Veterinary Toxicology
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

PVC) Products ______
CPSC Staff Report on Lead and Cadmium in Children's Polyvinyl Chloride (PVC) Products ___________________________________________ 21 November 1997 U.S. Consumer Product Safety Commission Washington, D.C. 20207 CPSC Staff Report on Lead and Cadmium in Children's Polyvinyl Chloride (PVC) Products November 1997 I. Introduction Since its inception, the U.S. Consumer Product Safety Commission (CPSC) has played a prominent role in protecting the public, especially children, from the hazards of exposure to lead and other toxic chemicals. The CPSC has a strong record of removing products from the marketplace that contain lead and result in exposures that are hazardous to children. Just this past year, Commission action resulted in manufacturers eliminating the use of lead as a stabilizer in vinyl miniblinds, stopping the production of children's jewelry containing lead, and developing and distributing guidance to state health officials and others about lead paint on public playground equipment. Several years ago, CPSC recalled crayons that contained hazardous levels of lead. The Commission is continually screening toys for the presence of lead paint and has recalled many toys that violated the Commission's lead paint standard. In 1996, CPSC found that children could be exposed to hazardous levels of lead in imported non-glossy vinyl (polyvinyl chloride, PVC) miniblinds. Following this discovery, CPSC staff collected and tested a number of children's plastic products that they believed might be repeatedly exposed to sunlight and heat such as the vinyl miniblinds. This type of exposure was shown by CPSC staff to promote the deterioration of the lead-containing PVC miniblind slats and result in the formation of lead dust on the slats' surface. -
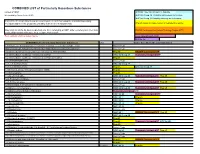
COMBINED LIST of Particularly Hazardous Substances
COMBINED LIST of Particularly Hazardous Substances revised 2/4/2021 IARC list 1 are Carcinogenic to humans list compiled by Hector Acuna, UCSB IARC list Group 2A Probably carcinogenic to humans IARC list Group 2B Possibly carcinogenic to humans If any of the chemicals listed below are used in your research then complete a Standard Operating Procedure (SOP) for the product as described in the Chemical Hygiene Plan. Prop 65 known to cause cancer or reproductive toxicity Material(s) not on the list does not preclude one from completing an SOP. Other extremely toxic chemicals KNOWN Carcinogens from National Toxicology Program (NTP) or other high hazards will require the development of an SOP. Red= added in 2020 or status change Reasonably Anticipated NTP EPA Haz list COMBINED LIST of Particularly Hazardous Substances CAS Source from where the material is listed. 6,9-Methano-2,4,3-benzodioxathiepin, 6,7,8,9,10,10- hexachloro-1,5,5a,6,9,9a-hexahydro-, 3-oxide Acutely Toxic Methanimidamide, N,N-dimethyl-N'-[2-methyl-4-[[(methylamino)carbonyl]oxy]phenyl]- Acutely Toxic 1-(2-Chloroethyl)-3-(4-methylcyclohexyl)-1-nitrosourea (Methyl-CCNU) Prop 65 KNOWN Carcinogens NTP 1-(2-Chloroethyl)-3-cyclohexyl-1-nitrosourea (CCNU) IARC list Group 2A Reasonably Anticipated NTP 1-(2-Chloroethyl)-3-cyclohexyl-1-nitrosourea (CCNU) (Lomustine) Prop 65 1-(o-Chlorophenyl)thiourea Acutely Toxic 1,1,1,2-Tetrachloroethane IARC list Group 2B 1,1,2,2-Tetrachloroethane Prop 65 IARC list Group 2B 1,1-Dichloro-2,2-bis(p -chloropheny)ethylene (DDE) Prop 65 1,1-Dichloroethane -

Full Article-PDF
