T He Growing Noncommunicable Disease Burden, a Challenge for the Countries of the Americas1
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
In This Issue: 11 Years All Optical Submarine Network Upgrades Of
66 n o v voice 2012 of the ISSn 1948-3031 Industry System Upgrades Edition In This Issue: 11 Years All Optical Submarine Network Upgrades of Upgrading Cables Systems? More Possibilities That You Originally Think Of! Excellence Reach, Reliability And Return On Investment: The 3R’s To Optimal Subsea Architecture Statistics Issue Issue Issue #64 Issue #3 #63 #2 Released Released Issue Released Released #65 Released 2 ISSN No. 1948-3031 PUBLISHER: Wayne Nielsen MANAGING EDITOR: Kevin G. Summers ovember in America is the month Forum brand which we will be rolling out we celebrate Thanksgiving. It during the course of the year, and which CONTRIBUTING WRITERS: Stewart Ash, is also the month SubTel Forum we believe will further enhance your James Barton, Bertrand Clesca, Dr Herve Fevrier, N Stephen Jarvis, Brian Lavallée, Pete LeHardy, celebrates our anniversary of existence, utility and enjoyment. We’re going to kick Vinay Rathore, Dr. Joerg Schwartz that now being 11 years going strong. it up a level or two, and think you will like the developments . And as always, it will Submarine Telecoms Forum magazine is When Ted and I established our little be done at no cost to our readers. published bimonthly by Submarine Telecoms magazine in 2001, our hope was to get Forum, Inc., and is an independent commercial enough interest to keep it going for a We will do so with two key founding publication, serving as a freely accessible forum for professionals in industries connected while. We had a list of contacts, an AOL principles always in mind, which annually with submarine optical fiber technologies and email address and a song in our heart; the I reaffirm to you, our readers: techniques. -

March 30, 2015 by ELECTRONIC FILING Marlene H. Dortch, Secretary Federal Communications Commission 445 12Th Street, S.W. Washin
(202) 223-7323 (202) 204-7371 [email protected] March 30, 2015 BY ELECTRONIC FILING Marlene H. Dortch, Secretary Federal Communications Commission 445 12th Street, S.W. Washington, D.C. 20554 Re: Joint Application for Transfer of Control of Cable Landing Licenses from Columbus Networks, Limited to Cable & Wireless Communications Plc, File Nos. SCL-T/C-20141121-00013 and SCL-T/C-20141121-00014; Applications for Transfer of Control of Section 214 Authorizations from Columbus Networks, Limited to Cable & Wireless Communications Plc, File Nos. ITC-T/C-20141121-00304 and ITC-T/C-20141121-00307 Dear Ms. Dortch: On Thursday, March 26, 2015, the undersigned counsel and representatives of Cable & Wireless Communications Plc (“C&W”) and Columbus Networks, Limited (“CNL”) met with members of the Commission’s staff to discuss the above-cited pending applications, and in particular Digicel’s pleadings and ex parte filing in the proceeding. Doc#: US1:9949275v3 Marlene H. Dortch, Secretary 2 Attending this meeting on behalf of Cable & Wireless Communications Plc were Belinda Bradbury, General Counsel, and Simeon Irvine, Chief Executive, Wholesale. C&W outside counsel Patrick Campbell and Diane Gaylor of Paul,Weiss, Rifkind, Wharton & Garrison LLP also attended. Attending on behalf of Columbus Networks, Limited were Paul Scott, President and Chief Operating Officer, Columbus Networks USA, Inc., and Victor A. Lago, Vice President of Legal Affairs, Columbus Networks USA, Inc. CNL outside counsel Ulises Pin of Morgan, Lewis & Bockius LLP also attended. Commission staff in attendance were, from the International Bureau, Nese Guendelsberger, Deputy Bureau Chief (by phone); Kathleen Collins, Assistant Bureau Chief; Walt Strack, Assistant Bureau Chief and Chief Economist; Howard Griboff, Acting Division Chief, Policy Division; David Krech, Associate Division Chief, Policy Division; Mark Uretsky, Senior Economist, Policy Division; Jodi Cooper, Senior Attorney, Policy Division; and, from the Office of General Counsel, James Bird. -

