Bromethalin Ingestion
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Veterinary Toxicology
GINTARAS DAUNORAS VETERINARY TOXICOLOGY Lecture notes and classes works Study kit for LUHS Veterinary Faculty Foreign Students LSMU LEIDYBOS NAMAI, KAUNAS 2012 Lietuvos sveikatos moksl ų universitetas Veterinarijos akademija Neužkre čiam ųjų lig ų katedra Gintaras Daunoras VETERINARIN Ė TOKSIKOLOGIJA Paskait ų konspektai ir praktikos darb ų aprašai Mokomoji knyga LSMU Veterinarijos fakulteto užsienio studentams LSMU LEIDYBOS NAMAI, KAUNAS 2012 UDK Dau Apsvarstyta: LSMU VA Veterinarijos fakulteto Neužkre čiam ųjų lig ų katedros pos ėdyje, 2012 m. rugs ėjo 20 d., protokolo Nr. 01 LSMU VA Veterinarijos fakulteto tarybos pos ėdyje, 2012 m. rugs ėjo 28 d., protokolo Nr. 08 Recenzavo: doc. dr. Alius Pockevi čius LSMU VA Užkre čiam ųjų lig ų katedra dr. Aidas Grigonis LSMU VA Neužkre čiam ųjų lig ų katedra CONTENTS Introduction ……………………………………………………………………………………… 7 SECTION I. Lecture notes ………………………………………………………………………. 8 1. GENERAL VETERINARY TOXICOLOGY ……….……………………………………….. 8 1.1. Veterinary toxicology aims and tasks ……………………………………………………... 8 1.2. EC and Lithuanian legal documents for hazardous substances and pollution ……………. 11 1.3. Classification of poisons ……………………………………………………………………. 12 1.4. Chemicals classification and labelling ……………………………………………………… 14 2. Toxicokinetics ………………………………………………………………………...………. 15 2.2. Migration of substances through biological membranes …………………………………… 15 2.3. ADME notion ………………………………………………………………………………. 15 2.4. Possibilities of poisons entering into an animal body and methods of absorption ……… 16 2.5. Poison distribution -

The Veterinarian's Guide
The Veterinarian’s Guide Bromethalin Addendum The Soft Bait Innovators™ Liphatech, Inc. • 3600 W. Elm Street • Milwaukee, WI 53209 • 1-888-331-7900 • www.liphatech.com NOTE: The information in this guide does not represent labeling and does not replace information on rodenticide labels relating to exposure of non-target species. Please read and follow all label directions on all rodenticide products you are using. Mentions of trade names in this publication does not imply endorsement of these products. Assault® is a registered trademark of PM Resources (St. Louis, MO) TakeDown™ and Cannon™ are trademarks of Liphatech, Inc. (Milwaukee, WI) Gunslinger® is a registered trademark of Liphatech, Inc. (Milwaukee, WI) Fastrac® is a registered trademark of Bell Labs (Madison, WI) Top Gun™ is a trademark of JT Eaton (Twinsburg, OH) Tomcat® and Rampage® are registered trademarks of Motomco (Madison, WI) Trounce® is a registered trademark of Agricultural Feeds (St. Louis, MO) At the time of this printing all information was deemed accurate and reliable. Liphatech, Inc. 3600 W. Elm Street Milwaukee, WI 53209 1-888-331-7900 www.liphatech.com October, 2016 The Veterinarian’s Guide - Bromethalin Addendum The Veterinarian’s Guide to Accidental Rodenticide Ingestion by Dogs and Cats focuses on anticoagulants. This addendum is intended to help veterinarians recognize and treat the symptoms of bromethalin toxicity in domestic animals. It describes bromethalin’s mode of action and how it is used as a rodenticide. In addition to reviewing the symptoms of bromethalin poisoning in domestic animals and the acute toxicity levels for dogs and cats (Table 5), we have also included the American Society for Prevention of Cruelty to Animals’ Animal Poison Control Center (ASPCA APCC) recommendations for decontamination (Tables 6 and 7). -

