Dissertation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Our Arctic Nation a U.S
Connecting the United States to the Arctic OUR ARCTIC NATION A U.S. Arctic Council Chairmanship Initiative Cover Photo: Cover Photo: Hosting Arctic Council meetings during the U.S. Chairmanship gave the United States an opportunity to share the beauty of America’s Arctic state, Alaska—including this glacier ice cave near Juneau—with thousands of international visitors. Photo: David Lienemann, www. davidlienemann.com OUR ARCTIC NATION Connecting the United States to the Arctic A U.S. Arctic Council Chairmanship Initiative TABLE OF CONTENTS 01 Alabama . .2 14 Illinois . 32 02 Alaska . .4 15 Indiana . 34 03 Arizona. 10 16 Iowa . 36 04 Arkansas . 12 17 Kansas . 38 05 California. 14 18 Kentucky . 40 06 Colorado . 16 19 Louisiana. 42 07 Connecticut. 18 20 Maine . 44 08 Delaware . 20 21 Maryland. 46 09 District of Columbia . 22 22 Massachusetts . 48 10 Florida . 24 23 Michigan . 50 11 Georgia. 26 24 Minnesota . 52 12 Hawai‘i. 28 25 Mississippi . 54 Glacier Bay National Park, Alaska. Photo: iStock.com 13 Idaho . 30 26 Missouri . 56 27 Montana . 58 40 Rhode Island . 84 28 Nebraska . 60 41 South Carolina . 86 29 Nevada. 62 42 South Dakota . 88 30 New Hampshire . 64 43 Tennessee . 90 31 New Jersey . 66 44 Texas. 92 32 New Mexico . 68 45 Utah . 94 33 New York . 70 46 Vermont . 96 34 North Carolina . 72 47 Virginia . 98 35 North Dakota . 74 48 Washington. .100 36 Ohio . 76 49 West Virginia . .102 37 Oklahoma . 78 50 Wisconsin . .104 38 Oregon. 80 51 Wyoming. .106 39 Pennsylvania . 82 WHAT DOES IT MEAN TO BE AN ARCTIC NATION? oday, the Arctic region commands the world’s attention as never before. -

Sampling Adults by Animal Bait Catches and by Animal-Baited Traps
Chapter 5 Sampling Adults by Animal Bait Catches and by Animal-Baited Traps The most fundamental method for catching female mosquitoes is to use a suit able bait to attract hungry host-seeking individuals, and human bait catches, sometimes euphemistically called landing counts, have been used for many years to collect anthropophagic species. Variations on the simple direct bait catch have included enclosing human or bait animals in nets, cages or traps which, in theory at least, permit the entrance of mosquitoes but prevent their escape. Other attractants, the most widely used of which are light and carbon dioxide, have also been developed for catching mosquitoes. In some areas, especially in North America, light-traps, with or without carbon dioxide as a supplement, have more or less replaced human and animal baits as a routine sampling method for several species (Chapter 6). However, despite intensive studies on host-seeking behaviour no really effective attractant has been found to replace a natural host, and consequently human bait catches remain the most useful single method of collecting anthropophagic mosquitoes. Moreover, although bait catches are not completely free from sampling bias they are usually more so than most other collecting methods that employ an attractant. They are also easily performed and require no complicated or expensive equipment. HUMAN BAIT CATCHES Attraction to hosts Compounds used by mosquitoes to locate their hosts are known as kairomones, that is substances from the emitters (hosts) are favourable to the receiver (mosquitoes) but not to themselves. Emanations from hosts include heat, water vapour, carbon dioxide and various host odours. -

Regional Concerns During the Age of Imperialism. Marshall E
Louisiana State University LSU Digital Commons LSU Historical Dissertations and Theses Graduate School 1995 The outhS and American Foreign Policy, 1894-1904: Regional Concerns During the Age of Imperialism. Marshall E. Schott Louisiana State University and Agricultural & Mechanical College Follow this and additional works at: https://digitalcommons.lsu.edu/gradschool_disstheses Recommended Citation Schott, Marshall E., "The outhS and American Foreign Policy, 1894-1904: Regional Concerns During the Age of Imperialism." (1995). LSU Historical Dissertations and Theses. 6134. https://digitalcommons.lsu.edu/gradschool_disstheses/6134 This Dissertation is brought to you for free and open access by the Graduate School at LSU Digital Commons. It has been accepted for inclusion in LSU Historical Dissertations and Theses by an authorized administrator of LSU Digital Commons. For more information, please contact [email protected]. INFORMATION TO USERS This manuscript has been reproduced from the microfilm master.UMI films the text directly from the original or copy submitted. Thus, some thesis and dissertation copies are in typewriter face, while others may be from any type of computer printer. The quality of this reproduction is dependent upon the quality of the copy submitted. Broken or indistinct print, colored or poor quality illustrations and photographs, print bleedthrough, substandard margins, and improper alignment can adversely afreet reproduction. In the unlikely event that the author did not send UMI a complete manuscript and there are missing pages, these will be noted. Also, if unauthorized copyright material had to be removed, a note will indicate the deletion. Oversize materials (e.g., maps, drawings, charts) are reproduced by sectioning the original, beginning at the upper left-hand comer and continuing from left to right in equal sections with small overlaps. -