Bachu Naveena et al, IJMPR, 2015, 3(1): 948–955 ISSN: 2321-2624 International Journal of Medicine and Pharmaceutical Research Journal Home Page: www.pharmaresearchlibrary.com/ijmpr Review Article Open Access Health Effects and Benefits of Chocolate Bachu Naveena*, Chennuru Madavi latha, Pigilam Sri Chandana, Pamula Nandini, Koppolu Hyndavi Narayana Pharmacy College, Chinthareddypalem, Nellore, Andhra Pradesh, India. A B S T R A C T Its history can be traced back to the ancient peoples of Central and South America. Early civilizations gave a religious significance to their beloved cocoa and their descendants still give offerings of cacao to their gods to this day. Chocolate may even have helped change the course of history. One of the great riches of the New World discovered by the conquistadors, a vein of chocolate runs through many historical events: imperialism and the slave trade, revolutions planned in the coffee houses of 17th-century Europe, the Industrial Revolution and as a welcome boost to the morale of troops in many wars. Today, it is impossible to imagine a world without chocolate. In the words of Milton Hershey, founder of the Hershey Chocolate Company, "caramels are only a fad. Chocolate is a permanent thing. Keywords: Physico-chemical traits, ash values, SEM, FT-IR spectroscopy A R T I C L E I N F O CONTENTS 1. Introduction . 948 2. Benefits of Chocolates. .949 3. Effects of Chocolates. 952 4. Conclusion . .. .. .954 5. References . .954 Article History: Received 15 October 2014, Accepted 10 December 2014, Available Online 10 February 2015 *Corresponding Author Bachu Naveena Narayana Pharmacy College, Chinthareddypalem, Nellore, Andhra Pradesh, India. -
Health Concerns of Heavy Metals (Pb; Cd; Hg) and Metalloids (As)
Health concerns of the heavy metals and metalloids Chris Cooksey • Toxicity - acute and chronic • Arsenic • Mercury • Lead • Cadmium Toxicity - acute and chronic Acute - LD50 Trevan, J. W., 'The error of determination of toxicity', Proc. Royal Soc., 1927, 101B, 483-514 LD50 (rat, oral) mg/kg CdS 7080 NaCl 3000 As 763 HgCl 210 NaF 52 Tl2SO4 16 NaCN 6.4 HgCl2 1 Hodge and Sterner Scale (1943) Toxicity Commonly used term LD50 (rat, oral) Rating 1 Extremely Toxic <=1 2 Highly Toxic 1 - 50 3 Moderately Toxic 50 - 500 4 Slightly Toxic 500 - 5000 5 Practically Non-toxic 5000 - 15000 6 Relatively Harmless >15000 GHS - CLP LD50 Category <=5 1 Danger 5 - 50 2 Danger 50 - 300 3 Danger 300 - 2000 4 Warning Globally Harmonised System of Classification and Labelling and Packaging of Chemicals CLP-Regulation (EC) No 1272/2008 Toxicity - acute and chronic Chronic The long-term effect of sub-lethal exposure • Toxicity - acute and chronic • Arsenic • Mercury • Lead • Cadmium Arsenic • Pesticide o Inheritance powder • Taxidermy • Herbicide o Agent Blue • Pigments • Therapeutic uses Inorganic arsenic poisoning kills by allosteric inhibition of essential metabolic enzymes, leading to death from multi- system organ failure. Arsenicosis - chronic arsenic poisoning. Arsenic LD50 rat oral mg/kg 10000 1000 LD50 100 10 1 Arsine Arsenic acid Trimethylarsine Emerald green ArsenicArsenious trisulfide oxideSodium arsenite MethanearsonicDimethylarsinic acid acid Arsenic poisoning by volatile arsenic compounds from mouldy wall paper in damp rooms • Gmelin (1839) toxic mould gas • Selmi (1874) AsH3 • Basedow (1846) cacodyl oxide • Gosio (1893) alkyl arsine • Biginelli (1893) Et2AsH • Klason (1914) Et2AsO • Challenger (1933) Me3As • McBride & Wolfe (1971) Me2AsH or is it really true ? William R. -

Official Newsletter of the German Wirehaired Pointer Club of Northern California
