Upper Limb Lecture Three Brachial Plexus
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Study of Brachial Plexus with Regards to Its Formation, Branching Pattern and Variations and Possible Clinical Implications of Those Variations
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 15, Issue 4 Ver. VII (Apr. 2016), PP 23-28 www.iosrjournals.org Study of Brachial Plexus With Regards To Its Formation, Branching Pattern and Variations and Possible Clinical Implications of Those Variations. Dr. Shambhu Prasad1, Dr. Pankaj K Patel2 1 (Assistant Professor , Department of Anatomy , NMCH , Sasaram , India ) 2 (Assistant Professor , Department of Pathology , NMCH , Sasaram , India ) Abstract: Aim of the study: to search variations in formation and branching pattern of brachial plexus and correlate them with possible clinical and surgical implications. Materials and Methods: 25human bodies were dissected for this study. Dissection was started in posterior triangle of neck and extended to distal part of upper limb passing through axilla . Photographs were taken and data was tabulated and analyzed . Observations: All 50 plexuses had origin from C5 – T1 . Dorsal scapular nerve was absent in 2 plexuses. Long thoracic nerve was made of C5,C6 fibers in one and of C6,C7 fibers in another . Lower trunk was abnormal in 2 plexuses both of same body, their was no contribution from T1 fibers to posterior cord in one of these plexus. One plexus had double lateral pectoral nerve , communication between lateral and medial pectoral nerves , lateral pectoral and medial root of median nerve also between musculocutaneous and lateral root of median nerve . 2 more plexuses had communication between lateral and medial pectoral nerves. One plexus showed 2 branches coming from posterior division of upper trunk itself before formation of posterior cord. -
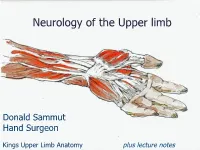
Neurology of the Upper Limb
Neurology of the Upper limb Donald Sammut Hand Surgeon Kings Upper Limb Anatomy plus lecture notes The$Neck$ The$Nerve$roots$which$supply$the$Upper$Limb$are$C5$to$T1$ Pre<fixed$(C4$to$C8)$and$Post<fixed$(C6$to$T2)$plexus$not$uncommon.$ Also$common$contributions$from$C4$and$from$T2$in$a$normally$rooted$plexus.$ $ The$anterior$nerve$roots$emerge$between$the$vertebrae$and$immediately$pass$ $through$the$first$area$of$possible$compression:$ The$root$nerve$canal$is$bounded$$ Anteriorly$by$the$posterior$margin$of$the$intervertebral$disc$and$$ Posteriorly,$by$the$facet$joint$between$vertebrae.$ $ Pathology$of$the$disc,$or$joint,$or$both,$can$narrow$this$channel$and$compress$ $the$nerve$root$ The$roots$emerge$from$the$cervical$spine$into$the$plane$between$$ Scalenius$Anterior$and$Scalenius$Medius.$$ $ Scalenius*Anterior:** Origin:$Anterior$tubercles$of$Cervical$vertebae$C3$to$6$(C6$tubercle$is$the$Carotid$tubercle)$ Insertion:$The$scalene$tubercle$on$inner$border/upper$surface$1st$rib$ $ Scalenius*Medius:* Origin:$Posterior$tubercles$of$all$cervical$vertebrae$ Insertion:$Quadrangular$area$between$the$neck$and$subclavian$groove$1st$rib$ $ Exiting$from$the$Scalenes,$the$trunks$lie$in$the$posterior$triangle$of$the$neck.$ The$posterior$triangle$is$bounded$anteriorly$by$SternoCleidoMastoid$and$$ posteriorly$by$the$Trapezius.$ The$inferior$border$is$the$clavicle$.$ The$apex$of$the$triangle$superiorly$is$at$the$back$of$the$skull$on$the$superior$nuchal$line$ $ $ The$Posterior$Triangle$ SternoCleidoMastoid$ Trapezius$ Scalenius$Medius$ Scalenius$Anterior$ -
Brachial Plexus and Branches Axillary A