RRAC Guidelines on Anticoagulant Rodenticide Resistance Management Editor: Rodenticide Resistance Action Committee (RRAC) of Croplife International Aim
RRAC guidelines on Anticoagulant Rodenticide Resistance Management Editor: Rodenticide Resistance Action Committee (RRAC) of CropLife International Aim This document provides guidance to advisors, national authorities, professionals, practitioners and others on the nature of anticoagulant resistance in rodents, the identification of anticoagulant resistance, strategies for rodenticide application that will avoid the development of resistance and the management of resistance where it occurs. The Rodenticide Resistance Action Committee (RRAC) is a working group within the framework of CropLife International. Participating companies include: Bayer CropScience, BASF, LiphaTech S. A., PelGar, Rentokil Initial, Syngenta and Zapi. Senior technical specialists, with specific expertise in rodenticides, represent their companies on this committee. The RRAC is grateful to the following co-authors: Stefan Endepols, Alan Buckle, Charlie Eason, Hans-Joachim Pelz, Adrian Meyer, Philippe Berny, Kristof Baert and Colin Prescott. Photos provided by Stefan Endepols. Contents 1. Introduction ............................................................................................................................................................................................................. 2 2. Classification and history of rodenticide compounds ..............................................................................................3 3. Mode of action of anticoagulant rodenticides, resistance mechanisms, and resistance mutations ......................................................................................................6 -

Question of the Day Archives: Monday, December 5, 2016 Question: Calcium Oxalate Is a Widespread Toxin Found in Many Species of Plants
Question Of the Day Archives: Monday, December 5, 2016 Question: Calcium oxalate is a widespread toxin found in many species of plants. What is the needle shaped crystal containing calcium oxalate called and what is the compilation of these structures known as? Answer: The needle shaped plant-based crystals containing calcium oxalate are known as raphides. A compilation of raphides forms the structure known as an idioblast. (Lim CS et al. Atlas of select poisonous plants and mushrooms. 2016 Disease-a-Month 62(3):37-66) Friday, December 2, 2016 Question: Which oral chelating agent has been reported to cause transient increases in plasma ALT activity in some patients as well as rare instances of mucocutaneous skin reactions? Answer: Orally administered dimercaptosuccinic acid (DMSA) has been reported to cause transient increases in ALT activity as well as rare instances of mucocutaneous skin reactions. (Bradberry S et al. Use of oral dimercaptosuccinic acid (succimer) in adult patients with inorganic lead poisoning. 2009 Q J Med 102:721-732) Thursday, December 1, 2016 Question: What is Clioquinol and why was it withdrawn from the market during the 1970s? Answer: According to the cited reference, “Between the 1950s and 1970s Clioquinol was used to treat and prevent intestinal parasitic disease [intestinal amebiasis].” “In the early 1970s Clioquinol was withdrawn from the market as an oral agent due to an association with sub-acute myelo-optic neuropathy (SMON) in Japanese patients. SMON is a syndrome that involves sensory and motor disturbances in the lower limbs as well as visual changes that are due to symmetrical demyelination of the lateral and posterior funiculi of the spinal cord, optic nerve, and peripheral nerves. -

Recommended Classification of Pesticides by Hazard and Guidelines to Classification 2019 Theinternational Programme on Chemical Safety (IPCS) Was Established in 1980
The WHO Recommended Classi cation of Pesticides by Hazard and Guidelines to Classi cation 2019 cation Hazard of Pesticides by and Guidelines to Classi The WHO Recommended Classi The WHO Recommended Classi cation of Pesticides by Hazard and Guidelines to Classi cation 2019 The WHO Recommended Classification of Pesticides by Hazard and Guidelines to Classification 2019 TheInternational Programme on Chemical Safety (IPCS) was established in 1980. The overall objectives of the IPCS are to establish the scientific basis for assessment of the risk to human health and the environment from exposure to chemicals, through international peer review processes, as a prerequisite for the promotion of chemical safety, and to provide technical assistance in strengthening national capacities for the sound management of chemicals. This publication was developed in the IOMC context. The contents do not necessarily reflect the views or stated policies of individual IOMC Participating Organizations. The Inter-Organization Programme for the Sound Management of Chemicals (IOMC) was established in 1995 following recommendations made by the 1992 UN Conference on Environment and Development to strengthen cooperation and increase international coordination in the field of chemical safety. The Participating Organizations are: FAO, ILO, UNDP, UNEP, UNIDO, UNITAR, WHO, World Bank and OECD. The purpose of the IOMC is to promote coordination of the policies and activities pursued by the Participating Organizations, jointly or separately, to achieve the sound management of chemicals in relation to human health and the environment. WHO recommended classification of pesticides by hazard and guidelines to classification, 2019 edition ISBN 978-92-4-000566-2 (electronic version) ISBN 978-92-4-000567-9 (print version) ISSN 1684-1042 © World Health Organization 2020 Some rights reserved. -

