 Keywords: dengue virus; protective immunity; vaccine; yellow fever INTRODUCTION from a viremic patient and is capable of delivering viruses to its Flaviviruses belong to the family Flaviviridae, which includes offspring, thereby amplifying the number of carriers of infec- mosquito-borne pathogens such as yellow fever virus (YFV), tion.6,7 Because international travel has become more frequent, Japanese encephalitis virus (JEV), dengue virus (DENV), and infected vectors can be transported much more easily from an West Nile virus (WNV). Flaviviruses can cause human diseases endemic region to other areas of the world, rendering vector- and thus are considered medically important. According to borne diseases such as dengue fever a global health problem. -

Transmission of Dengue Virus Without a Mosquito Vector: Nosocomial
BRIEF REPORT Transmission of Dengue Virus had recently returned from Peru; the presumed mechanism of transmission was mucocutaneous exposure that occurred dur- without a Mosquito Vector: ing medical care. We describe both cases of dengue fever and Nosocomial Mucocutaneous review the ways that dengue virus can be transmitted without mosquito vectors. Transmission and Other Routes Case reports. Patient 1, a 48-year-old female traveler, pres- of Transmission ented in November 2002 with a 5-day history of fever, myalgia, Downloaded from https://academic.oup.com/cid/article/39/6/e56/359683 by guest on 30 September 2021 and headache. She had recently returned from Iquitos, Peru Lin H. Chen1,2,3 and Mary E. Wilson1,3 (on a trip that lasted from 1 through 10 November), where 1Harvard Medical School, and 2Travel Medicine Center and 3Division of she worked as a nurse on a medical mission and traveled Infectious Diseases, Mount Auburn Hospital, Cambridge, Massachusetts through the Amazon jungles. She stayed in a hotel that had unscreened, open windows. The patient had received hepatitis A virus, hepatitis B virus, and oral typhoid vaccines prior to We report a case of dengue fever in a Boston-area health travel, and she took mefloquine hydrochloride for malaria pro- care worker with no recent history of travel but with mu- phylaxis. She had received yellow fever vaccine in 1997. cocutaneous exposure to infected blood from a febrile trav- At examination, the patient’s temperature was 37.9ЊC. Ab- eler who had recently returned from Peru. Serologic tests normal findings included marked erythroderma, especially on confirmed acute dengue virus infection in both the traveler the patient’s back, and a maculopapular rash along her hairline.