Current Concepts in Dermatology
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Rare Skin Cancers in General Practice
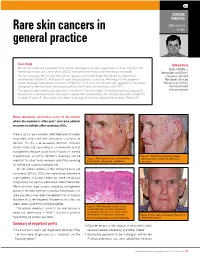
CLINICAL PRACTICE Skin cancer Rare skin cancers in series general practice Case study Anthony Dixon Mr LA has long been troubled with actinic damage to his skin, especially his face. He has had MBBS, FACRRM, is many squamous cell carcinomas (SCCs) removed and many solar keratoses managed. dermasurgeon and Director On this occasion Mr LA had two actinic lesions on his left cheek that failed to respond to of Research, Skin Alert cryotherapy (Figure 1). A biopsy of each site produced a surprise. Histology of the superior Skin Cancer Clinics and lesion revealed sebaceous carcinoma (Figure 2). This is an uncommon yet aggressive cutaneous Skincanceronly, Belmont, malignancy derived from sebaceous glands. The 5 year survival rate is 60–70%. Victoria. anthony@ The tumour was widely excised with a minimum 10 mm margin. A multidisciplinary approach skincanceronly.com resulted in a decision not to proceed to adjunctive radiotherapy. The wound was well healed by 8 weeks (Figure 3). Four years on there is no sign of local or regional recurrence (Figure 4). Many sebaceous carcinomas occur on the eyelids where the outcome is often poor;1 and some patients are prone to multiple other cutaneous SCCs. There is also a rare syndrome called Muir-torre of visceral neoplasms associated with sebaceous carcinoma on the skin.2 As this is an autosomal dominant condition, family history and counselling is an esssential part of management (enquire about family history of internal malignancies). A family member's diagnosis can be Figure 3. Satisfactory healing 8 weeks Figure 1. Two actinic lesions on the left face following wide excision of sebaceous important for other family members and offers screening have failed to respond to cryotherapy carcinoma for internal and cutaneous malignancies. -

General Pathomorpholog.Pdf
Ukrаiniаn Medicаl Stomаtologicаl Аcаdemy THE DEPАRTАMENT OF PАTHOLOGICАL АNАTOMY WITH SECTIONSL COURSE MАNUАL for the foreign students GENERАL PАTHOMORPHOLOGY Poltаvа-2020 УДК:616-091(075.8) ББК:52.5я73 COMPILERS: PROFESSOR I. STАRCHENKO ASSOCIATIVE PROFESSOR O. PRYLUTSKYI АSSISTАNT A. ZADVORNOVA ASSISTANT D. NIKOLENKO Рекомендовано Вченою радою Української медичної стоматологічної академії як навчальний посібник для іноземних студентів – здобувачів вищої освіти ступеня магістра, які навчаються за спеціальністю 221 «Стоматологія» у закладах вищої освіти МОЗ України (протокол №8 від 11.03.2020р) Reviewers Romanuk A. - MD, Professor, Head of the Department of Pathological Anatomy, Sumy State University. Sitnikova V. - MD, Professor of Department of Normal and Pathological Clinical Anatomy Odessa National Medical University. Yeroshenko G. - MD, Professor, Department of Histology, Cytology and Embryology Ukrainian Medical Dental Academy. A teaching manual in English, developed at the Department of Pathological Anatomy with a section course UMSA by Professor Starchenko II, Associative Professor Prylutsky OK, Assistant Zadvornova AP, Assistant Nikolenko DE. The manual presents the content and basic questions of the topic, practical skills in sufficient volume for each class to be mastered by students, algorithms for describing macro- and micropreparations, situational tasks. The formulation of tests, their number and variable level of difficulty, sufficient volume for each topic allows to recommend them as preparation for students to take the licensed integrated exam "STEP-1". 2 Contents p. 1 Introduction to pathomorphology. Subject matter and tasks of 5 pathomorphology. Main stages of development of pathomorphology. Methods of pathanatomical diagnostics. Methods of pathomorphological research. 2 Morphological changes of cells as response to stressor and toxic damage 8 (parenchimatouse / intracellular dystrophies). -