The Hidden Meaning in Those Letters and Numbers
International Journal of Humanities and Social Science Vol. 2 No. 19 [Special Issue – October 2012] The Hidden Meaning in Those Letters and Numbers Chuck Higgins, Ph.D. Dept. Finance/CIS Loyola Marymount Univ. 1 LMU Drive Los Angeles, CA 90045-8385 USA We all find number and letter codes around us. Many of these are both relevant and often easy to decode. Included herein are those most of us encounter: airport/ airline/airplane codes, alphabets, bonds, Braille, broadcast call letters, radio AM/FM, television, checks, corporations, credit cards, dates, highways, internet, license plates, measures, money, numbers, postal codes, postage stamps, railroads/trains, ships/boats, Social Security, stocks, telephone, temperature, time, and universal product codes. Not included herein are those that are field specific or important only to specialists. Thus not included are codes found in science, technology, special fields, and commerce; examples excluded include chemistry and physics, model numbers, ham radio and hobbies, expiration dates, and so on. All graphics herein are from Wikipedia or are mine. Thank you to Michelle Yeung and Zbigniew Przasnyski for their suggestions. Airports/Airlines/Airplanes ABC Airport codes are three letter mnemonics (four letters instead for pilots), some with historic references (ORD for O’Hare Airport previously called Orchard Field and MSY for New Orleans’ Moisant Field); see www.skygod.com for a full history. In the U.S. there are rarely airport codes starting with K, N, or W. The codes for Canadian airports usually start with a Y, but the reverse may not be true (YUM for Yuma International for example). A recommended website for flights is www.airfare.com . -

Artistic Swimming
ARTISTIC SWIMMING EVENTS Women (3) Duets Teams Highlight Mixed (1) Duets QUOTA Qualification Host NOC Total Men 7 1 8 Women 64 8 72 Total 71 9 80 athletes MAXIMUM QUOTA PER NOC EVENT Qualification Host NOC Total Duets 1 duet (2 athletes) 1 duet (2 athletes) 12 duets of 2 athletes Teams 1 team (8 athletes) 1 team (8 athletes) 8 teams of 8 athletes Highlight 1 team (8 athletes) 1 team (8 athletes) 8 teams of 8 athletes Mixed Duets 1 duet (2 athletes) 1 duet (2 athletes) 8 Duets of 2 athletes Total 9 athletes (8 women + 1 man) 9 athletes (8 women + 1 man) 80 athletes (72 women + 8 men) Athletes may register for more than one event. Eight teams with a maximum of 8 (eight) athletes each may participate in the team and highlight competition (no reserves will be allowed). Eight duets with a maximum of 2(two) athletes (one man and one woman) each may participate in the mixed duet competition (no reserves will be allowed). Twelve teams with a maximum of 24 athletes (no reserves will be allowed) may participate in the duet competition. As Host Country, Colombia automatically will qualify one team in each event, with a maximum of 9 athletes (8 women and 1 man). Athlete eligibility The athletes must have signed and submitted the Athlete Eligibility Condition Form. Only NOCs recognized by Panam Sports whose national swimming federations are affiliated with the International Swimming Federation (FINA) and the Union Americana de Natación (UANA) may enter athletes in the Cali 2021 Junior Pan American Games. -

ITU-Dstudygroups
ITU-D Study Groups Study period 2018-2021 Broadband development and connectivity solutions for rural and Question 5/1 Telecommunications/ remote areas ICTs for rural and remote areas Executive summary This annual deliverable reviews major backbone telecommunication Annual deliverable infrastructure installation efforts and approaches to last-mile connectivity, 2019-2020 describes current trends in last-mile connectivity and policy interventions and recommended last-mile technologies for use in rural and remote areas, as well as in small island developing States (SIDS). Discussions and contributions made during a workshop on broadband development in rural areas, held in September 2019, have been included in this document, which concludes with two sets of high-level recommendations for regulators and policy-makers, and for operators to use as guidelines for connecting rural and remote communities. 1 More information on ITU-D study groups: E-mail: [email protected] Tel.: +41 22 730 5999 Web: www.itu.int/en/ITU-D/study-groups ITU -D Study Groups Contents Executive summary 1 Introduction 3 Trends in telecommunication/ICT backbone infrastructure 4 Last mile-connectivity 5 Trends in last-mile connectivity 6 Business regulatory models and policies 7 Recommendations and guidelines for regulators and policy-makers 8 Recommendations and guidelines for operators 9 Annex 1: Map of the global submarine cable network 11 Annex 2: Listing of submarine cables (A-Y) 12 2 More information on ITU-D study groups: E-mail: [email protected] Tel.: +41 22 730 5999 Web: www.itu.int/en/ITU-D/study-groups ITU -D Study Groups Introduction The telecommunications/ICT sector and technologies have evolved over a long period of time, starting with ancient communication systems such as drum beating and smoke signals to the electric telegraph, the fixed telephone, radio and television, transistors, video telephony and satellite. -