Regional Anatomy of the Upper Limb 1 Wu Genghua Medical College Yangzhou University Anterior surface of the •Incisions: Upper Limb Make the skin incisions indicated in figure and reflect the skin flaps. Be careful not to cut too deep. As you remove the skin, look for the cephalic v., basilic v. and median cubital v. Superficial veins and nerves Mamma Structures Contains skin, mammary glands and adipose tissue Consists of 15 to 20 Lobes of mammary gland that radiate outward from the nipple lactiferous duct lactiferous sinuse Suspensory ligaments of breast (cooper’s ligaments): connective tissue septa that extend from the skin to the deep fascia Pectoral Region Superficial structures Superficial n. Supraclavicular n. Anterior cutaneous branches of intercostal n. lateral cutaneous branches of intercostal n. Muscles connecting the upper limb to the thoracic wall Pectoralis major 胸大肌 Subclevius 锁骨下肌 Pectoralis minor 胸小肌 Serratus anterior 前锯肌 Pectoral Region Deep structures clavipectoral fascia The deep fascia which extends between subclavius, coracoid process and pectoralis minor muscles The structures pass through the clavipectoral fascia . Cephalic v. Thoracoacromial a. Lateral pectoral n. Axillary region 腋区 Boundaries of the axillary fossa Apex is bounded by Middle 1/3 of clavicle Lateral border of first rib Upper border of the scapula Base is formed by the skin stretching between the anterior and posterior walls Anterior wall Formed by pectoralis major, pectoralis minor and subclavius muscles Boundaries of the axillary fossa The posterior wall latissimus dorsi teres major subscapularis and scapula Trilateral and quadrilateral space The posterior humeral circumflex a. and axillary n. pass through the quadrilateral foramen. -

Brachial Plexus Posterior Cord Variability: a Case Report and Review
CASE REPORT Brachial plexus posterior cord variability: a case report and review Edward O, Arachchi A, Christopher B Edward O, Arachchi A, Christopher B. Brachial plexus posterior cord anatomical variability. This case report details the anatomical variants discovered variability: a case report and review. Int J Anat Var. 2017;10(3):49-50. in the posterior cord of the brachial plexus in a routine cadaveric dissection at the University of Melbourne, Australia. Similar findings in the literature are reviewed ABSTRACT and the clinical significance of these findings is discussed. The formation and distribution of the brachial plexus is a source of great Key Words: Brachial plexus; Posterior cord; Axillary nerve; Anatomical variation INTRODUCTION he brachial plexus is the neural network that supplies motor and sensory Tinnervation to the upper limb. It is typically composed of anterior rami from C5 to T1 spinal segments, which subsequently unite to form superior, middle and inferior trunks. These trunks divide and reunite to form cords 1 surrounding the axillary artery, which terminate in branches of the plexus. The posterior cord is classically described as a union of the posterior divisions from the superior, middle and inferior trunks of the brachial plexus, with fibres from all five spinal segments. The upper subscapular, thoracodorsal and lower subscapular nerves propagate from the cord prior to the axillary and radial nerves forming terminal branches. Variability in the brachial plexus is frequently reported in the literature. It is C5 nerve root Suprascapular nerve important for clinicians to be aware of possible variations when considering Posterior division of C5-C6 injuries or disease of the upper limb. -

Pectoral Region and Axilla Doctors Notes Notes/Extra Explanation Editing File Objectives
Color Code Important Pectoral Region and Axilla Doctors Notes Notes/Extra explanation Editing File Objectives By the end of the lecture the students should be able to : Identify and describe the muscles of the pectoral region. I. Pectoralis major. II. Pectoralis minor. III. Subclavius. IV. Serratus anterior. Describe and demonstrate the boundaries and contents of the axilla. Describe the formation of the brachial plexus and its branches. The movements of the upper limb Note: differentiate between the different regions Flexion & extension of Flexion & extension of Flexion & extension of wrist = hand elbow = forearm shoulder = arm = humerus I. Pectoralis Major