Atypical Compound Nevus Arising in Mature Cystic Ovarian Teratoma
J Cutan Pathol 2005: 32: 71–123 Copyright # Blackwell Munksgaard 2005 Blackwell Munksgaard. Printed in Denmark Journal of Cutaneous Pathology Abstracts of the Papers Presented at the 41st Annual Meeting of The American Society of Dermatopathology Westin Copley Place Boston, Massachusetts, USA October 14–17, 2004 These abstracts were presented in oral or poster format at the 41st Annual Meeting of The American Society of Dermatopathology on October 14–17, 2004. They are listed on the following pages in alphabetical order by the first author’s last name. 71 Abstracts IN SITU HYBRIDIZATION IS A VALUABLE DIAGNOSTIC A 37-year-old woman with diagnosis of Sjogren’s syndrome (SS) TOOL IN CUTANEOUS DEEP FUNGAL INFECTIONS presented with asymptomatic non-palpable purpura of the lower J.J. Abbott1, K.L. Hamacher2,A.G.Bridges2 and I. Ahmed1,2 extremities. Biopsy of a purpuric macule revealed a perivascular Departments of Laboratory Medicine and Pathology1 and and focally nodular lymphocytic infiltrate with large numbers of Dermatology2, plasma cells, seemingly around eccrine glands. There was no vascu- litis. The histologic findings in the skin were strikingly similar to those Mayo Clinic and Mayo Foundation, Rochester, MN, USA of salivary, parotid, and other ‘‘secretory’’ glands affected in SS. The cutaneous manifestations of SS highlighted in textbooks include Dimorphic fungal infections (histoplasmosis, blastomycosis, coccidiomy- xerosis, annular erythema, small-vessel vasculitis, and pigmented cosis, and cryptococcosis) can occur in immunocompromised and purpura. This case illustrates that purpura in skin of patients with healthy individuals. Cutaneous involvement is often secondary and SS may be caused by a peri-eccrine plasma-rich infiltrate. -

Atypical Fibroxanthoma - Histological Diagnosis, Immunohistochemical Markers and Concepts of Therapy
ANTICANCER RESEARCH 35: 5717-5736 (2015) Review Atypical Fibroxanthoma - Histological Diagnosis, Immunohistochemical Markers and Concepts of Therapy MICHAEL KOCH1, ANNE J. FREUNDL2, ABBAS AGAIMY3, FRANKLIN KIESEWETTER2, JULIAN KÜNZEL4, IWONA CICHA1* and CHRISTOPH ALEXIOU1* 1Department of Otorhinolaryngology, Head and Neck Surgery, University Hospital Erlangen, Erlangen, Germany; 2Dermatology Clinic, 3Institute of Pathology, and 4ENT Department, University Hospital Mainz, Mainz, Germany Abstract. Background: Atypical fibroxanthoma (AFX) is an in 1962 (2). The name 'atypical fibroxanthoma' reflects the uncommon, rapidly growing cutaneous neoplasm of uncertain tumor composition, containing mainly xanthomatous-looking histogenesis. Thus far, there are no guidelines for diagnosis and cells and a varying proportion of fibrocytoid cells with therapy of this tumor. Patients and Methods: We included 18 variable, but usually marked cellular atypia (3). patients with 21 AFX, and 2,912 patients with a total of 2,939 According to previous reports, AFX chiefly occurs in the AFX cited in the literature between 1962 and 2014. Results: In sun-exposed head-and-neck area, especially in elderly males our cohort, excision with safety margin was performed in 100% (3). There are two disease peaks described: one within the 5th of primary tumors. Local recurrences were observed in 25% of to 7th decade of life and another one between the 7th and 8th primary tumors and parotid metastases in 5%. Ten-year disease- decade. The former disease peak is associated with lower specific survival was 100%. The literature research yielded 280 tumor frequency (21.8%) and tumors that do not necessarily relevant publications. Over 90% of the reported cases were manifest on skin areas exposed to sunlight (4). -