Technology and the Geography of the Foreign Exchange Market
Working Paper Series Barry Eichengreen Cables, Sharks and Servers: Romain Lafarguette and Arnaud Mehl Technology and the Geography of the Foreign Exchange Market No 1889 / March 2016 Note: This Working Paper should not be reported as representing the views of the European Central Bank (ECB). The views expressed are those of the authors and do not necessarily reflect those of the ECB Abstract We analyze the impact of technology on production and trade in services, focusing on the foreign exchange market. We identify exogenous technological changes by the connection of countries to submarine fiber- optic cables used for electronic trading, but which were not laid for purposes related to the foreign exchange market. We estimate the impact of cable connections on the share of offshore foreign exchange transactions. Cable connections between local markets and matching servers in the major financial centers lower the fixed costs of trading currencies and increase the share of currency trades occurring onshore. At the same time, however, they attenuate the effect of standard spatial frictions such as distance, local market liquidity, and restrictive regulations that otherwise prevent transactions from moving to the major financial centers. Our estimates suggest that the second effect dominates. Technology dampens the impact of spatial frictions by up to 80 percent and increases, in net terms, the share of offshore trading by 21 percentage points. Technology also has economically important implications for the distribution of foreign exchange transactions across financial centers, boosting the share in global turnover of London, the world’s largest trading venue, by as much as one-third. -

Nber Working Paper Series Cables, Sharks and Servers
NBER WORKING PAPER SERIES CABLES, SHARKS AND SERVERS: TECHNOLOGY AND THE GEOGRAPHY OF THE FOREIGN EXCHANGE MARKET Barry Eichengreen Romain Lafarguette Arnaud Mehl Working Paper 21884 http://www.nber.org/papers/w21884 NATIONAL BUREAU OF ECONOMIC RESEARCH 1050 Massachusetts Avenue Cambridge, MA 02138 January 2016, Revised April 2021 We are grateful to Mark Aguiar, Pol Antràs, Thorsten Beck, Geert Bekaert, Bruno Biais, Jérôme Busca, Estelle Cantillon, Giancarlo Corsetti, Alexander Duering, Torsten Ehlers, Benoît Geller, Jérôme Héricourt, Jean Imbs, Takatoshi Ito, Amit Khandelwal, Philip Lane, Istvan Mak, Guy- Charles Marhic, Philippe Martin, Martin Uribe, Frank Packer, Hashem Pesaran, Romain Rancière, Andrew Rose, Alan Taylor and Xavier Vives for comments and discussions, as well as to seminar participants at the ECB, Goethe University Frankfurt and USC Dornsife and to participants at the Clausen Center Conference on Global Economic Issues, Berkeley, and to the Cambridge-INET conference on the microstructure of the FX market for comments. We thank Ziqi Li for excellent research assistance. We are also grateful to Denis Pêtre and Philip Wooldridge for providing unpublished Bank for International Settlements data on offshore foreign exchange trading. The views expressed are those of the authors and do not necessarily reflect those of the ECB, the Eurosystem, the IMF, or the National Bureau of Economic Research. NBER working papers are circulated for discussion and comment purposes. They have not been peer-reviewed or been subject to the review by the NBER Board of Directors that accompanies official NBER publications. © 2016 by Barry Eichengreen, Romain Lafarguette, and Arnaud Mehl. All rights reserved. Short sections of text, not to exceed two paragraphs, may be quoted without explicit permission provided that full credit, including © notice, is given to the source. -