Origin 2 heads Clavicular head: From Medial ½ of the front of the clavicle. Sternocostal head: From; Sternum. Upper 6 costal cartilages. Aponeurosis of the external oblique muscle. Insertion Lateral lip of bicipital groove (humerus)* Costal cartilage (hyaline Nerve Supply Medial & lateral pectoral nerves. cartilage that connects the ribs to the sternum) Action Adduction and medial rotation of the arm. Recall what we took in foundation: Only the clavicular head helps in flexion of arm Muscles are attached to bones / (shoulder). ligaments / cartilage by 1) tendons * 3 muscles are attached at the bicipital groove: 2) aponeurosis Latissimus dorsi, pectoral major, teres major 3) raphe Extra Extra picture for understanding II. Pectoralis Minor Origin From 3rd ,4th, & 5th ribs close to their costal cartilages. Insertion Coracoid process (scapula)* 3 Nerve Supply Medial pectoral nerve. 4 Action 1. Depression of the shoulder. 5 2. Draw the ribs upward and outwards during deep inspiration. *Don’t confuse the coracoid process on the scapula with the coronoid process on the ulna Extra III. -

Electrodiagnosis of Brachial Plexopathies and Proximal Upper Extremity Neuropathies
Electrodiagnosis of Brachial Plexopathies and Proximal Upper Extremity Neuropathies Zachary Simmons, MD* KEYWORDS Brachial plexus Brachial plexopathy Axillary nerve Musculocutaneous nerve Suprascapular nerve Nerve conduction studies Electromyography KEY POINTS The brachial plexus provides all motor and sensory innervation of the upper extremity. The plexus is usually derived from the C5 through T1 anterior primary rami, which divide in various ways to form the upper, middle, and lower trunks; the lateral, posterior, and medial cords; and multiple terminal branches. Traction is the most common cause of brachial plexopathy, although compression, lacer- ations, ischemia, neoplasms, radiation, thoracic outlet syndrome, and neuralgic amyotro- phy may all produce brachial plexus lesions. Upper extremity mononeuropathies affecting the musculocutaneous, axillary, and supra- scapular motor nerves and the medial and lateral antebrachial cutaneous sensory nerves often occur in the context of more widespread brachial plexus damage, often from trauma or neuralgic amyotrophy but may occur in isolation. Extensive electrodiagnostic testing often is needed to properly localize lesions of the brachial plexus, frequently requiring testing of sensory nerves, which are not commonly used in the assessment of other types of lesions. INTRODUCTION Few anatomic structures are as daunting to medical students, residents, and prac- ticing physicians as the brachial plexus. Yet, detailed understanding of brachial plexus anatomy is central to electrodiagnosis because of the plexus’ role in supplying all motor and sensory innervation of the upper extremity and shoulder girdle. There also are several proximal upper extremity nerves, derived from the brachial plexus, Conflicts of Interest: None. Neuromuscular Program and ALS Center, Penn State Hershey Medical Center, Penn State College of Medicine, PA, USA * Department of Neurology, Penn State Hershey Medical Center, EC 037 30 Hope Drive, PO Box 859, Hershey, PA 17033. -

Variant Branches of Brachial Plexus - a Case Report
eISSN 1308-4038 International Journal of Anatomical Variations (2012) 5: 5–7 Case Report Variant branches of brachial plexus - a case report Published online April 8th, 2012 © http://www.ijav.org Prashant Nashiket CHAWARE Abstract Jaideo Manohar UGHADE During routine dissection of brachial plexus we observed two upper subscapular nerves. These two upper subscapular nerves, lower subscapular nerve and axillary nerve arose from posterior Sudhir Vishnupant PANDIT division of upper trunk. Posterior cord gave thoracodorsal nerve and continued as radial Gajanan Laxmanrao MASKE nerve. We also found that anterior division of middle trunk divided into two branches; anterior