The 10 Most Common Toxicoses in Dogs
Toxicology Brief managing common poisonings in companion animals PEER-REVIEWED The 10 most common toxicoses in dogs Irina Meadows, DVM, and Sharon Gwaltney-Brant DVM, PhD ogs are usually exposed to potentially toxic house- Chocolate hold products and medications accidentally. But 2 Chocolate contains two types of Dsometimes well-intentioned owners unknowingly methylxanthine, theobromine and caf- give their dogs harmful products and medications. To help feine, with their amounts varying de- prepare you for patients with theses toxicoses, we com- pending on the type of chocolate. For piled this list of the 10 most common hazards to dogs, example, milk chocolate contains about based on the number of calls we have received at the 60 mg/oz methylxanthine, dark chocolate about 150 mg/oz, ASPCA Animal Poison Control Center (APCC) between 2001 and baking chocolate about 450 mg/oz.3 and 2005.1 Clinical signs of chocolate ingestion range from GI upset to cardiovascular effects (e.g. tachycardia, hypertension or hy- Ibuprofen potension, arrhythmias) to CNS signs (e.g. agitation, pacing, hy- 1 Ibuprofen, a nonsteroidal anti- peractivity, tremors, seizures). The toxicity depends on the inflammatory drug with analgesic, anti- type of chocolate, the amount ingested, the size of the animal, inflammatory, and antipyretic effects,2 is and the animal’s sensitivity to methylxanthines. Mild stimula- available in a variety of strengths. The tion such as hyperactivity, agitation, and restlessness may most common over-the-counter occur in dogs ingesting around 20 mg/kg methylxanthine. strength is 200 mg, but the prescription-strength tablets can Cardiotoxicosis may occur in dogs ingesting 40 mg/kg, and contain up to 800 mg ibuprofen. -
Managing Pesticide Poisoning Risk and Understanding the Signs and Symptoms Clyde L
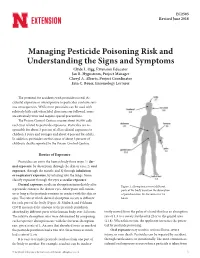
EC2505 Revised June 2018 Managing Pesticide Poisoning Risk and Understanding the Signs and Symptoms Clyde L. Ogg, Extension Educator Jan R. Hygnstrom, Project Manager Cheryl A. Alberts, Project Coordinator Erin C. Bauer, Entomology Lecturer The potential for accidents with pesticides is real. Ac- cidental exposure or overexposure to pesticides can have seri- ous consequences. While most pesticides can be used with relatively little risk when label directions are followed, some are extremely toxic and require special precautions. The Poison Control Centers receive about 90,000 calls each year related to pesticide exposures. Pesticides are re- sponsible for about 3 percent of all accidental exposures to children 5 years and younger and about 4 percent for adults. In addition, pesticides are the cause of about 3 percent of children’s deaths reported to the Poison Control Centers. Routes of Exposure Pesticides can enter the human body three ways: 1) der- mal exposure, by absorption through the skin or eyes; 2) oral exposure, through the mouth; and 3) through inhalation or respiratory exposure, by inhaling into the lungs. Some classify exposure through the eyes as ocular exposure. Dermal exposure results in absorption immediately after Figure 1. Absorption rates of different a pesticide contacts the skin or eyes. Absorption will contin- parts of the body based on the absorption ue as long as the pesticide remains in contact with the skin or of parathion into the forearm over 24 eyes. The rate at which dermal absorption occurs is different hours. for each part of the body (Figure 1). Maiback and Feldman (1974) measured the amount of the pesticide parathion absorbed by different parts of the human body over 24 hours. -

