Lysogeny of Ten Mycobacteriophages for Host Mycobacterium Tuberculosis H37ra
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Table S5. the Information of the Bacteria Annotated in the Soil Community at Species Level
Table S5. The information of the bacteria annotated in the soil community at species level No. Phylum Class Order Family Genus Species The number of contigs Abundance(%) 1 Firmicutes Bacilli Bacillales Bacillaceae Bacillus Bacillus cereus 1749 5.145782459 2 Bacteroidetes Cytophagia Cytophagales Hymenobacteraceae Hymenobacter Hymenobacter sedentarius 1538 4.52499338 3 Gemmatimonadetes Gemmatimonadetes Gemmatimonadales Gemmatimonadaceae Gemmatirosa Gemmatirosa kalamazoonesis 1020 3.000970902 4 Proteobacteria Alphaproteobacteria Sphingomonadales Sphingomonadaceae Sphingomonas Sphingomonas indica 797 2.344876284 5 Firmicutes Bacilli Lactobacillales Streptococcaceae Lactococcus Lactococcus piscium 542 1.594633558 6 Actinobacteria Thermoleophilia Solirubrobacterales Conexibacteraceae Conexibacter Conexibacter woesei 471 1.385742446 7 Proteobacteria Alphaproteobacteria Sphingomonadales Sphingomonadaceae Sphingomonas Sphingomonas taxi 430 1.265115184 8 Proteobacteria Alphaproteobacteria Sphingomonadales Sphingomonadaceae Sphingomonas Sphingomonas wittichii 388 1.141545794 9 Proteobacteria Alphaproteobacteria Sphingomonadales Sphingomonadaceae Sphingomonas Sphingomonas sp. FARSPH 298 0.876754244 10 Proteobacteria Alphaproteobacteria Sphingomonadales Sphingomonadaceae Sphingomonas Sorangium cellulosum 260 0.764953367 11 Proteobacteria Deltaproteobacteria Myxococcales Polyangiaceae Sorangium Sphingomonas sp. Cra20 260 0.764953367 12 Proteobacteria Alphaproteobacteria Sphingomonadales Sphingomonadaceae Sphingomonas Sphingomonas panacis 252 0.741416341 -
Wo 2010/025267 A2
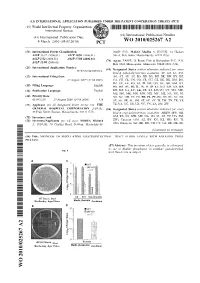
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date 4 March 2010 (04.03.2010) WO 2010/025267 A2 (51) International Patent Classification: 02459 (US). MALO, Madhu S. [US/US]; 14 Hudson A61K 33/42 (2006.01) A61P 19/02 (2006.01) Street, Watertown, Massachusetts 02474 (US). A61P 1/12 (2006.01) A61P 37/08 (2006.01) (74) Agent: FASSE, J. Peter; Fish & Richardson P.C., P.O. A61P 31/04 (2006.01) Box 1022, Minneapolis, Minnesota 55440-1022 (US). (21) International Application Number: (81) Designated States (unless otherwise indicated, for every PCT/US2009/055216 kind of national protection available): AE, AG, AL, AM, (22) International Filing Date: AO, AT, AU, AZ, BA, BB, BG, BH, BR, BW, BY, BZ, 27 August 2009 (27.08.2009) CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, DO, DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, (25) Filing Language: English HN, HR, HU, ID, IL, IN, IS, JP, KE, KG, KM, KN, KP, (26) Publication Language: English KR, KZ, LA, LC, LK, LR, LS, LT, LU, LY, MA, MD, ME, MG, MK, MN, MW, MX, MY, MZ, NA, NG, NI, (30) Priority Data: NO, NZ, OM, PE, PG, PH, PL, PT, RO, RS, RU, SC, SD, 61/093,129 29 August 2008 (29.08.2008) US SE, SG, SK, SL, SM, ST, SV, SY, TJ, TM, TN, TR, TT, (71) Applicant (for all designated States except US): THE TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, ZW. -