Puerto Rico and Jamaica's Olympic Movement in Pan‐American Sport
The International Journal of the History of Sport ISSN: 0952-3367 (Print) 1743-9035 (Online) Journal homepage: http://www.tandfonline.com/loi/fhsp20 Colonial Olympism: Puerto Rico and Jamaica’s Olympic Movement in Pan‐American Sport, 1930 to the 1950s Antonio Sotomayor To cite this article: Antonio Sotomayor (2016) Colonial Olympism: Puerto Rico and Jamaica’s Olympic Movement in Pan‐American Sport, 1930 to the 1950s, The International Journal of the History of Sport, 33:1-2, 84-104, DOI: 10.1080/09523367.2016.1147429 To link to this article: http://dx.doi.org/10.1080/09523367.2016.1147429 Published online: 29 Feb 2016. Submit your article to this journal Article views: 83 View related articles View Crossmark data Full Terms & Conditions of access and use can be found at http://www.tandfonline.com/action/journalInformation?journalCode=fhsp20 Download by: [University of Illinois at Urbana-Champaign] Date: 22 April 2016, At: 11:07 THE INTERNATIONAL JOURNAL OF THE HISTORY OF SPORT, 2016 VOL. 33, NOS. 1–2, 84–104 http://dx.doi.org/10.1080/09523367.2016.1147429 Colonial Olympism: Puerto Rico and Jamaica’s Olympic Movement in Pan‐American Sport, 1930 to the 1950s Antonio Sotomayor University Library, Latin American and Caribbean Studies, University of Illinois, Urbana, IL, USA ABSTRACT KEYWORDS This paper examines how two Caribbean islands, Puerto Rico and Colonial Olympism; Puerto Jamaica, developed ideas of national identity while negotiating Rico; Jamaica; national political emancipation within two distinct, yet allied Anglophone identity; colonialism empires. We can see this process through the Olympic movement and referred to here as ‘colonial Olympism’. -
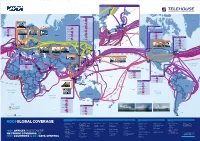
KDDI Global Network
JAPAN LANDING CABLES CHINA RUSSIA TEA-3 TEA Hokkaido-Sakhalin Cable System Ishikari Nakhodka JIH JAPAN JIH APCN-2 Russia-Japan EAC-C2C FASTER Chikura NORTH Akita SJC KOREA GREENLAND SJC2 PC-1 UNITED KINGDOM JAPAN Unity/EAC Pacific Tata TGN-Pacific Sea of Tata TGN-Pacific NCP Emi Tata TGN-Pacific Japan Sendai TPE FASTER APG Seoul Naoetsu Japan-U.S. HONG KONG ASE Kitaibaraki Shindu-Ri PC-1 AJC SOUTH Ajigaura WASHINGTON Cape D’Aguilar AAE-1 Maruyama JUPITER London KOREA Ibaraki Unity Japan-U.S. Oyama CORNWALL Tokyo JUPITER [2020] Harbour Pointe PC-1 EAC-C2C New Cross Pacific EAC-C2C Busan Miura Nagoya Emi Chung Hom Kok SJC TPE Keoje Apollo FRANCE GERMANY RUSSIA KJCN Maruyama Wada SJC2 Osaka Toyohashi Chikura EIG Shima Bude Miura FLAG Europe-Asia TAT-14 PLCN Yellow Kita-kyushu U.S. ICELAND Deep Water Bay SeaMeWe-3 Naoetsu RJCN Fukuoka OREGON TGN-IA Goonhilly Downs SeaMeWe-3 TPE APG Japan-U.S. APCN-2 AJC APCN-2 Bandon FASTER Porthcurno FLAG Europe-Asia JIH Miyazaki Paris Frankfurt Moscow Lantau Island AAG EAC-C2C TPE Southern Cross FINLAND EAC-C2C Hillsboro FLAG Europe-Asia FASTER NCP MOC Tata TGN-Pacific Skewjack FLAG Atlantic-1 Shima TPE CANADA RUSSIA JUPITER APG Tong Fuk FLAG/REACH NAL Japan-U.S. SJC2 Nedonna Beach TPE APG FLAG/REACH NAL PLCN [2019] PC-1 FEA NEW YORK / NEW JERSEY NORWAY St. Petersburg SMW-3 FEA Hawaiki SWEDEN APG SJC2 Pacific City TEA-2 APCN-2 New Cross Pacific Tseung Kwan O ASE APG Bellport, NY Yellow ESTONIA EAC-C2C PACIFIC TEA EAC-C2C Wada FLAG/REACH NAL JUPITER [2020] FASTER SJC2 [2020] OCEAN Island Park, NY FLAG Atlantic-1 UNITED TEA-2 TPE FEA UNITED STATES LATVIA APG NCP MOC ASE KINGDOM DENMARK TEA-2 TEA-2 Apollo TEA-2 EAC-C2C Manasquan, NJ APCN-2 AJC TEA-2 JIH TAT-14 LITHUANIA Moscow SeaMeWe-3 TEA SJC2 [2020] EAC-C2C SJC TEA-3 TEA-3 FLAG/REACH NAL FLAG/REACH NAL Northport, NY FLAG Atlantic-1 EAC-C2C Okinawa BELARUS TEA TEA GTT-Atlantic NETH. -