Atypical Fibroxanthoma and Pleomorphic Dermal Sarcoma - Two Stages of the Same Disease?
Case Report World Journal of Oral and Maxillofacial Surgery Published: 12 Jul, 2018 Atypical Fibroxanthoma and Pleomorphic Dermal Sarcoma - Two Stages of the Same Disease? Farhana Kapasi1*, Marta Cabral2, Phillip Ameerally1 and Antonia Barbieri1 1Department of Oral and Maxillofacial Surgery, Northampton General Hospital, UK 2Marta Cabral, The Royal Devon and Exeter NHS Foundation Trust, UK Abstract Atypical Fibroxanthoma and Pleomorphic Dermal Sarcoma are rare cutaneous neoplasm's which share clinical and Histopathological features which can pose a diagnostic challenge. Atypical Fibroxanthoma has been considered a low-grade malignancy whereas Pleomorphic Dermal Sarcoma has been considered high grade and aggressive. We report a case of an 83-year-old male with a history of Actinic Keratosis who presented with an erythematous papule on the right parietal scalp. Histopathological diagnosis was Atypical Fibroxanthoma. Seven months postoperatively, the patient developed a rapidly growing purple nodule at the operative site which was adherent to the skull. Histopathological diagnosis was Pleomorphic Dermal Sarcoma with bone involvement. We suggest that the recurrence rate and low aggressive potential of Atypical Fibroxanthoma may have been underestimated, as these tumours are rare and have not been widely reported in the literature. In this case, the tumour recurred following complete excision. The recurrence was the more infiltrative Pleomorphic Dermal Sarcoma, which reinforces the hypotheses that Atypical Fibroxanthoma may be the precursor lesion of Pleomorphic Dermal Sarcoma and that these are indeed two stages of the same disease rather than separate entities. Keywords: General dermatology; Medical dermatology; Head and neck oncology Introduction OPEN ACCESS Atypical Fibroxanthoma is a rare cutaneous tumour first described in 1963 by Elson Helwig [1]. -

Cutaneous Neoplasms
torr CALIFORNIA TUMOR TISSUE REGISTRY 1 03RD SEMI-ANNUAL CANCER SEMINAR ON CUTANEOUS NEOPLASMS CASE HISTORIES 00•MODERAT.0RS: . PHILIP E. LE~0FJ', M.Q. Dir;ector O:f Oermatopafholo.gy ;Ser:Vice Associate Professor of Clinical Pathology U.C.S.F.- Elermatopa~hology San Francisco, ·californla and TIMGTH1f' H. MCG~WMON'f,, M ~D. Assistant Clinical Professor U.C~S.F. - Dermatopathology San Francisco, California December 7, 1997 Sheraton Palace Hotel San Francisco, California PLATFORM CHAIR: CLAUDE 0. BURDICK, M.D. Director of laboratory ValleyCare Health System Pleasanton, California CASE RISTORJES 10.3"" Semi-Annual Seminar (Due to in$uffient material, Case 115 is • compo~ite to two ca!ICll with an identical diagnosis, Ace. #15523 and Ace #12395.) Ca.c 1#1 - As:c 1#28070: The patient was a 12-ycaro{)ld male who had a fairly long history ofa very small bump in the scalp of the temporal area, which had recently become greally enlarged. The submitting denna!ologist mentioned that this was a soliwy lesion, with no other lesions apparent (Contributed by Prescott Rasmussen, MD.) c-111- As:c #11543: The patient was a 60-year-old Caucasian female wbo presented with a S.O em right suprapalellar subcutaneous mass which was reported to be present and gradually increasing in size for a period of approximately rn·o years. There was no history of prior trauma, and the remainder ofthe clinical history and physical findings wcze uoremarialble. An cxeisional biopsy was performed. The specimeD consisted ofa 4.S x 1.1 em elliptical segment ofeentnllly dimpled skin which surmowlted a S.3 x 4.4 x 3.6 em delicately encapsulated. -

