Fourth Fistula Campaign in Somalia
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Bay Bakool Rural Baseline Analysis Report
Technical Series Report No VI. !" May 20, 2009 Livelihood Baseline Analysis Bay and Bakool Food Security and Nutrition Analysis Unit - Somalia Box 1230, Village Market Nairobi, Kenya Tel: 254-20-4000000 Fax: 254-20-4000555 Website: www.fsnau.org Email: [email protected] Technical and Funding Agencies Managerial Support European Commission FSNAU Technical Series Report No VI. 19 ii Issued May 20, 2009 Acknowledgements These assessments would not have been possible without funding from the European Commission (EC) and the US Office of Foreign Disaster and Assistance (OFDA). FSNAU would like to also thank FEWS NET for their funding contributions and technical support made by Mohamed Yusuf Aw-Dahir, the FEWS NET Representative to Soma- lia, and Sidow Ibrahim Addow, FEWS NET Market and Trade Advisor. Special thanks are to WFP Wajid Office who provided office facilities and venue for planning and analysis workshops prior to, and after fieldwork. FSNAU would also like to extend special thanks to the local authorities and community leaders at both district and village levels who made these studies possible. Special thanks also to Wajid District Commission who was giving support for this assessment. The fieldwork and analysis would not have been possible without the leading baseline expertise and work of the two FSNAU Senior Livelihood Analysts and the FSNAU Livelihoods Baseline Team consisting of 9 analysts, who collected and analyzed the field data and who continue to work and deliver high quality outputs under very difficult conditions in Somalia. This team was led by FSNAU Lead Livelihood Baseline Livelihood Analyst, Abdi Hussein Roble, and Assistant Lead Livelihoods Baseline Analyst, Abdulaziz Moalin Aden, and the team of FSNAU Field Analysts and Consultants included, Ahmed Mohamed Mohamoud, Abdirahaman Mohamed Yusuf, Abdikarim Mohamud Aden, Nur Moalim Ahmed, Yusuf Warsame Mire, Abdulkadir Mohamed Ahmed, Abdulkadir Mo- hamed Egal and Addo Aden Magan. -

Somalia Terror Threat
THECHRISTOPHER TERROR February 12, THREAT FROM THE TERROR THREAT FROM SOMALIA THE INTERNATIONALIZATION OF AL SHABAAB CHRISTOPHER HARNISCH APPENDICES AND MAPS BY KATHERINE ZIMMERMAN FEBRUARY 12, 2010 A REPORT BY THE CRITICAL THREATS PROJECT OF THE AMERICAN ENTERPRISE INSTITUTE THE TERROR THREAT FROM SOMALIA CHRISTOPHER HARNISCH February 12, 2010 Contents EXECUTIVE SUMMARY 1 IMPORTANT GROUPS AND ORGANIZATIONS IN SOMALIA 3 NOTABLE INDIVIDUALS 4 INTRODUCTION 8 ORIGINS OF AL SHABAAB 10 GAINING CONTROL, GOVERNING, AND MAINTAINING CONTROL 14 AL SHABAAB’S RELATIONSHIP WITH AL QAEDA, THE GLOBAL JIHAD MOVEMENT, AND ITS GLOBAL IDEOLOGY 19 INTERNATIONAL RECRUITING AND ITS IMPACT 29 AL SHABAAB’S INTERNATIONAL THREATS 33 THREAT ASSESSMENT AND CONCLUSION 35 APPENDIX A: TIMELINE OF MAJOR SECURITY EVENTS IN SOMALIA 37 APPENDIX B: MAJOR SUICIDE ATTACKS AND ASSASSINATIONS CLAIMED BY OR ATTRIBUTED TO AL SHABAAB 47 NOTES 51 Maps MAP OF THE HORN OF AFRICA AND MIDDLE EAST 5 POLITICAL MAP OF SOMALIA 6 MAP OF ISLAMIST-CONTROLLED AND INFLUENCED AREAS IN SOMALIA 7 www.criticalthreats.org THE TERROR THREAT FROM SOMALIA CHRISTOPHER HARNISCH February 12, 2010 Executive Summary hree hundred people nearly died in the skies of and assassinations. Al Shabaab’s primary objectives at TMichigan on Christmas Day, 2009 when a Niger- the time of the Ethiopian invasion appeared to be ian terrorist attempted to blow up a plane destined geographically limited to Somalia, and perhaps the for Detroit. The terrorist was an operative of an al Horn of Africa. The group’s rhetoric and behavior, Qaeda franchise based in Yemen called al Qaeda in however, have shifted over the past two years reflect- the Arabian Peninsula (AQAP). -

World Bank Final Report