Official Newsletter of the German Wirehaired Pointer Club of Northern California March/April/May2013 Volume 3 - Issue 3 Newsletter Editor: Diane Marsh [email protected] 2013 Club Officers President Francis Marsh Vice President Cindy Heiller, DVM Secretary Debbie Lewis Treasurer Diane Marsh 2013 Directors Silke Alberts Randy Berry Frank Ely Robert Lewis Joan Payton Club Web Site: www.gwpcnc.9f.com Web Master: Kathy Kimberlin [email protected] Informational Web Sites AKC American Kennel Club www.akc.org GWPA German Wirehaired Pointer Club of America www.gwpca.com GWPCNC German Wirehaired Pointer Club of N. California www.gwpcnc.9f.com NAVHDA N. American Versatile Hunting Dog Association www.navhda.org OFA Orthopedic Foundation For Animals www.offa.org VHDF Versatile Hunting Dog Federation www.vhdf.org German Wirehair Alliance - www.wirehairalliance.com (promoting and safeguarding the breed) 1 Welcome New Members: Cliff & Joan Thomas 2 Happy “Belated” Birthday Mildred.... April 17th (thank you Janet Levy for the birthday picture) Submitted by Sharon Jahn Many of our new club members have not had the opportunity of meeting Mildred Revell. I, along with other early members, consider her the “matriarch” of our club, so am including a little history about Mildred’s involvement in the early years of the GWP. Mildred was recognized at the 2006 GWP Nationals Awards Banquet with an Award of Appreciation. The following information is reprinted from the winter 2006 Wire News: “...Her first Wirehair in 1969, an anniversary gift from her hus- band, convinced Mildred that the GWP was the breed for her. Prior to the acquisition of the first Wirehair, CH Weidenhugel Anniversary, Mildred bred German Shorthairs under the Weidenbach prefix, but quickly found she preferred the Wirehairs – and so the Weidenhugel prefix was creat- ed to distinguish the GWPs from the Shorthairs. -

Environmental Properties of Chemicals Volume 2
1 t ENVIRONMENTAL 1 PROTECTION Esa Nikunen . Riitta Leinonen Birgit Kemiläinen • Arto Kultamaa Environmental properties of chemicals Volume 2 1 O O O O O O O O OO O OOOOOO Ol OIOOO FINNISH ENVIRONMENT INSTITUTE • EDITA Esa Nikunen e Riitta Leinonen Birgit Kemiläinen • Arto Kultamaa Environmental properties of chemicals Volume 2 HELSINKI 1000 OlO 00000001 00000000000000000 Th/s is a second revfsed version of Environmental Properties of Chemica/s, published by VAPK-Pub/ishing and Ministry of Environment, Environmental Protection Department as Research Report 91, 1990. The pubiication is also available as a CD ROM version: EnviChem 2.0, a PC database runniny under Windows operating systems. ISBN 951-7-2967-2 (publisher) ISBN 952-7 1-0670-0 (co-publisher) ISSN 1238-8602 Layout: Pikseri Julkaisupalvelut Cover illustration: Jussi Hirvi Edita Ltd. Helsinki 2000 Environmental properties of chemicals Volume 2 _____ _____________________________________________________ Contents . VOLUME ONE 1 Contents of the report 2 Environmental properties of chemicals 3 Abbreviations and explanations 7 3.1 Ways of exposure 7 3.2 Exposed species 7 3.3 Fffects________________________________ 7 3.4 Length of exposure 7 3.5 Odour thresholds 8 3.6 Toxicity endpoints 9 3.7 Other abbreviations 9 4 Listofexposedspecies 10 4.1 Mammais 10 4.2 Plants 13 4.3 Birds 14 4.4 Insects 17 4.5 Fishes 1$ 4.6 Mollusca 22 4.7 Crustaceans 23 4.8 Algae 24 4.9 Others 25 5 References 27 Index 1 List of chemicals in alphabetical order - 169 Index II List of chemicals in CAS-number order -

Behavior of Α-Tomatine and Tomatidine Against Several Genera of Trypanosomatids from Insects and Plants and Trypanosoma Cruzi
