Cutaneous Neoplasms
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Rare Skin Cancers in General Practice
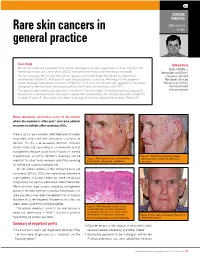
CLINICAL PRACTICE Skin cancer Rare skin cancers in series general practice Case study Anthony Dixon Mr LA has long been troubled with actinic damage to his skin, especially his face. He has had MBBS, FACRRM, is many squamous cell carcinomas (SCCs) removed and many solar keratoses managed. dermasurgeon and Director On this occasion Mr LA had two actinic lesions on his left cheek that failed to respond to of Research, Skin Alert cryotherapy (Figure 1). A biopsy of each site produced a surprise. Histology of the superior Skin Cancer Clinics and lesion revealed sebaceous carcinoma (Figure 2). This is an uncommon yet aggressive cutaneous Skincanceronly, Belmont, malignancy derived from sebaceous glands. The 5 year survival rate is 60–70%. Victoria. anthony@ The tumour was widely excised with a minimum 10 mm margin. A multidisciplinary approach skincanceronly.com resulted in a decision not to proceed to adjunctive radiotherapy. The wound was well healed by 8 weeks (Figure 3). Four years on there is no sign of local or regional recurrence (Figure 4). Many sebaceous carcinomas occur on the eyelids where the outcome is often poor;1 and some patients are prone to multiple other cutaneous SCCs. There is also a rare syndrome called Muir-torre of visceral neoplasms associated with sebaceous carcinoma on the skin.2 As this is an autosomal dominant condition, family history and counselling is an esssential part of management (enquire about family history of internal malignancies). A family member's diagnosis can be Figure 3. Satisfactory healing 8 weeks Figure 1. Two actinic lesions on the left face following wide excision of sebaceous important for other family members and offers screening have failed to respond to cryotherapy carcinoma for internal and cutaneous malignancies. -

Atypical Compound Nevus Arising in Mature Cystic Ovarian Teratoma
J Cutan Pathol 2005: 32: 71–123 Copyright # Blackwell Munksgaard 2005 Blackwell Munksgaard. Printed in Denmark Journal of Cutaneous Pathology Abstracts of the Papers Presented at the 41st Annual Meeting of The American Society of Dermatopathology Westin Copley Place Boston, Massachusetts, USA October 14–17, 2004 These abstracts were presented in oral or poster format at the 41st Annual Meeting of The American Society of Dermatopathology on October 14–17, 2004. They are listed on the following pages in alphabetical order by the first author’s last name. 71 Abstracts IN SITU HYBRIDIZATION IS A VALUABLE DIAGNOSTIC A 37-year-old woman with diagnosis of Sjogren’s syndrome (SS) TOOL IN CUTANEOUS DEEP FUNGAL INFECTIONS presented with asymptomatic non-palpable purpura of the lower J.J. Abbott1, K.L. Hamacher2,A.G.Bridges2 and I. Ahmed1,2 extremities. Biopsy of a purpuric macule revealed a perivascular Departments of Laboratory Medicine and Pathology1 and and focally nodular lymphocytic infiltrate with large numbers of Dermatology2, plasma cells, seemingly around eccrine glands. There was no vascu- litis. The histologic findings in the skin were strikingly similar to those Mayo Clinic and Mayo Foundation, Rochester, MN, USA of salivary, parotid, and other ‘‘secretory’’ glands affected in SS. The cutaneous manifestations of SS highlighted in textbooks include Dimorphic fungal infections (histoplasmosis, blastomycosis, coccidiomy- xerosis, annular erythema, small-vessel vasculitis, and pigmented cosis, and cryptococcosis) can occur in immunocompromised and purpura. This case illustrates that purpura in skin of patients with healthy individuals. Cutaneous involvement is often secondary and SS may be caused by a peri-eccrine plasma-rich infiltrate. -

