Shared Data & Cancer Registries
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Rare Skin Cancers in General Practice
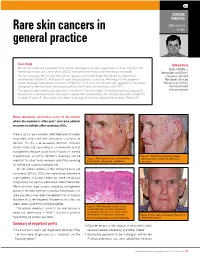
CLINICAL PRACTICE Skin cancer Rare skin cancers in series general practice Case study Anthony Dixon Mr LA has long been troubled with actinic damage to his skin, especially his face. He has had MBBS, FACRRM, is many squamous cell carcinomas (SCCs) removed and many solar keratoses managed. dermasurgeon and Director On this occasion Mr LA had two actinic lesions on his left cheek that failed to respond to of Research, Skin Alert cryotherapy (Figure 1). A biopsy of each site produced a surprise. Histology of the superior Skin Cancer Clinics and lesion revealed sebaceous carcinoma (Figure 2). This is an uncommon yet aggressive cutaneous Skincanceronly, Belmont, malignancy derived from sebaceous glands. The 5 year survival rate is 60–70%. Victoria. anthony@ The tumour was widely excised with a minimum 10 mm margin. A multidisciplinary approach skincanceronly.com resulted in a decision not to proceed to adjunctive radiotherapy. The wound was well healed by 8 weeks (Figure 3). Four years on there is no sign of local or regional recurrence (Figure 4). Many sebaceous carcinomas occur on the eyelids where the outcome is often poor;1 and some patients are prone to multiple other cutaneous SCCs. There is also a rare syndrome called Muir-torre of visceral neoplasms associated with sebaceous carcinoma on the skin.2 As this is an autosomal dominant condition, family history and counselling is an esssential part of management (enquire about family history of internal malignancies). A family member's diagnosis can be Figure 3. Satisfactory healing 8 weeks Figure 1. Two actinic lesions on the left face following wide excision of sebaceous important for other family members and offers screening have failed to respond to cryotherapy carcinoma for internal and cutaneous malignancies. -

A Rare Bone Tumor
OPEN ACCESS L E T T E R T O T H E E D I T O R Periosteal Desmoplastic Fibroma of Radius: A Rare Bone Tumor Aniqua Saleem1,* Hira Saleem2 1 Radiology Department, District Head Quarters Hospital, Rawalpindi Medical University, Rawalpindi 2 Department of Surgery, Shifa International Hospital, Islamabad. Correspondence*: Dr. Aniqua Saleem, Radiology Department, District Head Quarters Hospital, Rawalpindi Medical University, Rawalpindi E-mail: [email protected] © 2019, Saleem et al, Submitted: 05-04-2019 Accepted: 09-06-2019 Conflict of Interest: None Source of Support: Nil This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. DEAR SIR Desmoplastic fibroma is an extremely rare tumor of enhancement on post contrast images and with adjacent bone with a reported incidence of 0.11 % of all primary bone involvement as was evident by focal cortical inter- bone tumors. The most common site of involvement is ruption, mild endosteal thickening and irregularity and mandible (reported incidence 22% of all Desmoplastic also mild ulnar shaft remodeling (Fig. 3a, 3b). To further fibroma cases) followed by metaphysis of long bones. characterize the lesion, Tc99 MDP (methylene diphos- Involvement of forearm especially involving periosteum phonate) bone scan was also performed which showed is seldom reported. Prompt diagnosis and adequate active bone involvement in left distal radial shaft. management is important for limb salvage and restora- tion of limb function. [1-3] An 11-year-old boy presented with painful mild swelling of left forearm for a month, with no significant past med- ical history or any history of trauma. -