Acta Scientiarum http://periodicos.uem.br/ojs/acta ISSN on-line: 1807-863X Doi: 10.4025/actascibiolsci.v40i1.41853 BIOTECHNOLOGY Behavior of α-tomatine and tomatidine against several genera of trypanosomatids from insects and plants and Trypanosoma cruzi Adriane Feijó Evangelista1, Erica Akemi Kavati2, Jose Vitor Jankevicius3 and Rafael Andrade Menolli4* 1Centro de Pesquisa em Oncologia Molecular, Hospital de Câncer de Barretos, Barretos, São Paulo, Brazil. 2Laboratório de Genética, Instituto Butantan, São Paulo, São Paulo, Brazil. 3Departamento de Microbiologia, Universidade Estadual de Londrina, Londrina, Paraná, Brazil. 4Centro de Ciências Médicas e Farmacêuticas, Universidade Estadual do Oeste do Paraná, Rua Universitária, 2069, 85819-110, Cascavel, Paraná, Brazil. *Author for correspondence. E-mail: [email protected] ABSTRACT. Glycoalkaloids are important secondary metabolites accumulated by plants as protection against pathogens. One of them, α-tomatine, is found in high concentrations in green tomato fruits, while in the ripe fruits, its aglycone form, tomatidine, does not present a protective effect, and it is usual to find parasites of tomatoes like Phytomonas serpens in these ripe fruits. To investigate the sensitivity of trypanosomatids to the action of α-tomatine, we used logarithmic growth phase culture of 20 trypanosomatids from insects and plants and Trypanosoma cruzi. The lethal dose 50% (LD50) was determined by mixing 107 cells of the different isolates with α-tomatine at concentrations ranging from 10-3 to 10-8 M for 30 min at room temperature. The same tests performed with the tomatidine as a control showed no detectable toxicity against the same trypanosomatid cultures. The tests involved determination of the percentage (%) survival of the protozoan cultures in a Neubauer chamber using optical microscopy. -

Penitrem and Thomitrem Formation by Penicillium Crustosum
Mycopathologia 157: 349–357, 2004. 349 © 2004 Kluwer Academic Publishers. Printed in the Netherlands. Penitrem and thomitrem formation by Penicillium crustosum Thomas Rundberget1, Ida Skaar1, Oloff O’Brien2 & Arne Flåøyen1 1National Veterinary Institute, PO Box 8156 Dep., 0033 Oslo, Norway; 2ARC Plant Protection, Research Institute, Private Bag X134, Pretoria 0001, South Africa Received 9 September 2002; accepted in final form 16 July 2003 Abstract The levels of penitrems A, B, C, D, E, F, roquefortine C and thomitrem A and E recovered from extracts of 36 Norwegian, 2 American and one each of Japanese, German, South African, Danish and Fijian isolates of Penicillum crustosum Thom were quantitatively determined using high performance liquid chromatography-mass spectrometry (HPLC-MS). Forty-two of the 44 isolates of penitrem-producing isolates grown on rice, afforded levels of thomitrem A and E comparable to that of penitrem A. Thomitrems A and E were also found, but at lower levels, when cultures were grown on barley. No thomitrems were found when the isolates were grown on liquid media. The effects of time and temperature on mycotoxin formation were studied on rice over a 4 week period at 10, 15 and 25 ◦C, respectively. No mycotoxins could be detected after 1 week at 10 ◦C, but after 2 weeks at 10 ◦C levels were similar to those produced at 15 and 25 ◦C. Higher levels of thomitrems A and E were detected when media were maintained at lower pH. The possibility that thomitrems A and E might be derived by acid promoted conversion of penitrems A and E was explored in stability trials performed at pH 2, 3, 4, 5 and 7 in the presence and absence of media. -

Alpha-Tomatine Content in Tomato and Tomato Products Determined By
