Rehabilitation 2030: a Call for Action
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Pure Magazine
PURE MAGAZINOctobeEr 2017 Jack O’Rourke Talks Music, Electric Picnic, Father John Misty and more… The Evolution Of A Modern Gentleman Jimmy Star chats with Hollywood actor... Sean Kanan Sony’s VR capabilities establishes them as serious contenders in the Virtual Reality headset war! Eli Lieb Talks Music, Creating & Happiness… Featured Artist Dionne Warwick Marilyn Manson Cheap Trick Otherkin Eileen Shapiro chats with award winning artist Emma Langford about her Debut + much more EalbumM, tour neMws plus mAore - T urLn to pAage 16 >N> GFORD @PureMzine Pure M Magazine ISSUE 22 Mesmerising WWW.PUREMZINE.COM forty seven Editor in Chief Trevor Padraig [email protected] and a half Editorial Paddy Dunne [email protected] minutes... Sarah Swinburne [email protected] Shane O’ Rielly [email protected] Marilyn Manson Heaven Upside Down Contributors Dave Simpson Eileen Shapiro Jimmy Star Garrett Browne lt-rock icon Marilyn Manson is back “Say10” showcases a captivatingly creepy Danielle Holian brandishing a brand new album coalescence of hauntingly hushed verses and Simone Smith entitled Heaven Upside Down. fantastically fierce choruses next as it Irvin Gamede ATackling themes such as sex, romance, saunters unsettlingly towards the violence and politics, the highly-anticipated comparatively cool and catchy “Kill4Me”. Front Cover - Ken Coleman sequel to 2015’s The Pale Emperor features This is succeeded by the seductively ten typically tumultuous tracks for fans to psychedelic “Saturnalia”, the dreamy yet www.artofkencoleman.com feast upon. energetic delivery of which ensures it stays It’s introduced through the sinister static entrancing until “Je$u$ Cri$i$” arrives to of “Revelation #12” before a brilliantly rivet with its raucous refrain and rebellious bracing riff begins to blare out beneath a instrumentation. -

Omega Auctions Ltd Catalogue 28 Apr 2020
Omega Auctions Ltd Catalogue 28 Apr 2020 1 REGA PLANAR 3 TURNTABLE. A Rega Planar 3 8 ASSORTED INDIE/PUNK MEMORABILIA. turntable with Pro-Ject Phono box. £200.00 - Approximately 140 items to include: a Morrissey £300.00 Suedehead cassette tape (TCPOP 1618), a ticket 2 TECHNICS. Five items to include a Technics for Joe Strummer & Mescaleros at M.E.N. in Graphic Equalizer SH-8038, a Technics Stereo 2000, The Beta Band The Three E.P.'s set of 3 Cassette Deck RS-BX707, a Technics CD Player symbol window stickers, Lou Reed Fan Club SL-PG500A CD Player, a Columbia phonograph promotional sticker, Rock 'N' Roll Comics: R.E.M., player and a Sharp CP-304 speaker. £50.00 - Freak Brothers comic, a Mercenary Skank 1982 £80.00 A4 poster, a set of Kevin Cummins Archive 1: Liverpool postcards, some promo photographs to 3 ROKSAN XERXES TURNTABLE. A Roksan include: The Wedding Present, Teenage Fanclub, Xerxes turntable with Artemis tonearm. Includes The Grids, Flaming Lips, Lemonheads, all composite parts as issued, in original Therapy?The Wildhearts, The Playn Jayn, Ween, packaging and box. £500.00 - £800.00 72 repro Stone Roses/Inspiral Carpets 4 TECHNICS SU-8099K. A Technics Stereo photographs, a Global Underground promo pack Integrated Amplifier with cables. From the (luggage tag, sweets, soap, keyring bottle opener collection of former 10CC manager and music etc.), a Michael Jackson standee, a Universal industry veteran Ric Dixon - this is possibly a Studios Bates Motel promo shower cap, a prototype or one off model, with no information on Radiohead 'Meeting People Is Easy 10 Min Clip this specific serial number available. -