division-a and anterior division-b. Anterior division-a joined anterior division of upper trunk to Department of Anatomy, Shri Vasantrao Naik Government form the lateral cord. Anterior division-b joined medial root-1 of median nerve to form medial root-2 of median nerve. This medial root-2 joined with lateral root of median nerve to form Medical College, Yavatmal, Maharashtra, INDIA. median nerve. The anterior division-b carrying fibers from C7 primary ramus, contributed fibers to form medial root-2 of median nerve and then joined with the ulnar nerve. Presence of C7 root Dr. Prashant Nashiket Chaware in ulnar nerve was clearly seen in our case, which is seldom visualized in routine dissection. © Assistant Professor Int J Anat Var (IJAV). 2012; 5: 5–7. Department of Anatomy Shri Vasantrao Naik Government Medical College Yavatmal, Maharashtra 445001, INDIA. +91 7232 242456 ext. 157 [email protected] Received September 8th, 2011; accepted March 10th, 2012 Key words [posterior cord] [median nerve] [ulnar nerve] [nerve variations] Introduction trunk was much thinner than the others (Figure 1). -

Section 1 Upper Limb Anatomy 1) with Regard to the Pectoral Girdle
Section 1 Upper Limb Anatomy 1) With regard to the pectoral girdle: a) contains three joints, the sternoclavicular, the acromioclavicular and the glenohumeral b) serratus anterior, the rhomboids and subclavius attach the scapula to the axial skeleton c) pectoralis major and deltoid are the only muscular attachments between the clavicle and the upper limb d) teres major provides attachment between the axial skeleton and the girdle 2) Choose the odd muscle out as regards insertion/origin: a) supraspinatus b) subscapularis c) biceps d) teres minor e) deltoid 3) Which muscle does not insert in or next to the intertubecular groove of the upper humerus? a) pectoralis major b) pectoralis minor c) latissimus dorsi d) teres major 4) Identify the incorrect pairing for testing muscles: a) latissimus dorsi – abduct to 60° and adduct against resistance b) trapezius – shrug shoulders against resistance c) rhomboids – place hands on hips and draw elbows back and scapulae together d) serratus anterior – push with arms outstretched against a wall 5) Identify the incorrect innervation: a) subclavius – own nerve from the brachial plexus b) serratus anterior – long thoracic nerve c) clavicular head of pectoralis major – medial pectoral nerve d) latissimus dorsi – dorsal scapular nerve e) trapezius – accessory nerve 6) Which muscle does not extend from the posterior surface of the scapula to the greater tubercle of the humerus? a) teres major b) infraspinatus c) supraspinatus d) teres minor 7) With regard to action, which muscle is the odd one out? a) teres -

Unilateral Intercordal Neural Communication Coexistent with Variant Branching Pattern of Posterior Cord of Brachial Plexus
CAse reporT Unilateral intercordal neUral commUnication coexistent with variant branching pattern of posterior cord of brachial plexUs Renu Baliyan, Vandana Mehta, Jyoti Arora, Ashish Kr. Nayyar, R. K. Suri, Gaytri Rath Department of Anatomy, Vardhman Mahavir Medical College, New Delhi, India Summary: Variant branching pattern of the cords of brachial plexus coupled with erroneous communications has been an area of concern for surgeons opting to explore this region. Anaesthetic blocks and surgical approaches are the highlights of these interventions, where a keen familiarization of the anatomy of this region is mandatory. The present case description reports a unilateral variant branching pattern of the posterior cord coexistent with a neural communication between lateral and medial cords in an adult male cadaver. This intercordal neural communication between lateral and medial cords was oriented obliquely and measured 2.2 cm in length. Furthermore, the posterior cord revealed a variant branching pattern. It branched into three upper subscapular