Atypical Fibroxanthoma - Histological Diagnosis, Immunohistochemical Markers and Concepts of Therapy
ANTICANCER RESEARCH 35: 5717-5736 (2015) Review Atypical Fibroxanthoma - Histological Diagnosis, Immunohistochemical Markers and Concepts of Therapy MICHAEL KOCH1, ANNE J. FREUNDL2, ABBAS AGAIMY3, FRANKLIN KIESEWETTER2, JULIAN KÜNZEL4, IWONA CICHA1* and CHRISTOPH ALEXIOU1* 1Department of Otorhinolaryngology, Head and Neck Surgery, University Hospital Erlangen, Erlangen, Germany; 2Dermatology Clinic, 3Institute of Pathology, and 4ENT Department, University Hospital Mainz, Mainz, Germany Abstract. Background: Atypical fibroxanthoma (AFX) is an in 1962 (2). The name 'atypical fibroxanthoma' reflects the uncommon, rapidly growing cutaneous neoplasm of uncertain tumor composition, containing mainly xanthomatous-looking histogenesis. Thus far, there are no guidelines for diagnosis and cells and a varying proportion of fibrocytoid cells with therapy of this tumor. Patients and Methods: We included 18 variable, but usually marked cellular atypia (3). patients with 21 AFX, and 2,912 patients with a total of 2,939 According to previous reports, AFX chiefly occurs in the AFX cited in the literature between 1962 and 2014. Results: In sun-exposed head-and-neck area, especially in elderly males our cohort, excision with safety margin was performed in 100% (3). There are two disease peaks described: one within the 5th of primary tumors. Local recurrences were observed in 25% of to 7th decade of life and another one between the 7th and 8th primary tumors and parotid metastases in 5%. Ten-year disease- decade. The former disease peak is associated with lower specific survival was 100%. The literature research yielded 280 tumor frequency (21.8%) and tumors that do not necessarily relevant publications. Over 90% of the reported cases were manifest on skin areas exposed to sunlight (4). -

Atypical Fibroxanthoma and Pleomorphic Dermal Sarcoma - Two Stages of the Same Disease?
Case Report World Journal of Oral and Maxillofacial Surgery Published: 12 Jul, 2018 Atypical Fibroxanthoma and Pleomorphic Dermal Sarcoma - Two Stages of the Same Disease? Farhana Kapasi1*, Marta Cabral2, Phillip Ameerally1 and Antonia Barbieri1 1Department of Oral and Maxillofacial Surgery, Northampton General Hospital, UK 2Marta Cabral, The Royal Devon and Exeter NHS Foundation Trust, UK Abstract Atypical Fibroxanthoma and Pleomorphic Dermal Sarcoma are rare cutaneous neoplasm's which share clinical and Histopathological features which can pose a diagnostic challenge. Atypical Fibroxanthoma has been considered a low-grade malignancy whereas Pleomorphic Dermal Sarcoma has been considered high grade and aggressive. We report a case of an 83-year-old male with a history of Actinic Keratosis who presented with an erythematous papule on the right parietal scalp. Histopathological diagnosis was Atypical Fibroxanthoma. Seven months postoperatively, the patient developed a rapidly growing purple nodule at the operative site which was adherent to the skull. Histopathological diagnosis was Pleomorphic Dermal Sarcoma with bone involvement. We suggest that the recurrence rate and low aggressive potential of Atypical Fibroxanthoma may have been underestimated, as these tumours are rare and have not been widely reported in the literature. In this case, the tumour recurred following complete excision. The recurrence was the more infiltrative Pleomorphic Dermal Sarcoma, which reinforces the hypotheses that Atypical Fibroxanthoma may be the precursor lesion of Pleomorphic Dermal Sarcoma and that these are indeed two stages of the same disease rather than separate entities. Keywords: General dermatology; Medical dermatology; Head and neck oncology Introduction OPEN ACCESS Atypical Fibroxanthoma is a rare cutaneous tumour first described in 1963 by Elson Helwig [1]. -