From Genotype to Phenotype: Inferring Relationships Between Microbial Traits and Genomic Components
From genotype to phenotype: inferring relationships between microbial traits and genomic components Inaugural-Dissertation zur Erlangung des Doktorgrades der Mathematisch-Naturwissenschaftlichen Fakult¨at der Heinrich-Heine-Universit¨atD¨usseldorf vorgelegt von Aaron Weimann aus Oberhausen D¨usseldorf,29.08.16 aus dem Institut f¨urInformatik der Heinrich-Heine-Universit¨atD¨usseldorf Gedruckt mit der Genehmigung der Mathemathisch-Naturwissenschaftlichen Fakult¨atder Heinrich-Heine-Universit¨atD¨usseldorf Referent: Prof. Dr. Alice C. McHardy Koreferent: Prof. Dr. Martin J. Lercher Tag der m¨undlichen Pr¨ufung: 24.02.17 Selbststandigkeitserkl¨ arung¨ Hiermit erkl¨areich, dass ich die vorliegende Dissertation eigenst¨andigund ohne fremde Hilfe angefertig habe. Arbeiten Dritter wurden entsprechend zitiert. Diese Dissertation wurde bisher in dieser oder ¨ahnlicher Form noch bei keiner anderen Institution eingereicht. Ich habe bisher keine erfolglosen Promotionsversuche un- ternommen. D¨usseldorf,den . ... ... ... (Aaron Weimann) Statement of authorship I hereby certify that this dissertation is the result of my own work. No other person's work has been used without due acknowledgement. This dissertation has not been submitted in the same or similar form to other institutions. I have not previously failed a doctoral examination procedure. Summary Bacteria live in almost any imaginable environment, from the most extreme envi- ronments (e.g. in hydrothermal vents) to the bovine and human gastrointestinal tract. By adapting to such diverse environments, they have developed a large arsenal of enzymes involved in a wide variety of biochemical reactions. While some such enzymes support our digestion or can be used for the optimization of biotechnological processes, others may be harmful { e.g. mediating the roles of bacteria in human diseases. -

Ldentif Ication of Clinically Relevant Viridans Streptococci by Analysis of Transfer DNA Intergenic Spacer Length Polymorphism
international Journal of Systematic Bacteriology (1 999), 49, 1 59 1-1 598 Printed in Great Britain ldentif ication of clinically relevant viridans streptococci by analysis of transfer DNA intergenic spacer length polymorphism Y. De Gheldre,' P. Vandamme,213H. Goossens3and M. J. Struelens' Author for correspondence: Yves De Gheldre. Tel: + 32 2 555 4517. Fax: + 32 2 555 6459. e-mail : [email protected] 1 Department of The utility of PCR analysis of transfer DNA intergenic spacer length Microbiology, HBpital polymorphism @DNA-ILP)for the identification to the species level of clinically Erasme, Universite Libre de Bruxelles, 808 Route de relevant viridans streptococci was evaluated with a collection of reference Lennik, 1070 Brussels, strains of 15 species of the salivarius, anginosus, mitis and mutans rRNA Belgium homology groups. PCR products generated by using fluorescent, outwardly 2 Laboratory of directed, consensus tDNA primers were analysed by electrophoresis on Microbiology and denaturating polyacrylamide gels and by laser fluorescence scanning. Eleven BCCM/LMG Culture Collection, University of species showed specific and distinct tDNA patterns : Streptococcus cristatus, Ghent, Belgium Streptococcus gordonii, Streptococcus oralis, Streptococcus mitis, 3 Laboratory of Medical Streptococcus pneumoniae, Streptococcus sanguinis, Streptococcus Microbiology, University parasanguinis, Streptococcus anginosus, Streptococcus mutans, Streptococcus Hospital Antwerp, criceti and Streptococcus ratti. Indistinguishable patterns were obtained Antwerp, Belgium among two groups of species : Streptococcus vestibularis and Streptococcus salivarius on the one hand and Streptococcus constellatus and Streptococcus intermedius on the other. 5. mitis strains produced heterogeneous patterns that could be separated into three groups: a group containing S. mitis biovar 1 and two S, mitis biovar 2 groups, one of which clustered with S. -
Patterns of Horizontal Gene Transfer Into the Geobacillus Clade
Imperial College London London Institute of Medical Sciences Patterns of Horizontal Gene Transfer into the Geobacillus Clade Alexander Dmitriyevich Esin September 2018 Submitted in part fulfilment of the requirements for the degree of Doctor of Philosophy of Imperial College London For my grandmother, Marina. Without you I would have never been on this path. Your unwavering strength, love, and fierce intellect inspired me from childhood and your memory will always be with me. 2 Declaration I declare that the work presented in this submission has been undertaken by me, including all analyses performed. To the best of my knowledge it contains no material previously published or presented by others, nor material which has been accepted for any other degree of any university or other institute of higher learning, except where due acknowledgement is made in the text. 3 The copyright of this thesis rests with the author and is made available under a Creative Commons Attribution Non-Commercial No Derivatives licence. Researchers are free to copy, distribute or transmit the thesis on the condition that they attribute it, that they do not use it for commercial purposes and that they do not alter, transform or build upon it. For any reuse or redistribution, researchers must make clear to others the licence terms of this work. 4 Abstract Horizontal gene transfer (HGT) is the major driver behind rapid bacterial adaptation to a host of diverse environments and conditions. Successful HGT is dependent on overcoming a number of barriers on transfer to a new host, one of which is adhering to the adaptive architecture of the recipient genome. -