J. Agric. Food Chem. 1995, 43, 1507-151 1 1507 a-Tomatine Content in Tomato and Tomato Products Determined by HPLC with Pulsed Amperometric Detection Mendel Friedman* and Carol E. Levin Food Safety and Health Research Unit, Western Regional Research Center, Agricultural Research Service, U.S. Department of Agriculture, 800 Buchanan Street, Albany, California 94710 Tomato plants (Lycopersicon esculentum) synthesize the glycoalkaloid a-tomatine, possibly as a defense against insects and other pests. As part of an effort to improve the safety of plant foods, the usefulness of a new HPLC pulsed amperometric detection (PAD) method for the direct analysis of a-tomatine in different parts of the tomato plant; in store-bought and field-grown, including transgenic, tomatoes; in a variety of commercial and home-processed tomato products; and in eggplant and tomatillos was evaluated. The method was found to be useful for analysis of a variety of products including high-tomatine calyxes, flowers, leaves, roots, and stems of the tomato plant (14-130 mg/100 g of fresh weight), low-tomatine red tomatoes (0.03-0.08 mg/100 g), intermediate- tomatine tomatoes (0.1-0.8 mg/100 g), and high-tomatine fresh and processed green, including pickled and fried, tomatoes (0.9-55 mg/100 g). No experimental difficulties were encountered with extraction and analysis of tomatine in complex foods such as tomato juice, ketchup, salsa, sauce, and sun-dried tomatoes. Microwaving and frying did not significantly affect tomatine levels of tomato foods. The tomatine content of fresh market and transgenic delayed-ripening varieties was not different from the range ordinarily seen in tomato. -

(BK) Channel Antagonist Penitrem a As a Novel Breast Cancer-Targeted Therapeutic
marine drugs Article The Maxi-K (BK) Channel Antagonist Penitrem A as a Novel Breast Cancer-Targeted Therapeutic Amira A. Goda 1, Abu Bakar Siddique 1 ID , Mohamed Mohyeldin 1,3, Nehad M. Ayoub 2 ID and Khalid A. El Sayed 1,* ID 1 Department of Basic Pharmaceutical Sciences, School of Pharmacy, University of Louisiana at Monroe, 1800 Bienville Drive, Monroe, LA 71201, USA; [email protected] (A.A.G.); [email protected] (A.B.S.); [email protected] (M.M.) 2 Department of Clinical Pharmacy, Faculty of Pharmacy, Jordan University of Science and Technology, Irbid 22110, Jordan; [email protected] 3 Department of Pharmacognosy, Faculty of Pharmacy, Alexandria University, Alexandria 21521, Egypt * Correspondence: [email protected]; Tel.: +1-318-342-1725 Received: 6 April 2018; Accepted: 9 May 2018; Published: 11 May 2018 Abstract: Breast cancer (BC) is a heterogeneous disease with different molecular subtypes. The high conductance calcium-activated potassium channels (BK, Maxi-K channels) play an important role in the survival of some BC phenotypes, via membrane hyperpolarization and regulation of cell cycle. BK channels have been implicated in BC cell proliferation and invasion. Penitrems are indole diterpene alkaloids produced by various terrestrial and marine Penicillium species. Penitrem A (1) is a selective BK channel antagonist with reported antiproliferative and anti-invasive activities against multiple malignancies, including BC. This study reports the high expression of BK channel in different BC subtypes. In silico BK channel binding affinity correlates with the antiproliferative activities of selected penitrem analogs. 1 showed the best binding fitting at multiple BK channel crystal structures, targeting the calcium-sensing aspartic acid moieties at the calcium bowel and calcium binding sites. -

The ABC of Drugs