Myxofibrosarcoma Mimicking Inflammatory Lesion Of
applied sciences Communication Myxofibrosarcoma Mimicking Inflammatory Lesion of Temporomandibular Joint—Case Presentation Dawid Zagacki 1,*, Krzysztof Sztychny 2, Marta Tyndorf 2, Robert Bibik 3, Dominik Sygut 4 and Marcin Kozakiewicz 2 1 International Doctoral School, Medical University of Łód´z,Pl. Hallera 1, 90-647 Łód´z,Poland 2 Department of Maxillofacial Surgery, Medical University of Łód´z,Pl. Hallera 1, 90-647 Łód´z,Poland; [email protected] (K.S.); [email protected] (M.T.); [email protected] (M.K.) 3 Department of Radiation Oncology, Radom’s Oncology Centre, 26-600 Radom, Poland; [email protected] 4 Department of Clinical Patomorphology and Cytopathology, Medical University of Lodz, ul. Zeromskiego 113, 90-549 Lodz, Poland; [email protected] * Correspondence: [email protected] Abstract: Treating oncologic patients remains a challenge for surgeons aiming to provide patients with safe margins of resection while maintaining the highest possible quality of life. The latter, in the case of malignancies, requires using sophisticated methods of reconstruction. Thus, we present a case of a 75-year-old patient treated in our department with a rare neoplasm in the region of the temporomandibular joint—a myxofibrosarcoma that was mimicking an inflammatory lesion. The patient underwent two surgeries—firstly alloplasty of the TMJ due to the suspicion of an inflammatory lesion, lately extended to the resection of glenoid fossa and subtemporal fossa contents when the mandible was reconstructed using UHMW-PE (ultra-high molecular weight polyethylene). Citation: Zagacki, D.; Sztychny, K.; The patient was also referred for adjuvant radiotherapy and has remained disease-free for over Tyndorf, M.; Bibik, R.; Sygut, D.; 96 months with very good aesthetics and function of the mandible. -

Tc. Süleyman Demirel Üniversitesi Sosyal Bilmler Enstitüsü Tarih Anabilim Dali
TC. SÜLEYMAN DEMİREL ÜNİVERSİTESİ SOSYAL BİLMLER ENSTİTÜSÜ TARİH ANABİLİM DALI ORTAÇAĞ ANADOLU’SUNDA İSTANBUL İLE AFYONKARAHİSAR ARASINDAKİ ASKERİ YOL GÜZERGÂHLARI Seda EDİZ 1130204513 YÜKSEK LİSANS TEZİ DANIŞMAN Doç. Dr. Abdullah BAKIR ISPARTA-2019 (Ediz, Seda, Ortaçağ Anadolu’sunda İstanbul ile Afyonkarahisar Arasındaki Askeri Yol Güzergâhları, Yüksek Lisans Tezi, Isparta, 2018) ÖZET Yapılan bu tez çalışmasında İstanbul-Afyonkarahisar arasındaki askeri yol güzergahları ve bu iki şehir arasında kalan bölgenin tarihi coğrafyası hakkında bilgiler verilmektedir. Bu bağlamda öncelikle Eski Çağda bölgenin tarihi coğrafyası ve bu dönemde gerçekleşmiş, söz konusu saha üzerinden yapılan veya bu yollardan geçen savaşlar ele alınmıştır. Ardından Orta Çağda gerçekleşen Bizans Selçuklu mücadeleleri sırasında kullanılan yol güzergahları değerlendirilmiş sonrasında ise I., II., ve III. Haçlı Seferleri esnasında kullanılan yol güzergahları ana kaynaklar ve topografik eserler yardımı ile incelenmeye alınmıştır. Çalışmada konunun aydınlatılmasına yardımcı olması açısından söz konusu sahanın tarihi coğrafyası, Bithynia, Mysia, Troas, Aiolis, Lydia, Ionia ve Phrygia olacak şekilde sırasıyla ele alınmıştır. Tarihi coğrafya incelendikten sonra Eski Çağda bölgeden geçen askeri yol güzergahını kullanmış orduların savaşlarına kronolojik olarak yer verilmiştir. Öncelikle Pers kral yolu değerlendirilmiş ardından, Pers Kralı Kserkses’in Yunanistan Seferi (MÖ. 481-480) sırasında Anadolu’da izlediği yol güzergahı ve savaş esnasında yaşanan olaylara yer verilmiştir. -