Watershed Planning Commission
Scott Watershed Management Organization 200 Fourth Avenue West Shakopee, MN 55379-1220 0 952-496-8054 Fax 952-496-8496 www.co.scott.mn.us AGENDA Scott WMO – Watershed Planning Commission May 24, 2021 4:00 p.m. Watershed Planning Commission Meeting Video Conference I. Call to Order Action II. Approval of Agenda and Meeting Minutes a. April 26, 2021 Minutes Action III. Staff Reports a. Scott SWCD - TK Information b. Scott WMO - VS Information IV. Ongoing Business a. Project Updates - RH Information b. Program Updates – MBE Information c. Wake Boats Information V. New Business a. Public Hearing: 2020 MS4/SWPPP – Megan Tasca Action b. Kevin Koepp Grade Stabilization Application - RH Action VI. Adjourn Action Scott Watershed Management Organization 200 Fourth Avenue West Shakopee, MN 55379-1220 952-496-8054 Fax 952-496-8496 www.scottcountymn.gov/wmo Scott WMO – Watershed Planning Commission Meeting Minutes April 26th, 2021 I. Call to order Commissioner Weaver called to order the regular meeting of the Watershed Planning Commission meeting at 4:01 PM on April 26th, 2021 at Virtual Conference via Zoom. Specific details and video of the entire April 26th, 2021 Scott WMO Watershed Planning Commission Meeting is available for viewing on the Scott County Website. The video link can be viewed at: Scott WMO Planning Commission: February 22, 2021 - YouTube II. Roll call Members Present: Members Absent: Staff Present: Others Present: Pam Caselius Vanessa Strong Troy Kuphal Virgil Pint Melissa Bokman- Bruce Loney Rita Weaver Ermer Tom Wolf Brian Schmidt Ryan Holzer Mark Vierling Domi Archiebald Kevin Shea Joe Thill III. -

THE COLLECTED POEMS of HENRIK IBSEN Translated by John Northam
1 THE COLLECTED POEMS OF HENRIK IBSEN Translated by John Northam 2 PREFACE With the exception of a relatively small number of pieces, Ibsen’s copious output as a poet has been little regarded, even in Norway. The English-reading public has been denied access to the whole corpus. That is regrettable, because in it can be traced interesting developments, in style, material and ideas related to the later prose works, and there are several poems, witty, moving, thought provoking, that are attractive in their own right. The earliest poems, written in Grimstad, where Ibsen worked as an assistant to the local apothecary, are what one would expect of a novice. Resignation, Doubt and Hope, Moonlight Voyage on the Sea are, as their titles suggest, exercises in the conventional, introverted melancholy of the unrecognised young poet. Moonlight Mood, To the Star express a yearning for the typically ethereal, unattainable beloved. In The Giant Oak and To Hungary Ibsen exhorts Norway and Hungary to resist the actual and immediate threat of Prussian aggression, but does so in the entirely conventional imagery of the heroic Viking past. From early on, however, signs begin to appear of a more personal and immediate engagement with real life. There is, for instance, a telling juxtaposition of two poems, each of them inspired by a female visitation. It is Over is undeviatingly an exercise in romantic glamour: the poet, wandering by moonlight mid the ruins of a great palace, is visited by the wraith of the noble lady once its occupant; whereupon the ruins are restored to their old splendour. -

Gerold L. Schiebler, MD