Congressional Record-House. April 24
5476 CONGRESSIONAL RECORD-HOUSE. APRIL 24, By Mr. WILSON of lllinois: A bill (H. R. 15397) granting a. HOUSE OF REPRESENTATIVES. pension to Carl Traver-to the Committee on Invalid Pensions. Also, a bill (H. R. 15398) to remove the charge of desertion from SUNDAY, .April24, 190.4-. the military record of GeorgeS. Green-to the Committee on Mil The House met at 12 o'clock m. itary Affairs. The following prayer was offered by the Chaplain, Rev. H.E..--rn.Y N. COUDEN, D. D.: PETITIONS, ETC. Eternal and everliving God, our Heavenly Father, we thank Thee for that deep and ever-abiding faith which Thou hast im Under clause 1 of Rn1e XXII, the following petitions and papers planted in the hearts of men, and which has inspired the true, the were laid on the Clerk's desk and referred as follows: noble, the brave of every age with patriotic zeal and fervor, bring By Mr. BRADLEY: Petition of Montgomery Grange, of Mont gomery, N.Y., and others, in favor of the passage of bill H. R. ing light out of darkness, order out of chaos, liberty out of bond 9302-to the Committee on Ways and Means. age, and thus contributing here a. little, there a. little, to the By Mr. CALDERHEAD: Petition of Lamar Methodist Episco splendid civilization of our age. Especially do we thank Thee for pal Church, of Lamar Kans., in favor of the Hepburn-Dolliver that long line of illustrious men who lived and wrought, suffered bill-to the Committee on the Judiciary. -

Hamilton's Forgotten Epidemics
Library and Archives Canada Cataloguing in Publication Ch2olera: Hamilton’s Forgotten Epidemics / D. Ann Herring and Heather T. Battles, editors. Includes bibliographical references and index. ISBN 978-0-9782417-4-2 Print catalogue data is available from Library and Archives Canada, at www.collectionscanada.gc.ca Cover Image: Historical City of Hamilton. Published by Rice & Duncan in 1859, drawn by G. Rice. http://map.hamilton.ca/old hamilton.jpg Cover Design: Robert Huang Group Photo: Temara Brown Ch2olera Hamilton’s Forgotten Epidemics D. Ann Herring and Heather T. Battles, editors DEPARTMENT OF ANTHROPOLOGY McMASTER UNIVERSITY Hamilton, Ontario, Canada Contents FIGURES AND TABLES vii Introduction Ch2olera: Hamilton’s Forgotten Epidemics D. Ann Herring and Heather T. Battles 2 2 “From Time Immemorial”: British Imperialism and Cholera in India Diedre Beintema 8 3 Miasma Theory and Medical Paradigms: Shift Happens? Ayla Mykytey 18 4 ‘A Rose by Any Other Name’: Types of Cholera in the 19th Century Thomas Siek 24 5 Doesn’t Anyone Care About the Children? Katlyn Ferrusi 32 6 Changing Waves: The Epidemics of 1832 and 1854 Brianna K. Johns 42 7 Charcoal, Lard, and Maple Sugar: Treating Cholera in the 19th Century S. Lawrence-Nametka 52 iii 8 How Disease Instills Fear into a Population Jacqueline Le 62 9 The Blame Game Andrew Turner 72 10 Virulence Victims in Victorian Hamilton Jodi E. Smillie 80 11 On the Edge of Death: Cholera’s Impact on Surrounding Towns and Hamlets Mackenzie Armstrong 90 12 Avoid Cholera: Practice Cleanliness and Temperance Karolina Grzeszczuk 100 13 New Rules to Battle the Cholera Outbreak Alexandra Saly 108 14 Sanitation in Early Hamilton Nathan G. -
Haitian Migration and Danced Identity in Eastern Cuba
Haitian Migration and Danced Identity in Eastern Cuba The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters Citation Viddal, Grete. 2010. Haitian migration and danced identity in eastern Cuba. In Making Caribbean Dance: Continuity and Creativity in Island Cultures, ed. Susanna Sloat, 83-94. Gainesville, FL: University Press of Florida. Published Version doi:10.5744/florida/9780813034676.003.0007 Citable link http://nrs.harvard.edu/urn-3:HUL.InstRepos:10384888 Terms of Use This article was downloaded from Harvard University’s DASH repository, and is made available under the terms and conditions applicable to Other Posted Material, as set forth at http:// nrs.harvard.edu/urn-3:HUL.InstRepos:dash.current.terms-of- use#LAA 7 Haitian Migration and Danced Identity in Eastern Cuba Grete Viddal I arrive at Santiago de Cuba’s Teatro Oriente to see a small crowd of locals and tourists waiting outside. We are here to see Ballet Folklórico Cutumba, one of eastern Cuba’s premier folkloric dance troupes. Although the theater is run down and no longer has electricity or running water, its former el- egance is apparent. As we enter, we see that lush but tattered velvet drapes flank the stage and ornate architectural details adorn the walls underneath faded and peeling paint. Light filters in through high windows. As the per- formance starts, women in elaborate ball gowns enter this dusty stage. They must hold up their voluminous skirts to keep yards of fabric from drag- ging on the floor. Men sport white topcoats with tails and matching white cravats. -