The Common Social Accountability Platform Deploying the Common Social Accountability Platform to inform the 2020 World Bank Performance and Learning Review January 2020 Africa’s Voices Project Team: Africa’s Voices Project Team: Anna Tomson (Governance & Accountability Senior Programme Manager), Khadija Mohamed (Programme Officer), Nasri Ali (Programme Officer), Zakaria Sheikh (Research Assistant), Alexander Simpson (Software Engineer), Lucas Malla (Senior Quantitative Researcher), and Samuel Kimeu (Executive Director). © 2019 Africa’s Voices Foundation Ltd Africa’s Voices Foundation Africa’s Voices Foundation Kenya Riverside Suites, Riverside Lane, Nairobi UK Centre for Global Equality, 8C King’s Parade CB2 1SP Cambridge africasvoices.org @africas_voices This report was written by Anna Tomson, Senior Programme Manager, Governance & Accountability and Khadija Hussein at Africa’s Voices Foundation 2 Africa’s Voices Foundation List of acronyms 4 1. INTRODUCTION 5 1.1 Context 5 1.2 Project Objectives 5 1.3 The Common Social Accountability Platform 6 1.4 AVF’s Interactive Radio Method 6 2. Methodology 8 2.1 Building inclusive community engagement at scale 8 2.2 Gathering insight on public opinion 10 2.3 Limitations of the methodology 10 3. Engagement 11 3.1 Content of the radio dialogue 11 3.2 Who participated in the dialogue 11 4. Insights into citizen perspectives 14 4.1 Citizen priorities for development 14 4.2 Citizen access to decision making and grievance mechanisms 21 ANNEX 1: List of radio stations 26 ANNEX 2: Thick description 27 ANNEX -

Constraints and Complexities of Information and Analysis in Humanitarian Emergencies Evidence from Somalia
November 2018 Constraints and Complexities of Information and Analysis in Humanitarian Emergencies Evidence from Somalia A FEINSTEIN INTERNATIONAL CENTER PUBLICATION Peter Hailey, Jeeyon Janet Kim, Erin McCloskey, Maria Wrabel, Daniel Maxwell FRIEDMAN SCHOOL OF NUTRITION SCIENCE AND POLICY Feinstein International Center Somalia Case Study Report 1 Cover photo: Pastoralists at well in Wajid District, Somalia, 2008. By Dan Maxwell. Citation: Hailey, Peter, Jeeyon Janet Kim, Erin McClos- key, Maria Wrabel, and Daniel Maxwell. Constraints and Complexities of Information and Analysis in Humanitarian Emergencies: Evidence from Somalia. Boston: Feinstein International Center, Tufts University, 2018. Corresponding author: Daniel Maxwell Corresponding author email: [email protected] This study—Constraints and Complexities of Informa- tion and Analysis in Humanitarian Emergencies—was funded by the Swiss Agency for Development Coop- eration (SDC) through a grant to the Feinstein Inter- national Center at the Friedman School of Nutrition Science and Policy, Tufts University. The research was conducted jointly by staff of the Feinstein Center and the Centre for Humanitarian Change in Nairobi. Jeeyon Janet Kim, Maria Wrabel, and Daniel Maxwell are with the Feinstein International Center, Friedman School of Nutrition Science and Policy, Tufts University, Boston. Peter Hailey and Erin McCloskey are with the Centre for Humanitarian Change, Nairobi. Copyright 2018 Tufts University, all rights reserved. “Tufts University” is a registered trademark -
Somalia Complex Emergency Fact Sheet #1- 04-26-2013
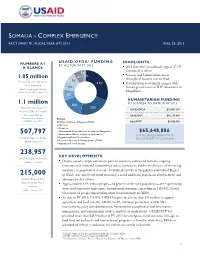
SOMALIA - COMPLEX EMERGENCY FACT SHEET #1, FISCAL YEAR (FY) 2013 APRIL 26, 2013 USAID/OFDA 1 F U N D I N G NUMBERS AT HIGHLIGHTS BY SECTOR IN FY 2013 A GLANCE 2013 Somalia Consolidated Appeal (CAP) requests $1.3 billion 2% Security and humanitarian access 6% 1% 1.05 million throughout Somalia remain fluid 7% People Experiencing Acute 31% Humanitarian community engages with Food Insecurity 7% Somali government on IDP relocations in U.N. Food Security and Nutrition Analysis Unit (FSNAU) – April 2013 Mogadishu 8% HUMANITARIAN FUNDING 1.1 million TO SOMALIA TO DATE IN FY 2013 15% Total Internally Displaced 23% USAID/OFDA $15,069,387 Persons (IDPs) in Somalia Office of the U.N. High USAID/FFP2 $45,579,499 Commissioner for Refugees Health 3 (UNHCR) – April 2013 Water, Sanitation, & Hygiene (WASH) State/PRM $5,000,000 Nutrition Protection Humanitarian Coordination & Information Management $65,648,886 507,797 Humanitarian Studies, Analysis, or Applications TOTAL USAID AND STATE Somali Refugees in Kenya Logistics and Relief Commodities ASSISTANCE TO SOMALIA Economic Recovery & Market Systems (ERMS) UNHCR – April 2013 Agriculture & Food Security 238,957 KEY DEVELOPMENTS Somali Refugees in Ethiopia UNHCR – April 2013 Despite security improvements in parts of southern and central Somalia, ongoing insecurity and restricted humanitarian access continue to hinder the delivery of life-saving assistance to populations in need. Al-Shabaab activity in Mogadishu and Bakool Region 215,000 in March and April heightened insecurity, caused additional population displacement, and Acutely Malnourished obstructed relief efforts. Children under Five in Approximately 1.05 million people—14 percent of the total population—are experiencing Somalia FSNAU – February 2013 acute food insecurity and require humanitarian assistance, according to FSNAU. -