ORAL HISTORY PROJECT Gerold L. Schiebler, MD Interviewed by Howard A. Pearson, MD March 18, 2000 Amelia Island, Florida This interview was supported by a donation from: The Florida Chapter of the American Academy of Pediatrics/Florida Pediatric Society https://www.aap.org/pediatrichistorycenter ã2001 American Academy of Pediatrics Elk Grove Village, IL Gerold L. Schiebler, MD Interviewed by Howard A. Pearson, MD Preface i About the Interviewer ii Interview of Gerold L. Schiebler, MD 1 Index of Interview 86 Curriculum Vita, Gerold L. Schiebler, MD 90 PREFACE Oral history has its roots in the sharing of stories which has occurred throughout the centuries. It is a primary source of historical data, gathering information from living individuals via recorded interviews. Outstanding pediatricians and other leaders in child health care are being interviewed as part of the Oral History Project at the Pediatric History Center of the American Academy of Pediatrics. Under the direction of the Historical Archives Advisory Committee, its purpose is to record and preserve the recollections of those who have made important contributions to the advancement of the health care of children through the collection of spoken memories and personal narrations. This volume is the written record of one oral history interview. The reader is reminded that this is a verbatim transcript of spoken rather than written prose. It is intended to supplement other available sources of information about the individuals, organizations, institutions, and events which are discussed. The use of face-to-face interviews provides a unique opportunity to capture a firsthand, eyewitness account of events in an interactive session. -
On Stage (Extra): a 'Curious' Case of Broadway-Style Entertainment
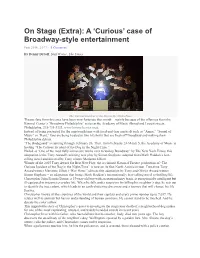
On Stage (Extra): A ‘Curious’ case of Broadway-style entertainment Feb 25th, 2017 · 0 Comment By Denny Dyroff, Staff Writer, The Times The Curious Incident of the Dog in the Night-Time. Theater fans from this area have been very fortunate this month – mainly because of the offerings from the Kimmel Center’s “Broadway Philadelphia” series at the Academy of Music (Broad and Locust streets, Philadelphia, 215-731-3333, www.kimmelcenter.org). Instead of being presented for the umpteenth time with tried-and-true musicals such as “Annie,” “Sound of Music” or “Rent,” fans are being treated to two hit shows that are fresh off Broadway and making their Philadelphia debuts. “The Bodyguard” is running through February 26. Then, from February 28-March 5, the Academy of Music is hosting “The Curious Incident of the Dog in the Night-Time.” Hailed as “One of the most fully immersive works ever to wallop Broadway” by The New York Times, this adaptation is the Tony Award®-winning new play by Simon Stephens, adapted from Mark Haddon’s best- selling novel and directed by Tony winner Marianne Elliott. Winner of the 2015 Tony Award for Best New Play, the acclaimed National Theatre production of “The Curious Incident of the Dog in the Night-Time” is now on its first North American tour. Two-time Tony Award winner Marianne Elliott (“War Horse”) directs this adaptation by Tony and Olivier Award winner Simon Stephens – an adaptation that brings Mark Haddon’s internationally best-selling novel to thrilling life. Christopher John Francis Boone, a 15-year-old boy with an extraordinary brain, is exceptionally intelligent but ill-equipped to interpret everyday life. -

The Broadsheet