Theobald 1903 1.Pdf
A MONOGRAPH OFTHE CULICIDAE OF THE WORLD. GENERAL NOTES. Several notes of general interest have been made and sent by correspondents that can scarcely be incorporated in the systematic part of this book. These are presented here. THE RELATIVEFREQUENCE OF CULICINAAND ANOPHELINA. It is interesting to note the relative frequence of these two sections of the CFulicidae. In most cases observations made personally during the past two years show that in Great Rritain the Anophelina, where they occur at all, are relatively more abundant in habitations than Culex. At Great Staughton during August the numbers counted in a privy in the morning were as follows during the week ending the 26th :-- 20th . 10 AM. Culex 12 ; Anopheles 37 21st . ,) . Culex 20; Anopheles 15 22nd . Culex 7 : Anopheles 40 23rd . ,; Culex 12; Anoiheles 17 24th . ,, :: Culex 2 ; Anopheles 7 25th . ,, . Culex 30; Anopheles 14 26th . ), .* Culex 8; Anopheles 27 eThe species were Cu1e.x pipi3iens and Anopheles mncuLpennk’ At Wye, again, observations were made during August, VOL. III. B September and October, again in a privy and also in a bed- room. AUGUST. Between In privy. In beihoom 12th . ~&~OA.IVI. Culex 4; Anopheles 6 . Culex 2 ; Anopheles 5 13th . ,, . Culex 1; Anbpheles 8 . Culex 1; Anopheles 6 14th . ,, . Culex 7;‘ Anopheles 15 . Culex 1; Anopheles 3 15th . ,, . Culex 3; Anopheles 3 . Culex 5; Anopheles 12 16th . ,, . Culex 7 ; Anopheles 12 . Culex 8 ; Anopheles 12 17th . ,, . Culex 9 ; Anopheles 8 . Culex 2 ; Anopheles 9 18th . ,, ., Culex 1; Anopheles 4 . Culex 3 ; Anopheles 4 SEPTEI+IBER. In prhy. In bedroom. 3rd . Culex 12 ; Anopheles 3 . -