Nutrition Analysis Post Gu ‘12
Nutrition Analysis Post Gu ‘12 Technical Series Report No VI. 47 September 26, 2012 Food Security and Nutrition Analysis Unit - Somalia Information for Better Livelihood Technical Partners Funding Agencies FSNAU Technical Series Report No. VI 47 Swiss Agency for Development and Cooperation SDC Issued September 26, 2012 Post Deyr 2011/12 Nutrition Analysis ii FSNAU Technical Series Report No. VI 47 Issued September 26, 2012 Acknowledgements FSNAU would like to thank all our 24 partner agencies for their participation and support in the Deyr 2011 seasonal nutrition assessments and analysis. Post Deyr 2011/12 Acknowledgement Nutrition Analysis From April through July 2012, a total of 46 nutrition surveys were conducted based on standard SMART methodology. Seventeen of the nutrition surveys were conducted in the south. Additionally, nutrition iii data from about 130 health and nutrition facilities was reviewed. Without the support and expertise of the 8 local NGOs, 3 International NGOs, 3 Local Authorities, 8 line Ministries and 2 UN agencies, this would not have been possible. Special thanks to UNICEF, for financial and/or technical support. A sincere note of appreciation also goes to the FSNAU nutrition team based in Somalia who work under such difficult conditions yet continue to produce such high quality professional work. Participating Partners - North Central regions only United Nations Children’s Fund (UNICEF), World Food Programme (WFP), Ministry of Health (MOH Somaliland), Ministry of Agriculture (Somaliland), Ministry of environment and rural development, and NERAD (Somaliland); Ministry of Health (Puntland), Ministry of Women Development and Family Affairs (MoWDFA), Ministry of Wildlife, Tourism and Environment (Puntland), Puntland State of Water and Energy (PSWEN), Medair, Somalia Red Crescent Society (SRCS), CAFDARO and Elberde Primary Health Care organization (EPHCO). -
Shabelle Relief and Development Organization (SHARDO)
Shabelle Relief and Development Organization (SHARDO) ASSESSMENT REPORT ON THE MECHANISMS AND NEEDS OF THE POPULATION LIVING IN JOWHAR, ADALE AND ADAN YABAL, WARSHEIKH DISTRICITS OF MIDDLE SHABELLE REGION. 1. General principles: Name of the implementing Agency Shabelle Relief and Development Organization (SHARDO) Name of the Funding Agency Somali – Swedish Intellectual Banadir Organization (SIBO) Assessment Period: 1st – 10th December 2007 Reporting Period: 15th December 2007 Contact Person: Mohamed Ahmed Moallim Tell: +252 1 644449 Mobile: +252 1 5513089 Email: [email protected] 1 2. Contents 1. General Principles Page 1 2. Contents 2 3. Introduction 3 4. General Objective 3 5. Specific Objective 3 6. General and Social demographic, economical Mechanism in Middle Shabelle region 4 1.1 Farmers 5 1.2 Agro – Pastoralists 5 1.3 Adale District 7 1.4 Fishermen 2 3. Introduction: Middle Shabelle is located in the south central zone of Somalia The region borders: Galgadud to the north, Hiran to the West, Lower Shabelle and Banadir regions to the south and the Indian Ocean to the east. A pre – war census estimated the population at 1.4 million and today the regional council claims that the region’s population is 1.6 million. The major clans are predominant Hawie and shiidle. Among hawiye clans: Abgal, Galjecel, monirity include: Mobilen, Hawadle, Kabole and Hilibi. The regional consists of seven (7) districts: Jowhar – the regional capital, Bal’ad, Adale, A/yabal, War sheikh, Runirgon and Mahaday. The region supports livestock production, rain-fed and gravity irrigated agriculture and fisheries, with an annual rainfall between 150 and 500 millimeters covering an area of approximately 60,000 square kilometers, the region has a 400 km coastline on Indian Ocean. -