The 2020 WHO Classification of Soft Tissue Tumours: News and Perspectives
PATHOLOGICA 2021;113:70-84; DOI: 10.32074/1591-951X-213 Review The 2020 WHO Classification of Soft Tissue Tumours: news and perspectives Marta Sbaraglia1, Elena Bellan1, Angelo P. Dei Tos1,2 1 Department of Pathology, Azienda Ospedale Università Padova, Padova, Italy; 2 Department of Medicine, University of Padua School of Medicine, Padua, Italy Summary Mesenchymal tumours represent one of the most challenging field of diagnostic pathol- ogy and refinement of classification schemes plays a key role in improving the quality of pathologic diagnosis and, as a consequence, of therapeutic options. The recent publica- tion of the new WHO classification of Soft Tissue Tumours and Bone represents a major step toward improved standardization of diagnosis. Importantly, the 2020 WHO classi- fication has been opened to expert clinicians that have further contributed to underline the key value of pathologic diagnosis as a rationale for proper treatment. Several rel- evant advances have been introduced. In the attempt to improve the prediction of clinical behaviour of solitary fibrous tumour, a risk assessment scheme has been implemented. NTRK-rearranged soft tissue tumours are now listed as an “emerging entity” also in con- sideration of the recent therapeutic developments in terms of NTRK inhibition. This deci- sion has been source of a passionate debate regarding the definition of “tumour entity” as well as the consequences of a “pathology agnostic” approach to precision oncology. In consideration of their distinct clinicopathologic features, undifferentiated round cell sarcomas are now kept separate from Ewing sarcoma and subclassified, according to the underlying gene rearrangements, into three main subgroups (CIC, BCLR and not Received: October 14, 2020 ETS fused sarcomas) Importantly, In order to avoid potential confusion, tumour entities Accepted: October 19, 2020 such as gastrointestinal stroma tumours are addressed homogenously across the dif- Published online: November 3, 2020 ferent WHO fascicles. -

2016 Essentials of Dermatopathology Slide Library Handout Book
2016 Essentials of Dermatopathology Slide Library Handout Book April 8-10, 2016 JW Marriott Houston Downtown Houston, TX USA CASE #01 -- SLIDE #01 Diagnosis: Nodular fasciitis Case Summary: 12 year old male with a rapidly growing temple mass. Present for 4 weeks. Nodular fasciitis is a self-limited pseudosarcomatous proliferation that may cause clinical alarm due to its rapid growth. It is most common in young adults but occurs across a wide age range. This lesion is typically 3-5 cm and composed of bland fibroblasts and myofibroblasts without significant cytologic atypia arranged in a loose storiform pattern with areas of extravasated red blood cells. Mitoses may be numerous, but atypical mitotic figures are absent. Nodular fasciitis is a benign process, and recurrence is very rare (1%). Recent work has shown that the MYH9-USP6 gene fusion is present in approximately 90% of cases, and molecular techniques to show USP6 gene rearrangement may be a helpful ancillary tool in difficult cases or on small biopsy samples. Weiss SW, Goldblum JR. Enzinger and Weiss’s Soft Tissue Tumors, 5th edition. Mosby Elsevier. 2008. Erickson-Johnson MR, Chou MM, Evers BR, Roth CW, Seys AR, Jin L, Ye Y, Lau AW, Wang X, Oliveira AM. Nodular fasciitis: a novel model of transient neoplasia induced by MYH9-USP6 gene fusion. Lab Invest. 2011 Oct;91(10):1427-33. Amary MF, Ye H, Berisha F, Tirabosco R, Presneau N, Flanagan AM. Detection of USP6 gene rearrangement in nodular fasciitis: an important diagnostic tool. Virchows Arch. 2013 Jul;463(1):97-8. CONTRIBUTED BY KAREN FRITCHIE, MD 1 CASE #02 -- SLIDE #02 Diagnosis: Cellular fibrous histiocytoma Case Summary: 12 year old female with wrist mass. -