May 2018 Issue XXIV THE BROADSHEET Seniors pose with inductees to Sigma Tau Delta Fifth Annual English Awards Ceremony This Issue: Celebrates Shared Scholarship, Award-Winning Verse, and Seniors Preparing for Graduation Poetry, Sanity, and By The Broadsheet Staff the Fifth Annual English Award Approximately fifty faculty, staff, students and family attended the fifth Ceremony annual English Awards Ceremony held on April 12 at 4 pm at the Merrimack College Writers House. The event consisted of a robust agenda, which Guest Speaker Tanya included the induction of eight new members into the Sigma Tau Delta Larkin Guides International Honor Society, the distribution of graduation cords to nine Majors along an seniors, a slide show from four of the five English majors who presented Important Path original scholarly and creative works at this year’s Sigma Tau Delta annual Sigma Tau Delta convention, the awarding of cash prizes to the three place winners in the Rev. John R. Aherne 2018 Poetry Contest, and a reading by poet Tanya Larkin, Conference 2018 Tufts University Lecturer in Creative Writing and author of two collections of original poetry, My Scarlet Ways, winner of the 2011 Saturnalia prize, and The Cryptic Manson Hothouse Orphan. of Heaven Upside Down The program also included readings by Aherne Poetry contest winners Bridget Kennedy (“Where I’m From,” first place), Dan Roussel (“Things Creating a Life in the I’ve Never Done,” second place), and Dakota Durbin (“Deer” and “Lucy Automated Future: Brook,” which tied for third place in the contest voting). In addition to her Mark Cuban on the reading, Larkin shared her thoughts about why poetry remains crucial to Liberal Arts emotional wellbeing. -

“I Am Your Faggot Anti-Pope”: an Exploration of Marilyn Manson As a Transgressive Artist
European journal of American studies 12-2 | 2017 Summer 2017, including Special Issue: Popularizing Politics: The 2016 U.S. Presidential Election “I Am Your Faggot Anti-Pope”: An Exploration of Marilyn Manson as a Transgressive Artist Coco d’Hont Electronic version URL: http://journals.openedition.org/ejas/12098 DOI: 10.4000/ejas.12098 ISSN: 1991-9336 Publisher European Association for American Studies Electronic reference Coco d’Hont, « “I Am Your Faggot Anti-Pope”: An Exploration of Marilyn Manson as a Transgressive Artist », European journal of American studies [Online], 12-2 | 2017, document 14, Online since 01 August 2017, connection on 19 April 2019. URL : http://journals.openedition.org/ejas/12098 ; DOI : 10.4000/ ejas.12098 This text was automatically generated on 19 April 2019. Creative Commons License “I Am Your Faggot Anti-Pope”: An Exploration of Marilyn Manson as a Transgres... 1 “I Am Your Faggot Anti-Pope”: An Exploration of Marilyn Manson as a Transgressive Artist Coco d’Hont 1 “As a performer,” Marilyn Manson announced in his autobiography, “I wanted to be the loudest, most persistent alarm clock I could be, because there didn’t seem to be any other way to snap society out of its Christianity- and media-induced coma” (Long Hard Road 80).i With this mission statement, expressed in 1998, the performer summarized a career characterized by harsh-sounding music, disturbing visuals, and increasingly controversial live performances. At first sight, the red thread running through the albums he released during the 1990s is a harsh attack on American ideologies. On his debut album Portrait of an American Family (1994), for example, Manson criticizes ideological constructs such as the nuclear family, arguing that the concept is often used to justify violent pro-life activism.ii Proclaiming that “I got my lunchbox and I’m armed real well” and that “next motherfucker’s gonna get my metal,” he presents himself as a personification of teenage angst determined to destroy his bullies, be they unfriendly classmates or the American government. -