Abstract Case Synopsis
Volume 20 Number 4 April 2014 Case presentation Solitary papule over scalp 1 1 1 2 Nidhi Singh , Laxmisha Chandrashekar , Devinder Mohan Thappa , Rakhee Kar Dermatology Online Journal 20 (4): 6 1Department of Dermatology, Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry, India 2Department of Pathology, Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry, India Correspondence: Laxmisha Chandrashekar Associate Professor, Department of Dermatology, Jawaharlal Institute of Postgraduate Medical Education and Research Puducherry, India [email protected] Abstract Folliculosebaceous cystic hamartoma (FSCH) is a rare cutaneous hamartoma characterized by follicular, sebaceous, and mesenchymal elements. Folliculosebaceous cystic hamartoma is probably not as rare as previously thought and its inclusion in the differential diagnosis of asymptomatic skin colored papules or nodules is warranted, especially if it is present in the head and neck region. Key words: folliculosebaceous cystic hamartoma, sebaceous tumor Case synopsis A 33-year-old woman presented with an asymptomatic papule that had persisted for the past 11 years. She noticed slow growth in the size of the lesion over the past 5 years. Repeated trauma to the papule while combing her hair resulted in discomfort. Physical examination revealed a single non-tender, skin colored, firm, hairless papule of 5 x 4 x 3 mm diameter over the vertex of the scalp (Figure 1). It was excised and sent for histopathological examination (Figure 2, 3 & 4). Histopathological examination revealed a dilated follicular cystic structure with numerous sebaceous lobules radiating out from it in the dermis (Figure 2). The cyst showed a predominantly infundibular keratinization (Figure 3). This folliculosebaceous structure was surrounded by increased collagen in the dermis (Figure 2) and clefts were visible between the folliculosebaceous structures and the surrounding stroma (Figure 4). -

Myxofibrosarcoma Mimicking Inflammatory Lesion Of
applied sciences Communication Myxofibrosarcoma Mimicking Inflammatory Lesion of Temporomandibular Joint—Case Presentation Dawid Zagacki 1,*, Krzysztof Sztychny 2, Marta Tyndorf 2, Robert Bibik 3, Dominik Sygut 4 and Marcin Kozakiewicz 2 1 International Doctoral School, Medical University of Łód´z,Pl. Hallera 1, 90-647 Łód´z,Poland 2 Department of Maxillofacial Surgery, Medical University of Łód´z,Pl. Hallera 1, 90-647 Łód´z,Poland; [email protected] (K.S.); [email protected] (M.T.); [email protected] (M.K.) 3 Department of Radiation Oncology, Radom’s Oncology Centre, 26-600 Radom, Poland; [email protected] 4 Department of Clinical Patomorphology and Cytopathology, Medical University of Lodz, ul. Zeromskiego 113, 90-549 Lodz, Poland; [email protected] * Correspondence: [email protected] Abstract: Treating oncologic patients remains a challenge for surgeons aiming to provide patients with safe margins of resection while maintaining the highest possible quality of life. The latter, in the case of malignancies, requires using sophisticated methods of reconstruction. Thus, we present a case of a 75-year-old patient treated in our department with a rare neoplasm in the region of the temporomandibular joint—a myxofibrosarcoma that was mimicking an inflammatory lesion. The patient underwent two surgeries—firstly alloplasty of the TMJ due to the suspicion of an inflammatory lesion, lately extended to the resection of glenoid fossa and subtemporal fossa contents when the mandible was reconstructed using UHMW-PE (ultra-high molecular weight polyethylene). Citation: Zagacki, D.; Sztychny, K.; The patient was also referred for adjuvant radiotherapy and has remained disease-free for over Tyndorf, M.; Bibik, R.; Sygut, D.; 96 months with very good aesthetics and function of the mandible. -