Wednesday Slide Conference 2008-2009
PROCEEDINGS DEPARTMENT OF VETERINARY PATHOLOGY WEDNESDAY SLIDE CONFERENCE 2008-2009 ARMED FORCES INSTITUTE OF PATHOLOGY WASHINGTON, D.C. 20306-6000 2009 ML2009 Armed Forces Institute of Pathology Department of Veterinary Pathology WEDNESDAY SLIDE CONFERENCE 2008-2009 100 Cases 100 Histopathology Slides 249 Images PROCEEDINGS PREPARED BY: Todd Bell, DVM Chief Editor: Todd O. Johnson, DVM, Diplomate ACVP Copy Editor: Sean Hahn Layout and Copy Editor: Fran Card WSC Online Management and Design Scott Shaffer ARMED FORCES INSTITUTE OF PATHOLOGY Washington, D.C. 20306-6000 2009 ML2009 i PREFACE The Armed Forces Institute of Pathology, Department of Veterinary Pathology has conducted a weekly slide conference during the resident training year since 12 November 1953. This ever- changing educational endeavor has evolved into the annual Wednesday Slide Conference program in which cases are presented on 25 Wednesdays throughout the academic year and distributed to 135 contributing military and civilian institutions from around the world. Many of these institutions provide structured veterinary pathology resident training programs. During the course of the training year, histopathology slides, digital images, and histories from selected cases are distributed to the participating institutions and to the Department of Veterinary Pathology at the AFIP. Following the conferences, the case diagnoses, comments, and reference listings are posted online to all participants. This study set has been assembled in an effort to make Wednesday Slide Conference materials available to a wider circle of interested pathologists and scientists, and to further the education of veterinary pathologists and residents-in-training. The number of histopathology slides that can be reproduced from smaller lesions requires us to limit the number of participating institutions. -

5–21–10 Vol. 75 No. 98 Friday May 21, 2010 Pages 28463–28750
5–21–10 Friday Vol. 75 No. 98 May 21, 2010 Pages 28463–28750 VerDate Mar 15 2010 19:10 May 20, 2010 Jkt 220001 PO 00000 Frm 00001 Fmt 4710 Sfmt 4710 E:\FR\FM\21MYWS.LOC 21MYWS hsrobinson on DSK69SOYB1PROD with PROPOSALS6 II Federal Register / Vol. 75, No. 98 / Friday, May 21, 2010 The FEDERAL REGISTER (ISSN 0097–6326) is published daily, SUBSCRIPTIONS AND COPIES Monday through Friday, except official holidays, by the Office of the Federal Register, National Archives and Records PUBLIC Administration, Washington, DC 20408, under the Federal Register Subscriptions: Act (44 U.S.C. Ch. 15) and the regulations of the Administrative Paper or fiche 202–512–1800 Committee of the Federal Register (1 CFR Ch. I). The Assistance with public subscriptions 202–512–1806 Superintendent of Documents, U.S. Government Printing Office, Washington, DC 20402 is the exclusive distributor of the official General online information 202–512–1530; 1–888–293–6498 edition. Periodicals postage is paid at Washington, DC. Single copies/back copies: The FEDERAL REGISTER provides a uniform system for making Paper or fiche 202–512–1800 available to the public regulations and legal notices issued by Assistance with public single copies 1–866–512–1800 Federal agencies. These include Presidential proclamations and (Toll-Free) Executive Orders, Federal agency documents having general FEDERAL AGENCIES applicability and legal effect, documents required to be published by act of Congress, and other Federal agency documents of public Subscriptions: interest. Paper or fiche 202–741–6005 Documents are on file for public inspection in the Office of the Assistance with Federal agency subscriptions 202–741–6005 Federal Register the day before they are published, unless the issuing agency requests earlier filing.