an Emerging Pathogen for Salmonid Culture Jesús L
, an emerging pathogen for salmonid culture Jesús L. Romalde, Carmen Ravelo, Iván Valdés, Beatriz Magariños, Eduardo de la Fuente, Carolina San Martín, Rubén Avendaño-Herrera, Alicia E. Toranzo To cite this version: Jesús L. Romalde, Carmen Ravelo, Iván Valdés, Beatriz Magariños, Eduardo de la Fuente, et al.. , an emerging pathogen for salmonid culture. Veterinary Microbiology, Elsevier, 2008, 130 (1-2), pp.198. 10.1016/j.vetmic.2007.12.021. hal-00532381 HAL Id: hal-00532381 https://hal.archives-ouvertes.fr/hal-00532381 Submitted on 4 Nov 2010 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Accepted Manuscript Title: Streptococcus phocae, an emerging pathogen for salmonid culture Authors: Jesus´ L. Romalde, Carmen Ravelo, Ivan´ Valdes,´ Beatriz Magarinos,˜ Eduardo de la Fuente, Carolina San Mart´ın, Ruben´ Avendano-Herrera,˜ Alicia E. Toranzo PII: S0378-1135(07)00644-X DOI: doi:10.1016/j.vetmic.2007.12.021 Reference: VETMIC 3926 To appear in: VETMIC Received date: 25-6-2007 Revised date: 12-12-2007 Accepted date: 13-12-2007 Please cite this article as: Romalde, J.L., Ravelo, C., Valdes,´ I., Magarinos,˜ B., de la Fuente, E., Mart´ın, C.S., Avendano-Herrera,˜ R., Toranzo, A.E., Streptococcus phocae, an emerging pathogen for salmonid culture, Veterinary Microbiology (2007), doi:10.1016/j.vetmic.2007.12.021 This is a PDF file of an unedited manuscript that has been accepted for publication. -

Are You Suprised ?
A DAMB 711 Microbiology Exam 2A 100 points September 27, 2011 Your name: _____________________________________________ Exam # ___________ Seat # ____________ 1 I. Multiple Choice: Choose the ONE BEST answer. Mark the correct answer in Part 1 of your answer sheet. 1. Which of the following conveys the highest risk of nosocomial infection to a hospitalized patient? A. the hospital environment (rooms, floors, fomites) B. invasive medical devices (catheters, respirators, etc.) C. hospital personnel, including physicians D. mechanical vectors 2. The clonality of pathogenic bacteria refers to: A. the environmental regulation of genes encoding virulence factors B. the acquisition of virulence determinants encoded on extra-chromosomal elements C. the infective dose of a specific species of bacteria D. opportunistic pathogens E. only a few strains in a species will be the etiologic agent of a disease 3. Diseases caused by this genus of bacteria are never transmitted through contaminated food. A. Listeria B. Staphylococcus C. Mycobacteria D. Corynebacteria 4. When Vibrio cholera is moved from a high salt, basic environment to isotonic conditions, with neutral pH a sensor kinase in the bacterium phosphorylates a response regulator that initiates transcription. This is an example of: A. the environmental regulation of genes encoding virulence factors B. the acquisition of virulence determinants encoded on extra-chromosomal elements C. the infective dose of a specific species of bacteria D. opportunistic pathogens E. only a few strains in a species will be the etiologic agent of a disease 5. In which form of tuberculosis is a patient coughing up infectious material? A. miliary B. active C. latent/dormant D. -