Transgressive Queer Embodiment in the Music Videos of Marilyn Manson
“It’s All Me… In One Way or Another”: Transgressive Queer Embodiment in the Music Videos of Marilyn Manson by Brandon Peter Masterman Bachelor of Music in Saxophone Performance, Youngstown State University, 2007 Master of Library and Information Science, University of Pittsburgh, 2008 Submitted to the Graduate Faculty of Dietrich School of Arts and Sciences in partial fulfillment of the requirements for the degree of Master of Arts in Musicology University of Pittsburgh 2012 UNIVERSITY OF PITTSBURGH Dietrich School of Arts and Sciences This thesis was presented by Brandon Peter Masterman It was defended on March 30, 2012 and approved by James P. Cassaro, MA, MLS, Adjunct Assistant Professor of Music Deane L. Root, PhD, Professor of Music Todd W. Reeser, PhD, Associate Professor of French Thesis Advisor: Adriana Helbig, PhD, Assistant Professor of Music ii Copyright © by Brandon Peter Masterman 2012 iii “It’s All Me… In One Way or Another”: Transgressive Queer Embodiment in the Music Videos of Marilyn Manson Brandon Peter Masterman, M.L.I.S., M.A. University of Pittsburgh, 2012 My work attempts to understand the deployment of transgressive queerness in contemporary American popular music videos. Rather than aligning with either the conservative moral panics or liberal arguments regarding free speech, I suggest that productive alternative understandings exist outside of this oppositional binary. Focusing on Marilyn Manson, particularly, I analyze how various performances open up a space of potentiality for greater imaginings of embodiment and erotics. The music of Marilyn Manson presents a scathing critique of the cultural landscape of the United States in the late twentieth and early twenty-first centuries. -

Songs by Artist
TOTALLY TWISTED KARAOKE Songs by Artist 37 SONGS ADDED IN SEP 2021 Title Title (HED) PLANET EARTH 2 CHAINZ, DRAKE & QUAVO (DUET) BARTENDER BIGGER THAN YOU (EXPLICIT) 10 YEARS 2 CHAINZ, KENDRICK LAMAR, A$AP, ROCKY & BEAUTIFUL DRAKE THROUGH THE IRIS FUCKIN PROBLEMS (EXPLICIT) WASTELAND 2 EVISA 10,000 MANIACS OH LA LA LA BECAUSE THE NIGHT 2 LIVE CREW CANDY EVERYBODY WANTS ME SO HORNY LIKE THE WEATHER WE WANT SOME PUSSY MORE THAN THIS 2 PAC THESE ARE THE DAYS CALIFORNIA LOVE (ORIGINAL VERSION) TROUBLE ME CHANGES 10CC DEAR MAMA DREADLOCK HOLIDAY HOW DO U WANT IT I'M NOT IN LOVE I GET AROUND RUBBER BULLETS SO MANY TEARS THINGS WE DO FOR LOVE, THE UNTIL THE END OF TIME (RADIO VERSION) WALL STREET SHUFFLE 2 PAC & ELTON JOHN 112 GHETTO GOSPEL DANCE WITH ME (RADIO VERSION) 2 PAC & EMINEM PEACHES AND CREAM ONE DAY AT A TIME PEACHES AND CREAM (RADIO VERSION) 2 PAC & ERIC WILLIAMS (DUET) 112 & LUDACRIS DO FOR LOVE HOT & WET 2 PAC, DR DRE & ROGER TROUTMAN (DUET) 12 GAUGE CALIFORNIA LOVE DUNKIE BUTT CALIFORNIA LOVE (REMIX) 12 STONES 2 PISTOLS & RAY J CRASH YOU KNOW ME FAR AWAY 2 UNLIMITED WAY I FEEL NO LIMITS WE ARE ONE 20 FINGERS 1910 FRUITGUM CO SHORT 1, 2, 3 RED LIGHT 21 SAVAGE, OFFSET, METRO BOOMIN & TRAVIS SIMON SAYS SCOTT (DUET) 1975, THE GHOSTFACE KILLERS (EXPLICIT) SOUND, THE 21ST CENTURY GIRLS TOOTIMETOOTIMETOOTIME 21ST CENTURY GIRLS 1999 MAN UNITED SQUAD 220 KID X BILLEN TED REMIX LIFT IT HIGH (ALL ABOUT BELIEF) WELLERMAN (SEA SHANTY) 2 24KGOLDN & IANN DIOR (DUET) WHERE MY GIRLS AT MOOD (EXPLICIT) 2 BROTHERS ON 4TH 2AM CLUB COME TAKE MY HAND -