Trichoblastoma Arising from the Nevus Sebaceus of Jadassohn
Open Access Case Report DOI: 10.7759/cureus.15325 Trichoblastoma Arising From the Nevus Sebaceus of Jadassohn Fatimazahra Chahboun 1 , Madiha Eljazouly 1 , Mounia Elomari 2 , Faycal Abbad 3 , Soumiya Chiheb 1 1. Dermatology Unit, Cheikh Khalifa International University Hospital, Mohammed VI University of Health Sciences, Casablanca, MAR 2. Plastic and Reconstructive Surgery, Cheikh Khalifa International University Hospital, Mohammed VI University of Health Sciences, Casablanca, MAR 3. Pathology, Cheikh Khalifa International University Hospital, Mohammed VI University of Health Sciences, Casablanca, MAR Corresponding author: Fatimazahra Chahboun, [email protected] Abstract Trichoblastoma is a rare benign skin adnexal tumour, belonging to the category of trichogenic tumours. The clinical and histological findings may often be confused with basal cell carcinoma, a malignant epidermal skin tumour. We report here a case of a 70-year-old man presented with a dome-shaped, dark-pigmented nodule within a yellowish hairless plaque on the scalp. The plaque had existed since childhood. However, the central pigmented nodule began appearing three months ago and enlarging gradually. The patient had no medical history. Furthermore the physical examination revealed a translucent, verrucous, and yellowish plaque, with central and pigmented nodule measuring 0.7 × 0.5 cm. Also basal cell carcinoma and trichoblastoma’s diagnosis were discussed. The patient was subsequently referred to the plastic surgery department, where he underwent a total excision. The histological examination was in favour of trichoblastoma arising from the nevus sebaceus. After 24 months of checking, no recurrence was observed. Trichoblastoma is a benign adnexal tumour. Its progression to malignant trichoblastoma (or trichoblastic carcinoma) is possible, but remains exceptional. -

The Best Diagnosis Is: H&E, Original Magnification 2
Dermatopathology Diagnosis The best diagnosis is: H&E, original magnification 2. a. adenoid cysticcopy carcinoma arising within a spiradenoma b. cylindroma and spiradenoma collision tumor c. microcysticnot change within a spiradenoma d. mucinous carcinoma arising within a spiradenoma Doe. trichoepithelioma and spiradenoma collision tumor CUTIS H&E, original magnification 100. PLEASE TURN TO PAGE 211 FOR DERMATOPATHOLOGY DIAGNOSIS DISCUSSION Amanda F. Marsch, MD; Jeffrey B. Shackelton, MD; Dirk M. Elston, MD Dr. Marsch is from the Department of Dermatology, University of Illinois at Chicago. Drs. Shackelton and Elston are from the Ackerman Academy of Dermatopathology, New York, New York. The authors report no conflict of interest. Correspondence: Amanda F. Marsch, MD, University of Illinois at Chicago, 808 S Wood St, Chicago, IL 60612 ([email protected]). 192 CUTIS® WWW.CUTIS.COM Copyright Cutis 2015. No part of this publication may be reproduced, stored, or transmitted without the prior written permission of the Publisher. Dermatopathology Diagnosis Discussion Trichoepithelioma and Spiradenoma Collision Tumor he coexistence of more than one cutaneous adnexal neoplasm in a single biopsy specimen Tis unusual and is most frequently recognized in the context of a nevus sebaceous or Brooke-Spiegler syndrome, an autosomal-dominant inherited disease characterized by cutaneous adnexal neoplasms, most commonly cylindromas and trichoepitheliomas.1-3 Brooke-Spiegler syndrome is caused by germline muta- tions in the cylindromatosis gene, CYLD, located on band 16q12; it functions as a tumor suppressor gene and has regulatory roles in development, immunity, and inflammation.1 Weyers et al3 first recognized the tendency for adnexal collision tumors to present in patients with Brooke-Spiegler syndrome; they reported a patient with Brooke-Spiegler syndrome with spirad- Figure 1. -