Atypical Compound Nevus Arising in Mature Cystic Ovarian Teratoma
J Cutan Pathol 2005: 32: 71–123 Copyright # Blackwell Munksgaard 2005 Blackwell Munksgaard. Printed in Denmark Journal of Cutaneous Pathology Abstracts of the Papers Presented at the 41st Annual Meeting of The American Society of Dermatopathology Westin Copley Place Boston, Massachusetts, USA October 14–17, 2004 These abstracts were presented in oral or poster format at the 41st Annual Meeting of The American Society of Dermatopathology on October 14–17, 2004. They are listed on the following pages in alphabetical order by the first author’s last name. 71 Abstracts IN SITU HYBRIDIZATION IS A VALUABLE DIAGNOSTIC A 37-year-old woman with diagnosis of Sjogren’s syndrome (SS) TOOL IN CUTANEOUS DEEP FUNGAL INFECTIONS presented with asymptomatic non-palpable purpura of the lower J.J. Abbott1, K.L. Hamacher2,A.G.Bridges2 and I. Ahmed1,2 extremities. Biopsy of a purpuric macule revealed a perivascular Departments of Laboratory Medicine and Pathology1 and and focally nodular lymphocytic infiltrate with large numbers of Dermatology2, plasma cells, seemingly around eccrine glands. There was no vascu- litis. The histologic findings in the skin were strikingly similar to those Mayo Clinic and Mayo Foundation, Rochester, MN, USA of salivary, parotid, and other ‘‘secretory’’ glands affected in SS. The cutaneous manifestations of SS highlighted in textbooks include Dimorphic fungal infections (histoplasmosis, blastomycosis, coccidiomy- xerosis, annular erythema, small-vessel vasculitis, and pigmented cosis, and cryptococcosis) can occur in immunocompromised and purpura. This case illustrates that purpura in skin of patients with healthy individuals. Cutaneous involvement is often secondary and SS may be caused by a peri-eccrine plasma-rich infiltrate. -

Atypical Fibroxanthoma - Histological Diagnosis, Immunohistochemical Markers and Concepts of Therapy
ANTICANCER RESEARCH 35: 5717-5736 (2015) Review Atypical Fibroxanthoma - Histological Diagnosis, Immunohistochemical Markers and Concepts of Therapy MICHAEL KOCH1, ANNE J. FREUNDL2, ABBAS AGAIMY3, FRANKLIN KIESEWETTER2, JULIAN KÜNZEL4, IWONA CICHA1* and CHRISTOPH ALEXIOU1* 1Department of Otorhinolaryngology, Head and Neck Surgery, University Hospital Erlangen, Erlangen, Germany; 2Dermatology Clinic, 3Institute of Pathology, and 4ENT Department, University Hospital Mainz, Mainz, Germany Abstract. Background: Atypical fibroxanthoma (AFX) is an in 1962 (2). The name 'atypical fibroxanthoma' reflects the uncommon, rapidly growing cutaneous neoplasm of uncertain tumor composition, containing mainly xanthomatous-looking histogenesis. Thus far, there are no guidelines for diagnosis and cells and a varying proportion of fibrocytoid cells with therapy of this tumor. Patients and Methods: We included 18 variable, but usually marked cellular atypia (3). patients with 21 AFX, and 2,912 patients with a total of 2,939 According to previous reports, AFX chiefly occurs in the AFX cited in the literature between 1962 and 2014. Results: In sun-exposed head-and-neck area, especially in elderly males our cohort, excision with safety margin was performed in 100% (3). There are two disease peaks described: one within the 5th of primary tumors. Local recurrences were observed in 25% of to 7th decade of life and another one between the 7th and 8th primary tumors and parotid metastases in 5%. Ten-year disease- decade. The former disease peak is associated with lower specific survival was 100%. The literature research yielded 280 tumor frequency (21.8%) and tumors that do not necessarily relevant publications. Over 90% of the reported cases were manifest on skin areas exposed to sunlight (4). -