LSD Joint Liquor Morphine Breath DrugTest 5000 Gin Lane Intoxication Witches Cheerful Purity Law Skin Evidential DRUID Sensor SpeedballAlcohol Ban Dependency Cocaine Emotions Sober Legalization BAC Roadside Checkpoint Opioids Drunk Ritalin Amphetamines Crack F.W. Sertürner Spice Profit Corn Schnapps EthanolInebriated Industrial Safety Sympathetic Nervous System Opium Sampling Unable to DriveUnable to War on Drugs War Blood Drugs Limits Prohibition MDMA Labrador Tea Catalyzer Poison Traffic Prevention Locoweed Reactions HeroinKhat Soul Pretest Bootlegger Rights Urine Shamans Injection IntoxicantRoad Deaths High-risk Professions Sober Alcohol Saliva Illegal Tube CultureAuthor Synthetic Wine Pervitin VodkaShisha Ecstasy PPT Paracelsus Beer Marijuana Electrochemical Alcotest Sweat Approval Drugs – ABCs Enzyme Ankle Bracelet Here is a brief, factual tour of commonly used drugs – their active ingredients as well as methods of use, risks, prevalence (frequency of use), origin, and history. © Drägerwerk AG & Co. KGaA 1 Drugs – ABCS Drugs – ABCS and sleep-in ducing purposes; their consumed cannabis at least once in Origins and history: the coca bush inter national non-proprietary names their lives. 6.8 percent of the same age has been cultivated in South America Drugs – ABCs often end in -azepam: Diazepam, group have consumed it within the for a good 5,000 years. Its leaves may Lorazepam and Oxazepam. Trade names past twelve months – or one out of three only have been used for ritual activities include Valium, Librium, Rohypnol, people have experimented with cannabis. initially. When impoverishment set in with Tavor, and Praxiten. Risks: restricted physical and mental the Spanish conquest, large sections Form of consumption: as tablets capacity, coupled with self-overestimation; of the population used the plant to stave or injected intraveneously. -

The Veterinarian's Guide
The Veterinarian’s Guide Bromethalin Addendum The Soft Bait Innovators™ Liphatech, Inc. • 3600 W. Elm Street • Milwaukee, WI 53209 • 1-888-331-7900 • www.liphatech.com NOTE: The information in this guide does not represent labeling and does not replace information on rodenticide labels relating to exposure of non-target species. Please read and follow all label directions on all rodenticide products you are using. Mentions of trade names in this publication does not imply endorsement of these products. Assault® is a registered trademark of PM Resources (St. Louis, MO) TakeDown™ and Cannon™ are trademarks of Liphatech, Inc. (Milwaukee, WI) Gunslinger® is a registered trademark of Liphatech, Inc. (Milwaukee, WI) Fastrac® is a registered trademark of Bell Labs (Madison, WI) Top Gun™ is a trademark of JT Eaton (Twinsburg, OH) Tomcat® and Rampage® are registered trademarks of Motomco (Madison, WI) Trounce® is a registered trademark of Agricultural Feeds (St. Louis, MO) At the time of this printing all information was deemed accurate and reliable. Liphatech, Inc. 3600 W. Elm Street Milwaukee, WI 53209 1-888-331-7900 www.liphatech.com October, 2016 The Veterinarian’s Guide - Bromethalin Addendum The Veterinarian’s Guide to Accidental Rodenticide Ingestion by Dogs and Cats focuses on anticoagulants. This addendum is intended to help veterinarians recognize and treat the symptoms of bromethalin toxicity in domestic animals. It describes bromethalin’s mode of action and how it is used as a rodenticide. In addition to reviewing the symptoms of bromethalin poisoning in domestic animals and the acute toxicity levels for dogs and cats (Table 5), we have also included the American Society for Prevention of Cruelty to Animals’ Animal Poison Control Center (ASPCA APCC) recommendations for decontamination (Tables 6 and 7).