(12) Patent Application Publication (10) Pub. No.: US 2014/0271932 A1 Rubel Et Al
US 2014027 1932A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2014/0271932 A1 Rubel et al. (43) Pub. Date: Sep. 18, 2014 (54) RODENTICIDAL COMPOSITION AND Publication Classification METHOD (51) Int. Cl. (71) Applicant: PIC Corporation/Pest Free Living, AOIN 59/00 (2006.01) Linden, NJ (US) (52) U.S. Cl. CPC ...................................... A0IN 59/00 (2013.01) (72) Inventors: Phyllis Rubel, Scotch Plains, NJ (US); USPC .......................................................... 424/717 Sidney Goldman, Verona, NJ (US); Bogdan Enache, Jersey City, NJ (US) (57) ABSTRACT A rodenticidal composition comprising a carbon dioxide (21) Appl. No.: 13/829,332 release agent and a carrier may be disclosed. A method of controlling rodents at a locus by applying the composition of (22) Filed: Mar 14, 2013 the disclosure may be disclosed. Patent Application Publication Sep. 18, 2014 US 2014/0271932 A1 9ISI I? 80I (S.97) US 2014/027 1932 A1 Sep. 18, 2014 RODENTCIDAL COMPOSITION AND 0007. In another embodiment of the present disclosure the METHOD carbonate salt and/or the bicarbonate salt may further com 0001. The present disclosure relates to a rodenticide or prise an ammonium cation. The nitrogen of the ammonium composition and method for controlling rodents, e.g. com cation may be substituted with from 1 to 4 substituents each of mensal rodents. which may be alkyl, phenyl, aryl, heteroaryl, or alkoxy-Sub 0002 The present disclosure may include a composition stituted alkyl. By the term alkyl may be generally meant lower comprising a rodenticidally effective amount of a carbon alkyl, that may be from C to C alkyl, or from C to Calkyl. -

Current Awareness in Clinical Toxicology Editors: Damian Ballam Msc and Allister Vale MD
Current Awareness in Clinical Toxicology Editors: Damian Ballam MSc and Allister Vale MD December 2015 CONTENTS General Toxicology 8 Metals 35 Management 19 Pesticides 37 Drugs 21 Chemical Warfare 39 Chemical Incidents & 30 Plants 39 Pollution Chemicals 31 Animals 39 CURRENT AWARENESS PAPERS OF THE MONTH Case series: toxicity from 25B-NBOMe – A cluster of N-bomb cases Gee P, Schep LJ, Jensen BP, Moore G, Barrington S. Clin Toxicol 2015; online early: doi: 10.3109/15563650.2015.1115056: Background A new class of hallucinogens called NBOMes has emerged. This class includes analogues 25I-NBOMe, 25C-NBOMe and 25B-NBOMe. Case reports and judicial seizures indicate that 25I-NBOMe and 25C-NBOMe are more prevalently abused. There have been a few confirmed reports of 25B-NBOMe use or toxicity. Report Observational case series. This report describes a series of 10 patients who suffered adverse effects from 25B-NBOMe. Hallucinations and violent agitation predominate along with serotonergic/stimulant signs such as mydriasis, tachycardia, hypertension and hyperthermia. The majority (7/10) required sedation with benzodiazepines. Analytical method 25B-NBOMe concentrations in plasma and urine were quantified in all patients using a validated liquid chromatography?tandem mass spectrometry (LC-MS/MS) method. Peak plasma levels were measured between 0.7–10.1 ng/ml. Current Awareness in Clinical Toxicology is produced monthly for the American Academy of Clinical Toxicology by the Birmingham Unit of the UK National Poisons Information Service, with contributions from the Cardiff, Edinburgh, and Newcastle Units. The NPIS is commissioned by Public Health England 2 Discussion The NBOMes are desired by users because of their hallucinogenic and stimulant effects. -

2017 Reduced Risk Pesticide List
ATTACHMENT A: DRAFT 2017 REDUCED RISK PESTICIDE LIST 2017 San Francisco Reduced Risk Pesticide List: Restrictions on “most hazardous” (Tier I) herbicides 3/21/17 DRAFT Background The restrictions below were created in a public process by the San Francisco Department of the Environment Integrated Pest Management Program in close consultation with all City & County of San Francisco departments involved in land management activities, in keeping with the Precautionary Principle and Integrated Pest Management ordinances (Environment Code, Chapters 1 and 3). These restrictions apply only to “most hazardous” herbicides, defined here as herbicide products rated as “Tier I” using San Francisco’s Pesticide Hazard Screening Protocol. US EPA label restrictions take precedence and must be followed. All other uses of “most hazardous” herbicides require an exemption granted by the San Francisco Department of the Environment. Goals The goals of the restriction process are to: 1. Reduce the use of Tier I herbicides to those situations where they are most critical to public health, public safety, and protection of major public assets, including biodiversity assets, 2. Ensure that the restrictions are attainable through continued collaboration among City IPM staff. 3. Minimize potential harm to the environment, City workers, and the general public, in keeping with the Precautionary Principle. 4. Maximize the ability of city residents to know when and where these products are being used. Conditions of use for “most hazardous” herbicides General requirements 5. All postings must clearly identify the area to be treated, be set up three days before treatment, and be identifiable for four days after the treatment. -