Review Memorandum
510(k) SUBSTANTIAL EQUIVALENCE DETERMINATION DECISION SUMMARY A. 510(k) Number: K181663 B. Purpose for Submission: To obtain clearance for the ePlex Blood Culture Identification Gram-Positive (BCID-GP) Panel C. Measurand: Bacillus cereus group, Bacillus subtilis group, Corynebacterium, Cutibacterium acnes (P. acnes), Enterococcus, Enterococcus faecalis, Enterococcus faecium, Lactobacillus, Listeria, Listeria monocytogenes, Micrococcus, Staphylococcus, Staphylococcus aureus, Staphylococcus epidermidis, Staphylococcus lugdunensis, Streptococcus, Streptococcus agalactiae (GBS), Streptococcus anginosus group, Streptococcus pneumoniae, Streptococcus pyogenes (GAS), mecA, mecC, vanA and vanB. D. Type of Test: A multiplexed nucleic acid-based test intended for use with the GenMark’s ePlex instrument for the qualitative in vitro detection and identification of multiple bacterial and yeast nucleic acids and select genetic determinants of antimicrobial resistance. The BCID-GP assay is performed directly on positive blood culture samples that demonstrate the presence of organisms as determined by Gram stain. E. Applicant: GenMark Diagnostics, Incorporated F. Proprietary and Established Names: ePlex Blood Culture Identification Gram-Positive (BCID-GP) Panel G. Regulatory Information: 1. Regulation section: 21 CFR 866.3365 - Multiplex Nucleic Acid Assay for Identification of Microorganisms and Resistance Markers from Positive Blood Cultures 2. Classification: Class II 3. Product codes: PAM, PEN, PEO 4. Panel: 83 (Microbiology) H. Intended Use: 1. Intended use(s): The GenMark ePlex Blood Culture Identification Gram-Positive (BCID-GP) Panel is a qualitative nucleic acid multiplex in vitro diagnostic test intended for use on GenMark’s ePlex Instrument for simultaneous qualitative detection and identification of multiple potentially pathogenic gram-positive bacterial organisms and select determinants associated with antimicrobial resistance in positive blood culture. -

Prevalence of Different Streptococci Species in the Oral Cavity of Children and Adolescents Patricia Amoroso 1 Fernando A
Braz J Oral Sci. January/March 2003 - Vol. 2 - Number 4 Prevalence of different streptococci species in the oral cavity of children and adolescents Patricia Amoroso 1 Fernando A. de Ávila 1 Abstract Célia M. O. Gagliardi 1 Streptococci species were isolated, identified and counted in 262 sa- liva samples collected from 131 children and adolescents from a pub- 1 Agraries and Veterinary Sciences University lic school nursery at the city of Jaboticabal, SP. Four Streptococci Departament of Patology Veterinary - species harboring oral samples were identified biochemically, as Strep- Estadual Paulista University tococcus salivarius, Streptococcus mutans, Streptococcus rattus, Strep- Campus Jaboticabal – SP - Brazil [email protected] tococcus sobrinus, and streptococci of the mitis group. The mean Streptococcus counts obtained were 1.0 x 109 CFU/ml saliva for the 3 to 5 year age range, 1.5 x 109 CFU/mL saliva for the 6 to 8 year age range, and 2.0 x 109 CFU/mL saliva for the 12 to 14 year age range. The prevalence of Streptococci in saliva were: S. salivarius (89.31%), S. mutans (73.28%), S. salivarius + S. mutans (44.27%) by the stan- Received for publication: January 22, 2003 dard method. The tongue depressor method showed S. mutans Accepted: February 14, 2003 (62.59%), S. salivarius (77.86%), S. salivarius + S. mutans (33.58%). The analysis of both techniques showed significant agreement for Streptococcus isolation. Key Words Isolation, streptococci, children, saliva, collection techniques. Correspondence to: Patricia Amoroso Av. Eng. Necker C. Camargos, 1733 Cep: 14783-085 Barretos SP Brazil e-mail: [email protected] 164 Braz J Oral Sci. -

Streptococcus Laboratory General Methods
The reference used for compiling the methods in Section I is: Murray, P.R., Baron, E. J., Jorgensen, J.J., Pfaller, M.A., and Yolken, R.H. Manual of Clinical Microbiology, 8th ed. ASM Press: Washington, DC, 2003. The Streptococcus species identification methods in Section II were compiled by Dr. Lynn Shewmaker. Also thanks to input from several individuals, including Richard Facklam and Lucia Teixeira. Section I. 1. Accuprobe-Enterococcus Test………….………..4 2. Accuprobe-Pneumococcus Test …………..….….4 3. Acid formation in carbohydrate broth..................5 4. Arginine Hydrolysis……………………….……….6 5. Bacitracin Test……………………………………..7 6. Bile-esculin Test…………………………………...8 7. Bile solubility Test …………………………………9 8. CAMP Test…......................................................10 9. Catalase Test......................................................11 10. Clindamycin test………………………………….12 11. Esculin hydrolysis……………………………….. 13 12. Gas from MRS broth……………………………...14 13. Gram Stain………………………………………...15 14. Growth at 10 & 45C……………………………. 17 15. Hemolysis………………………………………….18 16. Hippurate hydrolysis…………………………… 19 17. Lancefield Group Antigen………………………..20 18. Leucine amino peptidase (LAP)…………………21 19. Litmus Milk Test…………………………………..22 20. Motility………………………………………………23 21. 6.5% NaCl Tolerace Test...................................24 22. Optochin…………………………………………….25 23. Pigmentation....................................................... 26 24. Pyridoxal Requirement Test (Vitamin B6)……….27 25. Pyrrolidonlarylamindase (PYR)............................28 26. -