Somalia Emergency Weekly Health Update Aims to Provide an Overview of the Health Activities Conducted by WHO and Health Partners in Somalia
SSoommaalliiaa EEmmeerrggeennccyy WWeeeekkllyy HHeeaalltthh UUppddaattee The Somalia emergency weekly health update aims to provide an overview of the health activities conducted by WHO and health partners in Somalia. It compiles health information including nine health events (epidemiological surveillance) reported in Somalia, information on ongoing conflicts in some regions of Somalia and health responses from partners. For further information please contact: Pieter Desloovere - Communications Officer - [email protected] - T: +254 733 410 984 BULLETIN HIGHLIGHTS Reporting dates 1-14 April 2012 (reflecting Epidemiological week 13 and 14) • On 4 April, a female suicide bomber killed at least six people at National Theater in Mogadishu. According to three major hospitals in Mogadishu, the caseload accounted for 80 casualties, including eight death. • On 9 April, more than 40 casualties were brought to Baidoa hospital after a bomb exploded at the market place of Baidoa. • Child Health Days have kicked off, on 10 April in Gedo region as well as Banadir region. Two rounds will be organized in Banadir region, with round one from 14-18 April 2012 and round two from 21-25 April 2012. Proportion of timely reporting sentinel sites by zone % 100 90 80 70 67 facilitiess 65 60 59 63 61 R. 57 57 50 52 54 of 50 40 42 36 30 20 23 Proporton 10 0 1234567891011121314 Weeks South & Central Puntland Somaliland Of the 222 sentinel sites reporting weekly from the three zones of Somalia, for week 13, 98% (53) in Puntland, 98% (44) in Somaliland, but only 36% (44) sentinel sites reported on time from South and Central Somalia or 64% (141) of all sentinel sites. -

Protection Cluster Update Weekly Report
Protection Cluster Update Funded by: The People of Japan Weeklyhttp://www.shabelle.net/article.php?id=4297 Report 23 th September 2011 European Commission IASC Somalia •Objective Protection Monitoring Network (PMN) Humanitarian Aid This update provides information on the protection environment in Somalia, including apparent violations of Human Rights and International Humanitarian Law as reported during the last two weeks through the IASC Somalia Protection Cluster monitoring systems. Incidents mentioned in this report are not exhaustive. They are intended to highlight credible reports in order to inform and prompt programming and advocacy initiatives by the humanitarian community and national authorities. General Overview Heavy fighting in southern regions between Al Shabaab and Transitional Federal Government (TFG) has led to heightened protection concerns throughout the reporting period. In Ceel Waaq, 43 people were killed and almost 80 wounded and an unknown number displaced following fighting between the TFG and Al Shabaab forces.1 The civilian population continues to face insecurity due to the ongoing conflict compounded by limited access to basic services and humanitarian support. In other regions, the famine has continued to take its toll on the Somali population. This week the United Nations Children Fund (UNICEF) stated that Somalia has the worst international mortality rate for children. 2 Furthermore, local sources in the district of Eldher town, Galgaduud region reported that 30 people had died as a result of starvation and -
Somalia from Resilience Towards Recovery and Development
Report No.34356-SO Report No. 34356-SO Somalia From Resilience Towards Recovery and Development Public Disclosure Authorized Public Disclosure Authorized A Country Economic Memorandum for Somalia January 11, 2006 Poverty Reduction and Economic Management 2 Country Department for Somalia Africa Region Somalia and Development Recovery Towards Resilience From Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of the World Bank GFATM Global Fund to Fight Aids, Tuberculosis and Malaria ICAO International Civil Aviation Organization ICRC International Committee ofthe Red Cross IDA International Development Association IDP Internally Displaced People IFAD International Fund for Agriculture Development IFC International Finance Corporation IMF International Monetary Fund ITCZ Inter-Tropical Convergence Zone ITU International Telecommunication Union JNA Joint Needs Assessment KPHIS Kenya Plant Health Inspectorate Service KSA Kingdom of Saudi Arabia LDC Least Developed Country LICUS Low Income Countries under Stress MCH Maternal and Child Health MDG MillenniumDevelopment Goal MDRP Multi-Country Demobilization and Reintegration Program MDTF Multi-Donor Trust Fund MICS Multi Indicators Cluster Survey NGO NonGovernmental Organization ODA Official Development Assistance OECD Organization of Economic Cooperation and Development PHC Primary Health Care RRA Rahanweyn Residtance Army PRS Poverty Reduction Strategy SACB Somalia -