Historia Naval
REVISTA DE HISTORIA NAVAL Ao XVI Núm. 63 INSTITUTO DE HISTORIA Y CULTURA NAVAL ARMADA ESPAÑOLA INSTITUTO DE HISTORIA Y CULTURA NAVAL ARMADA ESPAÑOLA REVISTA DE HISTORIA NAVAL Año XVI 1998 Núm. 63 REVISTA DE HISTORIA NAVAL CONSEJO RECTOR: Presidente: Director del Instituto de Historia y Cultura Naval, José Ignacio González-Aller Hierro, contralmirante. Vicepresidente y Director: JoséCervera Pery, general auditor. Periodista. Vocales: Fernando de la Guardia Salvetti, Secretario General del Instituto de Historia y Cultura Naval; Rafaél Estrada Giménez, Jefe del Departa mento de Cultura del Instituto de Historia y Cultura Naval; Hugo O’Donnell y Duque de Estrada, de la Comisión Española de Historia Marítima; Enrique Martínez Ruiz, Catedrático de Historia de la Universidad Complutense de Madrid. Redacción, Difusión y Distribución: Isabel Hernández Sanz, Ana Berenguer Berenguer. Administración: Manuel Pérez García, comandante de Intendencia de la Armada. DIRECCIÓN y ADMINISTRACIÓN: Instituto de Historia y Cultura Naval Juan de Mena, 1, 1.’ planta. 28071 Madrid (España). Teléfono: 91 379 5000 Fax: 91 379 59 45 EDICIÓN DEL MINISTERIO DE DEFENSA IMPRIME: Servicio de Publicaciones de la Armada. Publicación trimestral: cuarto trimestre 1998. Precio del éjemplar suelto: 650 pesetas. Suscripción anual: España y Portugal: 2.600 pesetas. Resto del mundo: 4.000 pesetas. Depósito legal: M. 16.854-1983. ISSN-0212-467X. NIPO: 076-98-007-2 Impreso en España. - Printed in Spain. CUBIERTA ANTERIOR: Logotipo del Instituto de Historia y Cultura Naval. CUBIERTA POSTERIOR: Del libro Regimiento de Navegación, de Pedro de Medina. Sevilla, 1563. SUMARIO Págs. NOTA EDITORIAL . Reflexiones finales de un centenario, por José Cervera Pery7 Los libros del 98: una aproximación reflexiva, por Belén Fernández15 Un héroe de Filipinas: Ambrosio Ristori, «El manco de Bacoor», por Manuel Ristori Peláez23 La acción. -

Exile, Diplomacy and Texts: Exchanges Between Iberia and the British Isles, 1500–1767
Exile, Diplomacy and Texts Intersections Interdisciplinary Studies in Early Modern Culture General Editor Karl A.E. Enenkel (Chair of Medieval and Neo-Latin Literature Westfälische Wilhelms-Universität Münster e-mail: kenen_01@uni_muenster.de) Editorial Board W. van Anrooij (University of Leiden) W. de Boer (Miami University) Chr. Göttler (University of Bern) J.L. de Jong (University of Groningen) W.S. Melion (Emory University) R. Seidel (Goethe University Frankfurt am Main) P.J. Smith (University of Leiden) J. Thompson (Queen’s University Belfast) A. Traninger (Freie Universität Berlin) C. Zittel (Ca’ Foscari University of Venice / University of Stuttgart) C. Zwierlein (Freie Universität Berlin) volume 74 – 2021 The titles published in this series are listed at brill.com/inte Exile, Diplomacy and Texts Exchanges between Iberia and the British Isles, 1500–1767 Edited by Ana Sáez-Hidalgo Berta Cano-Echevarría LEIDEN | BOSTON This is an open access title distributed under the terms of the CC BY-NC-ND 4.0 license, which permits any non-commercial use, distribution, and reproduction in any medium, provided no alterations are made and the original author(s) and source are credited. Further information and the complete license text can be found at https://creativecommons.org/licenses/by-nc-nd/4.0/ The terms of the CC license apply only to the original material. The use of material from other sources (indicated by a reference) such as diagrams, illustrations, photos and text samples may require further permission from the respective copyright holder. This volume has been benefited from financial support of the research project “Exilio, diplomacia y transmisión textual: Redes de intercambio entre la Península Ibérica y las Islas Británicas en la Edad Moderna,” from the Agencia Estatal de Investigación, the Spanish Research Agency (Ministerio de Economía y Competitividad). -