Atypical Fibroxanthoma and Pleomorphic Dermal Sarcoma - Two Stages of the Same Disease?
Case Report World Journal of Oral and Maxillofacial Surgery Published: 12 Jul, 2018 Atypical Fibroxanthoma and Pleomorphic Dermal Sarcoma - Two Stages of the Same Disease? Farhana Kapasi1*, Marta Cabral2, Phillip Ameerally1 and Antonia Barbieri1 1Department of Oral and Maxillofacial Surgery, Northampton General Hospital, UK 2Marta Cabral, The Royal Devon and Exeter NHS Foundation Trust, UK Abstract Atypical Fibroxanthoma and Pleomorphic Dermal Sarcoma are rare cutaneous neoplasm's which share clinical and Histopathological features which can pose a diagnostic challenge. Atypical Fibroxanthoma has been considered a low-grade malignancy whereas Pleomorphic Dermal Sarcoma has been considered high grade and aggressive. We report a case of an 83-year-old male with a history of Actinic Keratosis who presented with an erythematous papule on the right parietal scalp. Histopathological diagnosis was Atypical Fibroxanthoma. Seven months postoperatively, the patient developed a rapidly growing purple nodule at the operative site which was adherent to the skull. Histopathological diagnosis was Pleomorphic Dermal Sarcoma with bone involvement. We suggest that the recurrence rate and low aggressive potential of Atypical Fibroxanthoma may have been underestimated, as these tumours are rare and have not been widely reported in the literature. In this case, the tumour recurred following complete excision. The recurrence was the more infiltrative Pleomorphic Dermal Sarcoma, which reinforces the hypotheses that Atypical Fibroxanthoma may be the precursor lesion of Pleomorphic Dermal Sarcoma and that these are indeed two stages of the same disease rather than separate entities. Keywords: General dermatology; Medical dermatology; Head and neck oncology Introduction OPEN ACCESS Atypical Fibroxanthoma is a rare cutaneous tumour first described in 1963 by Elson Helwig [1]. -

Cutaneous Neoplasms
torr CALIFORNIA TUMOR TISSUE REGISTRY 1 03RD SEMI-ANNUAL CANCER SEMINAR ON CUTANEOUS NEOPLASMS CASE HISTORIES 00•MODERAT.0RS: . PHILIP E. LE~0FJ', M.Q. Dir;ector O:f Oermatopafholo.gy ;Ser:Vice Associate Professor of Clinical Pathology U.C.S.F.- Elermatopa~hology San Francisco, ·californla and TIMGTH1f' H. MCG~WMON'f,, M ~D. Assistant Clinical Professor U.C~S.F. - Dermatopathology San Francisco, California December 7, 1997 Sheraton Palace Hotel San Francisco, California PLATFORM CHAIR: CLAUDE 0. BURDICK, M.D. Director of laboratory ValleyCare Health System Pleasanton, California CASE RISTORJES 10.3"" Semi-Annual Seminar (Due to in$uffient material, Case 115 is • compo~ite to two ca!ICll with an identical diagnosis, Ace. #15523 and Ace #12395.) Ca.c 1#1 - As:c 1#28070: The patient was a 12-ycaro{)ld male who had a fairly long history ofa very small bump in the scalp of the temporal area, which had recently become greally enlarged. The submitting denna!ologist mentioned that this was a soliwy lesion, with no other lesions apparent (Contributed by Prescott Rasmussen, MD.) c-111- As:c #11543: The patient was a 60-year-old Caucasian female wbo presented with a S.O em right suprapalellar subcutaneous mass which was reported to be present and gradually increasing in size for a period of approximately rn·o years. There was no history of prior trauma, and the remainder ofthe clinical history and physical findings wcze uoremarialble. An cxeisional biopsy was performed. The specimeD consisted ofa 4.S x 1.1 em elliptical segment ofeentnllly dimpled skin which surmowlted a S.3 x 4.4 x 3.6 em delicately encapsulated. -