PUBLIC NOTICE FEDERAL COMMUNICATIONS COMMISSION 445 12Th STREET S.W
PUBLIC NOTICE FEDERAL COMMUNICATIONS COMMISSION 445 12th STREET S.W. WASHINGTON D.C. 20554 News media information 202-418-0500 Internet: http://www.fcc.gov (or ftp.fcc.gov) TTY (202) 418-2555 Report No. SCL-00141NS Monday June 17, 2013 Non-Streamlined Submarine Cable Landing License Applications Accepted For Filing Unless otherwise specified, the following procedures apply to the applications listed below: The applications listed below have been found, upon initial review, to be acceptable for filing. These applications are not subject to the streamlined processing procedures set forth in Section 1.767 of the Commission’s rules, 47 C.F.R. § 1.767. Unless otherwise specified, interested parties may file comments with respect to these applications within 28 days of the date of this public notice. We request that such comments refer to the application file number shown below. Unless otherwise specified, ex parte communications between outside parties and Commission staff concerning these applications are permitted subject to the Commission’s rules for “permit-but-disclose proceedings.” See 47 C.F.R. § 1.1206. Copies of all applications listed here are available for public inspection in the FCC Reference and Information Center, located in room CY-A257 at the Portals 2 building, 445 12th Street SW, Washington DC 20554. The center can be contacted at (202) 418-0270. People with Disabilities: To request materials in accessible formats for people with disabilities (braille, large print, electronic files, audio format), send an e-mail to [email protected] or call the Consumer & Governmental Affairs Bureau at 202-418-0530 (voice), 202-418-0432 (tty). -

Before the FEDERAL COMMUNICATIONS COMMISSION
Before the FEDERAL COMMUNICATIONS COMMISSION In the Matter of ) ) The Americas I Submarine Cable System ) File No. SCL-LIC-19921110-00002 Operating Between the United States ) Mainland and St. Thomas in the U.S. Virgin ) Islands APPLICATION FOR CABLE LANDING LICENSE The Americas I Consortium, pursuant to 47 U.S.C. §§ 34-39, Executive Order 10,530, and 47 C.F.R. § 1.767, hereby applies for a cable landing license for the Americas I Cable System to allow the continued operation of this domestic submarine cable for an additional 25- 1 year term following the expiration of the existing cable landing license on September 1, 2019. The Americas I Cable System links the U.S. Mainland with the U.S. Virgin Islands and connects to other cables serving other Caribbean islands and Central and South America. The cable has operated successfully for 24 years pursuant to the cable landing license granted in 1992, has been upgraded six times between 2009 and 2018, currently provides more than 430 Gbps of available capacity, and has a design capacity of 800 Gbps. The continued operation of this cable will serve customers in the United States by providing bandwidth capacity for broadband traffic between the U.S. Mainland and the U.S. Virgin Islands with connections to 1 The Americas I Cable System commenced operation on September 1, 1994, pursuant to its original cable landing license granted on July 13, 1993. See American Telephone & Telegraph Company, et al., 8 FCC. Rcd. 5041 (1993). The international segments of Americas I were retired in June 2009. -

Pan American Files at Richter Library
ASM0341 PAN AMERICAN WORLD AIRWAYS, INC RECORDS CONTAINER LIST INSTRUCTIONS The Pan American World Airways, Inc. Records are organized into two accessions, with individual numbering systems. This means that there is a box 1 from Accession I, and a box 1 from Accession II. Be sure to note the accession number along with the box number in your requests. TABLE OF CONTENTS Pan American World Airways, Inc. Accession I (box 1 – 656)…………………………………………………. 2– 444 Pan American World Airways, Inc. Accession II (box 1 – 960)………………………………………………… 445 – 938 1 Special Collections, University of Miami Libraries ASM0341 Pan American World Airways, Inc. Records Container List Accession I (Brockway) Box Folder 1 1-5 First flight: General 1977-81 6 First flight: from San Francisco to Shanghai and Beijing via Tokyo 1981 7 First flight: (1986 not in box) 1982-83 8-13 First flight 1983-87 14 First Airbus flight: New York to Barbados 1984 15 Forty fifth Anniversary: First airmail passenger 1984 16 First day covers: China 1980-81 17 Proving flight to Beijing, China 1980 18 San Francisco/Los Angeles/Rio, and Johannesburg 1978 19 Special flight (charter) Boston Symphony/ Boston and Anchorage 1979 20 Survey flight to Canton, China from Hong Kong 1979 21 Round the World 1929 22 50th Anniversary Round the World Flight over the North and South Poles 1977 23 Houston/Mexico City added to Round the World flight 1978 24 Round the World Service: Mexico City/Houston/Washington/New York/London/Frankfurt 1978 25 Round the World flight: Film undated 26 Speed Records: Round the