The 2020 WHO Classification of Soft Tissue Tumours: News and Perspectives
PATHOLOGICA 2021;113:70-84; DOI: 10.32074/1591-951X-213 Review The 2020 WHO Classification of Soft Tissue Tumours: news and perspectives Marta Sbaraglia1, Elena Bellan1, Angelo P. Dei Tos1,2 1 Department of Pathology, Azienda Ospedale Università Padova, Padova, Italy; 2 Department of Medicine, University of Padua School of Medicine, Padua, Italy Summary Mesenchymal tumours represent one of the most challenging field of diagnostic pathol- ogy and refinement of classification schemes plays a key role in improving the quality of pathologic diagnosis and, as a consequence, of therapeutic options. The recent publica- tion of the new WHO classification of Soft Tissue Tumours and Bone represents a major step toward improved standardization of diagnosis. Importantly, the 2020 WHO classi- fication has been opened to expert clinicians that have further contributed to underline the key value of pathologic diagnosis as a rationale for proper treatment. Several rel- evant advances have been introduced. In the attempt to improve the prediction of clinical behaviour of solitary fibrous tumour, a risk assessment scheme has been implemented. NTRK-rearranged soft tissue tumours are now listed as an “emerging entity” also in con- sideration of the recent therapeutic developments in terms of NTRK inhibition. This deci- sion has been source of a passionate debate regarding the definition of “tumour entity” as well as the consequences of a “pathology agnostic” approach to precision oncology. In consideration of their distinct clinicopathologic features, undifferentiated round cell sarcomas are now kept separate from Ewing sarcoma and subclassified, according to the underlying gene rearrangements, into three main subgroups (CIC, BCLR and not Received: October 14, 2020 ETS fused sarcomas) Importantly, In order to avoid potential confusion, tumour entities Accepted: October 19, 2020 such as gastrointestinal stroma tumours are addressed homogenously across the dif- Published online: November 3, 2020 ferent WHO fascicles. -

Expert-Level Diagnosis of Nonpigmented Skin Cancer by Combined Convolutional Neural Networks
Supplementary Online Content Tschandl P, Rosendahl C, Akay BN, et al. Expert-level diagnosis of nonpigmented skin cancer by combined convolutional neural networks. JAMA Dermatol. Published online November 28, 2018. doi:10.1001/jamadermatol.2018.4378 eFigure. Sensitivities (Blue) and Specificities (Orange) at Different Threshold Cutoffs (Green) of the Combined Classifier Evaluated on the Validation Set eAppendix. Neural Network Training eTable 1. Complete List of Diagnoses and Their Frequencies Within the Test-Set eTable 2. Education of Users According to Their Experience Group eTable 3. Percent of Correct Prediction of the Malignancy Status for Specific Diagnoses of a CNN Using Either Close-up or Dermatoscopic Images This supplementary material has been provided by the authors to give readers additional information about their work. © 2018 American Medical Association. All rights reserved. Downloaded From: https://jamanetwork.com/ on 09/25/2021 eFigure. Sensitivities (Blue) and Specificities (Orange) at Different Threshold Cutoffs (Green) of the Combined Classifier Evaluated on the Validation Set A threshold cut at 0.2 (black) is found for a minimum of 51.3% specificity. © 2018 American Medical Association. All rights reserved. Downloaded From: https://jamanetwork.com/ on 09/25/2021 eAppendix. Neural Network Training We compared multiple architecture and training hyperparameter combinations in a grid-search fashion, and used only the single best performing network for dermoscopic and close-up images, based on validation accuracy, for further analyses. We trained four different CNN architectures (InceptionResNetV2, InceptionV3, Xception, ResNet50) and used model definitions and ImageNet pretrained weights as available in the Tensorflow (version 1.3.0)/ Keras (version 2.0.8) frameworks. -