Myxofibrosarcoma Mimicking Inflammatory Lesion Of
applied sciences Communication Myxofibrosarcoma Mimicking Inflammatory Lesion of Temporomandibular Joint—Case Presentation Dawid Zagacki 1,*, Krzysztof Sztychny 2, Marta Tyndorf 2, Robert Bibik 3, Dominik Sygut 4 and Marcin Kozakiewicz 2 1 International Doctoral School, Medical University of Łód´z,Pl. Hallera 1, 90-647 Łód´z,Poland 2 Department of Maxillofacial Surgery, Medical University of Łód´z,Pl. Hallera 1, 90-647 Łód´z,Poland; [email protected] (K.S.); [email protected] (M.T.); [email protected] (M.K.) 3 Department of Radiation Oncology, Radom’s Oncology Centre, 26-600 Radom, Poland; [email protected] 4 Department of Clinical Patomorphology and Cytopathology, Medical University of Lodz, ul. Zeromskiego 113, 90-549 Lodz, Poland; [email protected] * Correspondence: [email protected] Abstract: Treating oncologic patients remains a challenge for surgeons aiming to provide patients with safe margins of resection while maintaining the highest possible quality of life. The latter, in the case of malignancies, requires using sophisticated methods of reconstruction. Thus, we present a case of a 75-year-old patient treated in our department with a rare neoplasm in the region of the temporomandibular joint—a myxofibrosarcoma that was mimicking an inflammatory lesion. The patient underwent two surgeries—firstly alloplasty of the TMJ due to the suspicion of an inflammatory lesion, lately extended to the resection of glenoid fossa and subtemporal fossa contents when the mandible was reconstructed using UHMW-PE (ultra-high molecular weight polyethylene). Citation: Zagacki, D.; Sztychny, K.; The patient was also referred for adjuvant radiotherapy and has remained disease-free for over Tyndorf, M.; Bibik, R.; Sygut, D.; 96 months with very good aesthetics and function of the mandible. -

Desmoplastic Fibroma
Send Orders of Reprints at [email protected] 40 The Open Orthopaedics Journal, 2013, 7, 40-46 Open Access Desmoplastic Fibroma: A Case Report with Three Years of Clinical and Radiographic Observation and Review of the Literature Alexander Nedopil*, Peter Raab and Maximilian Rudert Department of Orthopaedic Surgery at the University of Würzburg, König Ludwig Haus, Germany Abstract: Background: Desmoplastic fibroma (DF) is an extremely rare locally aggressive bone tumor with an incidence of 0.11% of all primary bone tumors. The typical clinical presentation is pain and swelling above the affected area. The most common sites of involvement are the mandible and the metaphysis of long bones. Histologically and biologically, desmoplastic fibroma mimics extra-abdominal desmoid tumor of soft tissue. Case Presentation and Literature Review: A case of a 27-year old man with DF in the ilium, including the clinical, radiological and histological findings over a 4-year period is presented here. CT scans performed in 3-year intervals prior to surgical intervention were compared with respect to tumor extension and cortical breakthrough. The patient was treated with curettage and grafting based on anatomical considerations. Follow-up CT scans over 18-months are also documented here. Additionally, a review and analysis of 271 cases including the presented case with particular emphasis on imaging patterns in MRI and CT as well as treatment modalities and outcomes are presented. Conclusion: In patients with desmoplastic fibroma, CT is the preferred imaging technique for both the diagnosis of intraosseus tumor extension and assessment of cortical involvement, whereas MRI is favored for the assessment of extraosseus tumor growth and preoperative planning. -