Somalia: Window of Opportunity for Addressing One of the World's Worst Internal Displacement Crises 9
SOMALIA: Window of opportunity for addressing one of the world’s worst internal displacement crises A profile of the internal displacement situation 10 January 2006 This Internal Displacement Profile is automatically generated from the online IDP database of the Internal Displacement Monitoring Centre (IDMC). It includes an overview of the internal displacement situation in the country prepared by the IDMC, followed by a compilation of excerpts from relevant reports by a variety of different sources. All headlines as well as the bullet point summaries at the beginning of each chapter were added by the IDMC to facilitate navigation through the Profile. Where dates in brackets are added to headlines, they indicate the publication date of the most recent source used in the respective chapter. The views expressed in the reports compiled in this Profile are not necessarily shared by the Internal Displacement Monitoring Centre. The Profile is also available online at www.internal-displacement.org. About the Internal Displacement Monitoring Centre The Internal Displacement Monitoring Centre, established in 1998 by the Norwegian Refugee Council, is the leading international body monitoring conflict-induced internal displacement worldwide. Through its work, the Centre contributes to improving national and international capacities to protect and assist the millions of people around the globe who have been displaced within their own country as a result of conflicts or human rights violations. At the request of the United Nations, the Geneva-based Centre runs an online database providing comprehensive information and analysis on internal displacement in some 50 countries. Based on its monitoring and data collection activities, the Centre advocates for durable solutions to the plight of the internally displaced in line with international standards. -
Transition Initiatives for Stabilization Plus (Tis+) Program Year Three – Annual Work Plan
TRANSITION INITIATIVES FOR STABILIZATION PLUS (TIS+) PROGRAM YEAR THREE – ANNUAL WORK PLAN (OCTOBER 1, 2017 – SEPTEMBER 30, 2018) Revised November 2017 This publication was produced for review by the United States Agency for International Development. It was prepared by AECOM. Annual Work plan | Transition Initiatives for Stabilization Plus (TIS+) Program i TRANSITION INITIATIVES FOR STABILIZATION PLUS (TIS+) PROGRAM YEAR THREE – ANNUAL WORK PLAN (OCTOBER 1, 2017 – SEPTEMBER 30, 2018) Contract No: AID-623-C-15-00001 Submitted to: USAID | Somalia Prepared by: AECOM International Development DISCLAIMER: The authors’ views expressed in this document do not necessarily reflect the views of the United States Agency for International Development or the United States Government. Year Three - Annual Work Plan | Transition Initiatives for Stabilization Plus (TIS+) Program i TABLE OF CONTENTS Table of Contents ........................................................................................................................................ ii Acronym List .............................................................................................................................................. iii Stabilization Context .................................................................................................................................. 5 Goals and Objectives of USAID and TIS+ ............................................................................................... 6 Methodology ........................................................................................................................................