Table of Contents
Table of Contents 1, 1-Dichloroethane 1, 2-Dichloroethane 1-Nitropyrene 2-Chloropropionitrile 2-Methoxyaniline; o-Anisidine 2-Nitrofuran 2-Nitropropane 4-(1,1,3,3-tetramethylbutyl)phenol 4,4'-diphenylmethane diisocyanate (MDI) 4-Nitrophenol Absorption Academy of Toxicological Sciences Acceptable Daily Intake (ADI) Accutane ACE Inhibitors Acenaphthene Acephate Acetaldehyde Acetamide Acetaminophen Acetamiprid Acetic Acid Acetone Acetonitrile Acetophenone Acetylaminofluorene Acetylcholine Acetylene Acetylsalicylic Acid Acids Acifluorfen, sodium salt Acrolein Acrylamide Acrylic Acid Acrylonitrile Acute Health Exposure Guidelines Adiponitrile Advances in Physiolocally-Based Modeling coupled with In Vitro In Vivo Extrapolation od ADMET: Adverse Outcome Pathways Aerosols A-esterases Aflatoxin Alachlor Alar Albuterol Alchemy Alcoholic Beverages and Alcoholism Aldicarb Aldrin Algae Alkalies Alkyl Halides Allyl Alcohol Allyl Formate Allylamine Alpha Blockers Aluminosilicate Fibers Aluminum Aluminum Phosphide Amdro American Academy of Clinical Toxicology American Association of Poison Control Centers American Board of Toxicology American College of Medical Toxicology American College of Toxicology American Conference of Governmental Industrial Hygienists American Industrial Hygiene Association Americium Ames Test Aminobiphenyl, 4- Aminoglycosides Aminopyridine, 4- Amiodarone Amitraz Amitrole Ammonia Ammonium Nitrate Amphetamines Amyl Nitrite Anabolic Steroids Analytical Toxicology Ancient Warfare and Toxicology Androgens Anesthetic Agents Aneuploidy -

Rodenticides - Kramer R.E
ENVIRONMENTAL TOXICOLOGY AND HUMAN HEALTH – Vol. I - Rodenticides - Kramer R.E. and Baker R.C. RODENTICIDES Kramer R.E. and Baker R.C. Department of Pharmacology and Toxicology, University of Mississippi Medical Center, U.S.A. Keywords: Fluoroacetate, sodium monofluoroacetate, compound 1080, fluorocitrate, fluoroacetamide, compound 1081, 1,3-difluoro-2-propanol, DFP, thiourea, α- naphthylthiourea, ANTU, pyriminil, PNU, Vacor, bromethalin, vitamin D, cholecalciferol, ergocalciferol, norbormide, scillirosides, scillirosidin, glycosides, α- chlorohydrin, thallium, phosphorus, zinc phosphide, aluminum phosphide, phosphine, strychnine, anticoagulants, brodifacoum, bromadiolone, chlorophacinone, coumachlor, difenacoum, diphencoumarin, difethialone, diphacinone, flocoumafen, pindone, warfarin, vitamin K, mechanisms of action, toxicity, treatment; antidotes Contents 1. Introduction 2. Fluoroacetate derivatives 2.1. Sodium Monofluoroacetate 2.2. Fluoroacetamide 2.3. 1,3-Difluoro-2-propanol 3. Thiourea Rodenticides 3.1. α-Naphthylthiourea (ANTU) 3.2. Pyriminil 4. Bromethalin 5. Vitamin D-based rodenticides 6. Norbormide 7. Scilliroside 8. Alpha (α)-chlorohydrin 9. Thallium 10. Yellow phosphorus 11. Zinc phosphide 12. Strychnine 13. Anticoagulant rodenticides Glossary BibliographyUNESCO – EOLSS Biographical Sketches SAMPLE CHAPTERS Summary A rodenticide is defined as any compound used to kill rodents or other small animals. They are widely used, and as a class encompass a disparate group of compounds with differing structures and mechanisms of action.