Title: Bartonella Dynamics in Indigenous
Molecular diversity and prevalence of Helicobacter, Bartonella and Streptococcus in Mus musculus from sub-Antarctic Marion Island in relation to host diversity By Candice Eadie Submitted in partial fulfillment of the requirements for the degree Master of Science (Zoology) Faculty of Natural and Agricultural Sciences Department of Zoology and Entomology University of Pretoria Pretoria South Africa Supervisors: Prof A.D.S. Bastos, Prof M.N. Bester and Prof S.N. Venter December 2011 1 © University of Pretoria Declaration I, Candice Eadie hereby declare that the dissertation, which I hereby submit for the degree Master of Science (Zoology) at the University of Pretoria, is my own work and has not previously been submitted by me for a degree at this or any other tertiary institution. Signature: Date : 9/12/2011 2 Disclaimer This thesis consists of a series of chapters that have been prepared as stand-alone manuscripts for subsequent submission for publication purposes. Consequently, unavoidable overlaps and/or repetitions may occur between chapters. 3 Molecular diversity and prevalence of Helicobacter, Bartonella and Streptococcus in Mus musculus from sub-Antarctic Marion Island in relation to host diversity by Candice Eadie Mammal Research Institute (MRI), Department of Zoology and Entomology, University of Pretoria, Private Bag X20, Hatfield, 0028 South Africa SUPERVISORS: Prof. A.D.S. Bastos Mammal Research Institute (MRI), Department of Zoology and Entomology, University of Pretoria, Private Bag X20, Hatfield, 0028 South Africa Prof. M.N. Bester Mammal Research Institute (MRI), Department of Zoology and Entomology, University of Pretoria, Private Bag X20, Hatfield, 0028 South Africa. Prof. S.N. Venter Department of Microbiology and Plant pathology, University of Pretoria, Private Bag X20, Hatfield, 0028 South Africa. -

ISSN: 2320-5407 Int. J. Adv. Res. 8(12), 720-730
ISSN: 2320-5407 Int. J. Adv. Res. 8(12), 720-730 Journal Homepage: -www.journalijar.com Article DOI:10.21474/IJAR01/12203 DOI URL: http://dx.doi.org/10.21474/IJAR01/12203 RESEARCH ARTICLE A REVIEW ON MICROBIAL ECOLOGY OF MUTANS STREPTOCOCCI IN HUMAN MOUTH Dr. Apoorva Mehrotra1, Dr. Mohammad Iqbal2, Dr. Waleed Khalil Al Dahlawi3 and Dr. WalaSaad Al Raddadi4 1. Assistant Professor, Department of Conservative Dentistry & Endodontics, Career Postgraduate Institute of Dental Sciences and Hospital, Lucknow, India. 2. Associate Professor and Head, Department of Restorative Dental Sciences, Faculty of Dentistry- Al Baha University, Kingdom of Saudi Arabia. 3. Dentist, Al Hijra Dental Complex, Kingdom of Saudi Arabia. 4. Dentist, Sydalshuhada Primary Health Care Centre, Kingdom of Saudi Arabia. ……………………………………………………………………………………………….... Manuscript Info Abstract ……………………. ……………………………………………………………… Manuscript History The streptococci constitute a large and complex group of bacteria that Received: 20 October 2020 have widely varying characteristics and that under certain conditions Final Accepted: 24 November 2020 are capable of independent pathogenicity. In human mouth, the Published: December 2020 viridians streptococci are one of the main groups of bacteria and they are the most commonly occurring microorganisms in oral infections Key words:- Streptococcus, Dental Caries, Bacteria including dental caries. Copy Right, IJAR, 2020,. All rights reserved. …………………………………………………………………………………………………….... Introduction:- Streptococcus mutans were named by Clarke in 1924 due to its variable morphology after been isolated due to the fact that they were predominant in many human carious lesions. Clarke also found out that in artificially induced caries these Streptococcus mutans stuck closely to tooth surfaces. Characteristics and features of this cluster of streptococci have been termed as non-motile, catalase negative, gram positive cocci in medium or short chains1,2.