Race and Inequality in Cuban Tourism During the 21St Century
California State University, San Bernardino CSUSB ScholarWorks Electronic Theses, Projects, and Dissertations Office of aduateGr Studies 6-2015 Race and Inequality in Cuban Tourism During the 21st Century Arah M. Parker California State University - San Bernardino Follow this and additional works at: https://scholarworks.lib.csusb.edu/etd Part of the Politics and Social Change Commons, Race and Ethnicity Commons, Social and Cultural Anthropology Commons, and the Tourism Commons Recommended Citation Parker, Arah M., "Race and Inequality in Cuban Tourism During the 21st Century" (2015). Electronic Theses, Projects, and Dissertations. 194. https://scholarworks.lib.csusb.edu/etd/194 This Thesis is brought to you for free and open access by the Office of aduateGr Studies at CSUSB ScholarWorks. It has been accepted for inclusion in Electronic Theses, Projects, and Dissertations by an authorized administrator of CSUSB ScholarWorks. For more information, please contact [email protected]. RACE AND INEQUALITY IN CUBAN TOURISM DURING THE 21 ST CENTURY A Thesis Presented to the Faculty of California State University, San Bernardino In Partial Fulfillment of the Requirements for the Degree Master of Arts in Social Sciences by Arah Marie Parker June 2015 RACE AND INEQUALITY IN CUBAN TOURISM DURING THE 21 ST CENTURY A Thesis Presented to the Faculty of California State University, San Bernardino by Arah Marie Parker June 2015 Approved by: Dr. Teresa Velasquez, Committee Chair, Anthropology Dr. James Fenelon, Committee Member Dr. Cherstin Lyon, Committee Member © 2015 Arah Marie Parker ABSTRACT As the largest island in the Caribbean, Cuba boasts beautiful scenery, as well as a rich and diverse culture. -
Highlights Situation Overview
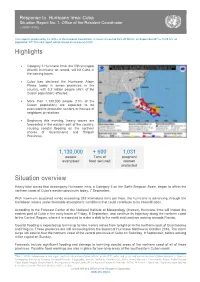
Response to Hurricane Irma: Cuba Situation Report No. 1. Office of the Resident Coordinator ( 07/09/ 20176) This report is produced by the Office of the Resident Coordinator. It covers the period from 20:00 hrs. on September 06th to 14:00 hrs. on September 07th.The next report will be issued on or around 08/09. Highlights Category 5 Hurricane Irma, the fifth strongest Atlantic hurricane on record, will hit Cuba in the coming hours. Cuba has declared the Hurricane Alarm Phase today in seven provinces in the country, with 5.2 million people (46% of the Cuban population) affected. More than 1,130,000 people (10% of the Cuban population) are expected to be evacuated to protection centers or houses of neighbors or relatives. Beginning this evening, heavy waves are forecasted in the eastern part of the country, causing coastal flooding on the northern shores of Guantánamo and Holguín Provinces. 1,130,000 + 600 1,031 people Tons of pregnant evacuated food secured women protected Situation overview Heavy tidal waves that accompany Hurricane Irma, a Category 5 on the Saffir-Simpson Scale, began to affect the northern coast of Cuba’s eastern provinces today, 7 September. With maximum sustained winds exceeding 252 kilometers (km) per hour, the hurricane is advancing through the Caribbean waters under favorable atmospheric conditions that could contribute to its intensification. According to the Forecast Center of the National Institute of Meteorology (Insmet), Hurricane Irma will impact the eastern part of Cuba in the early hours of Friday, 8 September, and continue its trajectory along the northern coast to the Central Region, where it is expected to make a shift to the north and continue moving towards Florida. -

Proposed Wisconsin – Lake Michigan National Marine Sanctuary
Proposed Wisconsin – Lake Michigan National Marine Sanctuary Draft Environmental Impact Statement and Draft Management Plan DECEMBER 2016 | sanctuaries.noaa.gov/wisconsin/ National Oceanic and Atmospheric Administration (NOAA) U.S. Secretary of Commerce Penny Pritzker Under Secretary of Commerce for Oceans and Atmosphere and NOAA Administrator Kathryn D. Sullivan, Ph.D. Assistant Administrator for Ocean Services and Coastal Zone Management National Ocean Service W. Russell Callender, Ph.D. Office of National Marine Sanctuaries John Armor, Director Matt Brookhart, Acting Deputy Director Cover Photos: Top: The schooner Walter B. Allen. Credit: Tamara Thomsen, Wisconsin Historical Society. Bottom: Photomosaic of the schooner Walter B. Allen. Credit: Woods Hole Oceanographic Institution - Advanced Imaging and Visualization Laboratory. 1 Abstract In accordance with the National Environmental Policy Act (NEPA, 42 U.S.C. 4321 et seq.) and the National Marine Sanctuaries Act (NMSA, 16 U.S.C. 1434 et seq.), the National Oceanic and Atmospheric Administration’s (NOAA) Office of National Marine Sanctuaries (ONMS) has prepared a Draft Environmental Impact Statement (DEIS) that considers alternatives for the proposed designation of Wisconsin - Lake Michigan as a National Marine Sanctuary. The proposed action addresses NOAA’s responsibilities under the NMSA to identify, designate, and protect areas of the marine and Great Lakes environment with special national significance due to their conservation, recreational, ecological, historical, scientific, cultural, archaeological, educational, or aesthetic qualities as national marine sanctuaries. ONMS has developed five alternatives for the designation, and the DEIS evaluates the environmental consequences of each under NEPA. The DEIS also serves as a resource assessment under the NMSA, documenting present and potential uses of the areas considered in the alternatives.