Shared Data & Cancer Registries
15 4 2021 Shared data & Cancer registries Jean-Yves BLAY Prof. of Medical oncology Director of Centre Léon Bérard Director of the ERN-EURACAN French Academy of Medicine President of Unicancer Disclosures Company Scientific advice Scientific works Symposia & oral communications Abbvie X X Amgen X X X ARIAD X X AstraZeneca X X Bayer X X X BMS X X X Deciphera x x DDB X X EISAI X X X Genomic Health X X Gilead X X GSK X X INNATE PHARMA X (member of the Supervisory committee) INCYTE X IQVIA x x x Jansenn X X LILLY X X Merck Serono X X MSD X X Nanobiotix X x Novartis X X X Novex X X Onxeo X Pfizer X X Pharmamar X X PRA X Roche X X Sanofi Aventis X X Swedish Orphan X X Takeda X Toray X Shared data & Cancer registries • The revolution of oncology : precision medicine vs biology based oncology (.. emerging rare cancers) • Shared data & registries: • Diagnosis • Epidemiology • Optimal primary treatment is cheaper • Connecting patients and doctors • Academic clinical and translational research Nosology and treatment Histology Nosology & treatment 2021+ Trials on molecular/immune Histology subgroups Molecular Trials on somatic genotype? Stroma characterization SHIVA, SAFIR, MOST (immune cells…) BASKET ! Example : NTRK fusions across cancers 0.5-1% of all cancers 9000/year in EU? Diagnosis? Treatment? EURACAN : THE ERN FOR RARE ADULT SOLID CANCERS Sub-thematic areas Connective tissue Female genital organs and placenta Male genital organs, and of the urinary tract Neuroendocrine system Digestive tract Endocrine organs 20% of cancers Head and neck 30% -

Diagnostic Value of CD163 in Cutaneous Spindle Cell Lesions
J Cutan Pathol 2009: 36: 859–864 Copyright # 2008 John Wiley & Sons A/S doi: 10.1111/j.1600-0560.2008.01179.x John Wiley & Sons. Printed in Singapore Journal of Cutaneous Pathology Continuing Medical Education Article Diagnostic value of CD163 in cutaneous spindle cell lesions Background: The histologic diagnosis of atypical fibroxanthoma Pedram Pouryazdanparast1, (AFX) can sometimes be challenging. No specific marker exists to Limin Yu1, Jonathan E. Cutlan1, confirm the diagnosis other than excluding other entities. CD163 has Stephen H. Olsen1,2, Douglas been shown to have great specificity for tumors of monocyte/histiocyte R. Fullen1,2 and Linglei Ma1,2 lineage. In this study, we evaluated the diagnostic utility of CD163 in 1Department of Pathology and diagnosing AFX and in identifying skin lesions with histiocytic/ 2Department of Dermatology, University of dendritic derivation. Michigan, Ann Arbor, MI, USA Methods: A total of 157 cases, including 14 AFXs, 5 spindle cell squamous cell carcinomas (SCCs), and 7 spindle cell/desmoplastic melanomas, along with other cutaneous spindle cell and histiocytic/ fibrohistiocytic lesions, were stained with CD163. Results: CD163 was expressed in 11 of 14 (79%) AFXs, with moderate to strong intensity. No staining was observed in cases of spindle cell SCC (0/5) and dermatofibrosarcoma protuberans (0/10). Rare spindle cell/desmoplastic melanomas (2/7) and cutaneous leiomyosarcomas (1/5) demonstrated positive staining. CD163 reactivity was seen in 24 of 29 of benign fibrous histiocytomas (BFHs), including 8 of 8 celular fibrous histiocytomas and 6 of 9 epithelioid cell histiocytomas. The majority of cutaneous histiocytic lesions, including juvenile xanthogranuloma, Langerhans cell histiocytosis and Rosai– Dorfman disease, were positive for CD163.