The New EU Agenda on Cancer and the Role of the European Reference Network EURACAN Jean Yves Blay
14 1 2021 The new EU Agenda on Cancer and the role of the European Reference Network EURACAN J-Y Blay Rare Adult Solid Cancers Co-funded by the EU Connective tissue Female genital organs and placenta Male genital organs, and of the urinary tract Neuroendocrine system Digestive tract Endocrine organs Head and neck Thorax Skin and eye melanoma Brain, spinal cords Geographical spreading of the Consortium all over Europe. 2017 66 full members accross 17 Member states Cyprus 2020 9 APS accross 7 Member States 2021 42 new members EURACAN - Lyon_Centre Léon Bérard November 2020 ASSOCIATE PARTNERS EURACAN - Lyon_Centre Léon Bérard November 2020 AFFILIATED PARTNERS Associated National Centres approved National Coordination hub approved Austria • Centre for bone and soft tissue tumors – Graz Luxembourg -Hospital Centre Croatia Malta - Mater dei Hospital - • University Hospital centre - Zagreb • Sestre University Hospital centre - Zagreb Cyprus • Bank of Cyprus oncology centre in collaboration with the Karaiskakio Foundation Estonia • North Estonia Medical Centre • University Hospital - Taru Latvia • East clinical University Hospital - Riga Member state Town Candidate Name DOMAIN(S) APPROVED BY THE BoN code G1.1 G2.2 G5.2 G9.1 G10 Brussels Cliniques universitaires Saint-Luc ASBL BE G1 G2.2 G3.1 G6.1 G9.2 Ghent Ghent University Hospital Prague Thomayer Hospital G3.1 CZ G2.1 Prague The institute for the Care of Mother and Child Berlin Helios Klinikum Berlin-Buch G1.1 G1.2 DE G1.1 G1.2 G2.1 G2.2 G3.1 G4 G5.1 G5.2 Munich Comprehensive Cancer Center -

Low‑Grade Myofibroblastic Sarcoma Arising in the Tip of the Tongue with Intravascular Invasion: a Case Report
ONCOLOGY LETTERS 16: 3889-3894, 2018 Low‑grade myofibroblastic sarcoma arising in the tip of the tongue with intravascular invasion: A case report YURIE MIKAMI1,2, SHINSUKE FUJII1, KEN‑ICHI KOHASHI3, YUICHI YAMADA3, MASAFUMI MORIYAMA2, SHINTARO KAWANO2, SEIJI NAKAMURA2, YOSHINAO ODA3 and TAMOTSU KIYOSHIMA1 1Laboratory of Oral Pathology and 2Section of Maxillofacial Oncology, Division of Maxillofacial Diagnostic and Surgical Sciences, Faculty of Dental Science, Kyushu University; 3Department of Anatomic Pathology, Graduate School of Medical Sciences, Kyushu University, Higashi‑ku, Fukuoka 812‑8582, Japan Received March 24, 2018; Accepted June 28, 2018 DOI: 10.3892/ol.2018.9115 Abstract. Low‑grade myofibroblastic sarcoma (LGMS) is a firstly identified in granulation tissue in 1971 (5). Fibroblasts rare intermediate tumor, which rarely metastasizes and has differentiate into myofibroblasts during wound healing myofibroblastic differentiation in various sites. It is particularly and tissue repair (6). According to the 2013 World Health associated with the tongue in the head and neck region. The Organization (WHO) classification (7), LGMS is categorized lack of any pathological features means it is difficult to make as a fibroblastic/myofibroblastic tumor; intermediate tumors a conclusive diagnosis of LGMS. The immunohistochemical (rarely metastasizing). Clinically, LGMS has a propensity for features and genomic rearrangements, including SS18‑SSXs local recurrence and is associated with a low risk of metastatic and MYH9‑USP6s and the genetic mutations of cancer‑associ- spread. Immunohistochemically, LGMS tumor cells are posi- ated genes, including APC, CTNNB1, EGFR, KRAS, PIK3CA tive for at least one myogenic marker, such as alpha‑smooth and p53 were examined in a case of LGMS arising in the tip muscle actin (α‑SMA), desmin or muscle actin (HHF‑35). -