Substance Use Disorder Treatment for People with Co-Occurring Disorders UPDATED 2020
Substance Use Disorder Treatment for People With Co-Occurring Disorders UPDATED 2020 TREATMENT IMPROVEMENT PROTOCOL TIP 42 This page intentionally left blank. TIP 42 Please share your thoughts about this publication by completing a brief online survey at: www.surveymonkey.com/r/KAPPFS The survey takes about 7 minutes to complete and is anonymous. Your feedback will help SAMHSA develop future products. i This page intentionally left blank. TIP 42 Contents Foreword vii Executive Summary ix Overall Key Messages ix Content Overview x Consensus Panel xvii TIP Development Participants xvii KAP Expert Panel and Federal Government Participants xviii Publication Information xxvii Chapter 1—Introduction to Substance Use Disorder Treatment for People With Co-Occurring Disorders 1 Scope of This TIP 2 Terminology in This TIP 3 Important Developments That Led to This TIP Update 6 Why Do We Need a TIP on CODs? 7 The Complex, Unstable, and Bidirectional Nature of CODs 11 Conclusion 12 Chapter 2— Guiding Principles for Working With People Who Have Co-Occurring Disorders 13 General Guiding Principles 14 Guidelines for Counselors and Other Providers 16 Guidelines for Administrators and Supervisors 21 Conclusion 29 Chapter 3—Screening and Assessment of Co-Occurring Disorders 31 Screening and Basic Assessment for CODs 32 The Complete Screening and Assessment Process 36 Considerations in Treatment Matching 65 Conclusion 68 Chapter 4—Mental and Substance-Related Disorders: Diagnostic and Cross-Cutting Topics 69 Depressive Disorders 71 Bipolar I Disorder 76 Posttraumatic -
Partner Név Jellemző Művek 100 BANDS PUBLISHING LUCKY YOU /#/ RINGER /#/ SIT DOWN /#/ KILLSHOT /#/ GOOD GUY FEAT JESSIE REYEZ
Partner név Jellemző Művek 100 BANDS PUBLISHING LUCKY YOU /#/ RINGER /#/ SIT DOWN /#/ KILLSHOT /#/ GOOD GUY FEAT JESSIE REYEZ 13 MOONS MUSIC BLOW /#/ KEEP PLAYING /#/ KEEP ME UP ALL NIGHT /#/ TOGETHER WE RUN /#/ BIGROOM BLITZ (RADIO MIX) 14 PRODUCTIONS SARL TIC TIC TAC /#/ OU SONT LES REVES /#/ PLACE DES GRANDS HOMMES /#/ QUI A LE DROIT /#/ JE SERAI LA POUR LA SUITE 1794 MUSIC AMERICAN BOOK OF SECRETS CUES /#/ AMERICA S BOOK OF SECRETS CUES /#/ BMOC /#/ LIMO HIP HOP VER 4 /#/ JOURNEY THROUGH TIME 1819 BROADWAY MUSIC DAYDREAM /#/ STORY S OVER (THE) /#/ STORY S OVER /#/ DAYDREAM (DJ NEWIK & STARWHORES REMIX) /#/ VADONATÚJ ÉRZÉS 1916 PUBLISHING MIDDLE (THE) /#/ HATE ME /#/ RUIN MY LIFE /#/ SLOW DANCE /#/ IF IT AIN T LOVE 23DB MUSIC RAPTURE /#/ HONEST SLEEP /#/ PALM DREAMS /#/ FLOWERS AND YOU /#/ DNA 24 HOUR SERVICE STATION ON THE LOOKOUT 2L E-SCORE UBI CARITAS /#/ SERENITY /#/ SNOW IN NEW YORK, FOR PIANO /#/ HUDSON /#/ ROXBURY PARK, FOR PIANO 2WAYTRAFFIC UK RIGHTS LTD TODAY S NAME - MAI JÁTÉKOSOK /#/ TODAY S NAMES /#/ WHAT IS THE ORDER - SORREND 3 WEDDINGS MUSIC SOMETHING ABOUT DECEMBER /#/ MAKE ME BELIEVE AGAIN /#/ HERE S TO NEVER GROWING UP /#/ JET BLACK HEART (START AGAIN) /#/ LET ME GO 360 MUSIC PUBLISHING LTD ONLY ONE /#/ IF YOU KNEW /#/ DON T BELONG /#/ HUMANICA /#/ MINIMAL LIFE 386MUSIC DON T LET GO /#/ VIOLET ALONE 3BEAT MUSIC LIMITED QUESTIONS /#/ MAN BEHIND THE SUN /#/ CONNECTION /#/ WHO'S LOVING YOU (PART 1) /#/ LINK UP 4 REAL MUSIC ANGELS LANDING /#/ EUGINA 2000 50 CENT MUSIC BEST FRIEND /#/ HATE IT OR LOVE IT /#/ HUSTLER S AMBITION