Pathology and Genetics of Tumours of Soft Tissue and Bone
bb5_1.qxd 13.9.2006 14:05 Page 3 World Health Organization Classification of Tumours WHO OMS International Agency for Research on Cancer (IARC) Pathology and Genetics of Tumours of Soft Tissue and Bone Edited by Christopher D.M. Fletcher K. Krishnan Unni Fredrik Mertens IARCPress Lyon, 2002 bb5_1.qxd 13.9.2006 14:05 Page 4 World Health Organization Classification of Tumours Series Editors Paul Kleihues, M.D. Leslie H. Sobin, M.D. Pathology and Genetics of Tumours of Soft Tissue and Bone Editors Christopher D.M. Fletcher, M.D. K. Krishnan Unni, M.D. Fredrik Mertens, M.D. Coordinating Editor Wojciech Biernat, M.D. Layout Lauren A. Hunter Illustrations Lauren A. Hunter Georges Mollon Printed by LIPS 69009 Lyon, France Publisher IARCPress International Agency for Research on Cancer (IARC) 69008 Lyon, France bb5_1.qxd 13.9.2006 14:05 Page 5 This volume was produced in collaboration with the International Academy of Pathology (IAP) The WHO Classification of Tumours of Soft Tissue and Bone presented in this book reflects the views of a Working Group that convened for an Editorial and Consensus Conference in Lyon, France, April 24-28, 2002. Members of the Working Group are indicated in the List of Contributors on page 369. bb5_1.qxd 22.9.2006 9:03 Page 6 Published by IARC Press, International Agency for Research on Cancer, 150 cours Albert Thomas, F-69008 Lyon, France © International Agency for Research on Cancer, 2002, reprinted 2006 Publications of the World Health Organization enjoy copyright protection in accordance with the provisions of Protocol 2 of the Universal Copyright Convention. -

Nationwide Incidence of Sarcomas and Connective Tissue Tumors of Intermediate Malignancy Over Four Years Using an Expert Pathology Review Network
medRxiv preprint doi: https://doi.org/10.1101/2020.06.19.20135467; this version posted June 22, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. All rights reserved. No reuse allowed without permission. Nationwide incidence of sarcomas and connective tissue tumors of intermediate malignancy over four years using an expert pathology review network. Prof. Gonzague de Pinieux MD, PhD *1 , Marie Karanian-Philippe MD *2, Francois Le Loarer MD, PhD*3, Sophie Le Guellec MD4 , Sylvie Chabaud PhD2, Philippe Terrier MD 5, Corinne Bouvier MD,PhD6, Maxime Battistella MD,PhD 7, Agnès Neuville MD, PhD3 , Yves-Marie Robin MD 8, Jean- Francois Emile MD, PhD 9 , Anne Moreau MD 10, Frederique Larousserie MD, PhD 11, Agnes Leroux MD12 , Nathalie Stock MD 13, Marick Lae MD 14, Francoise Collin MD15, Nicolas Weinbreck MD16, Sebastien Aubert MD8, Florence Mishellany MD17, Céline Charon-Barra MD15, Sabrina Croce MD, PhD3, Laurent Doucet MD 18, Isabelle Quintin-Rouet MD18 , Marie-Christine Chateau MD19 , Celine Bazille MD20, Isabelle Valo MD21, Bruno Chetaille MD16, Nicolas Ortonne MD22, Anne Gomez-Brouchet MD, PhD4 , Philippe Rochaix MD4, Anne De Muret MD1, Jean-Pierre Ghnassia MD, PhD23 , Lenaig Mescam-Mancini MD 25, Nicolas Macagno MD6, Isabelle Birtwisle-Peyrottes MD26, Christophe Delfour MD19, Emilie Angot MD13, Isabelle Pommepuy MD2, Dominique Ranchere-Vince MD2, Claire Chemin- Airiau MSc2 , Myriam Jean-Denis MSc2, Yohan Fayet PhD2 , Jean-Baptiste Courrèges MSc3 , Nouria Mesli MSc3 , Juliane Berchoud MSc10 , Maud Toulmonde MD, PhD3, Prof.