nerves and a common trunk for the thoracodorsal and lower subscapular nerves. The lowest of the three upper subscapular nerves gave a communicating twig to the thoracodorsal nerve. Inspite of uncount- able reports on variations of brachial plexus, descriptions regarding anomalous branching patterns hold enormous clinical significance for the radiologists, anesthetists and surgeons, besides being of academic interest for the anatomists. Key words: Posterior cord; Medial cord; Lateral cord; Neural communication introduction along with an intercordal neural communication between medial and lateral cords of brachial plexus. The hallmark of the axillary region is the brachial plexus, which is a plexiform arrangement of the anterior primary case report rami of the lowest 4 cervical and first thoracic spinal nerves. -

Hand and Foot Musculature of Anura: Structure, Homology, Terminology, and Synapomorphies for Major Clades
HAND AND FOOT MUSCULATURE OF ANURA: STRUCTURE, HOMOLOGY, TERMINOLOGY, AND SYNAPOMORPHIES FOR MAJOR CLADES BORIS L. BLOTTO, MARTÍN O. PEREYRA, TARAN GRANT, AND JULIÁN FAIVOVICH BULLETIN OF THE AMERICAN MUSEUM OF NATURAL HISTORY HAND AND FOOT MUSCULATURE OF ANURA: STRUCTURE, HOMOLOGY, TERMINOLOGY, AND SYNAPOMORPHIES FOR MAJOR CLADES BORIS L. BLOTTO Departamento de Zoologia, Instituto de Biociências, Universidade de São Paulo, São Paulo, Brazil; División Herpetología, Museo Argentino de Ciencias Naturales “Bernardino Rivadavia”–CONICET, Buenos Aires, Argentina MARTÍN O. PEREYRA División Herpetología, Museo Argentino de Ciencias Naturales “Bernardino Rivadavia”–CONICET, Buenos Aires, Argentina; Laboratorio de Genética Evolutiva “Claudio J. Bidau,” Instituto de Biología Subtropical–CONICET, Facultad de Ciencias Exactas Químicas y Naturales, Universidad Nacional de Misiones, Posadas, Misiones, Argentina TARAN GRANT Departamento de Zoologia, Instituto de Biociências, Universidade de São Paulo, São Paulo, Brazil; Coleção de Anfíbios, Museu de Zoologia, Universidade de São Paulo, São Paulo, Brazil; Research Associate, Herpetology, Division of Vertebrate Zoology, American Museum of Natural History JULIÁN FAIVOVICH División Herpetología, Museo Argentino de Ciencias Naturales “Bernardino Rivadavia”–CONICET, Buenos Aires, Argentina; Departamento de Biodiversidad y Biología Experimental, Facultad de Ciencias Exactas y Naturales, Universidad de Buenos Aires, Buenos Aires, Argentina; Research Associate, Herpetology, Division of Vertebrate Zoology, American -

GALEN on Anatomical Procedures
GALEN On Anatomical Procedures TRANSLATION WITH INTRODUCTION AND NOTES BY CHARLES SINGER Until recent years the works of Galen, the greatest and most prolific medical writer of antiquity, were closed books to the modern reader. Professor Singer has now added another to the very few works of Galen which have been translated from the Greek into English. Galen's work entitled De anatomicis administrationihus is the text of lectures on anatomy delivered in Rome about a.d. 177. The Greek text was translated into Latin in 153 1, and in this form the work had a profound influence on Vesalius and other great Renaissance anatomists. Although Galen had some knowledge ofhuman anatomy, especially of the bones, most of his dis^ section was done on the Rhesus monkey and the Barbary ape, in which many parts show marked differences from their human counterparts. Professor Singer has not only provided a scholarly translation of Galen's text, but he has also identic fied wherever possible the structures men^ tioned, and has attached to them their modern anatomical names. The book provides a basis for the study ofthe sources available for the foundation of modern anatomy. The dissection scene on the front of this jacket illustrates Galen demonstrating on a pig. Itjirst appeared on the title page of the Giunta edition of Galen s Works, Venice 1541-2. ^js. 6d. net Digitized by tlie Internet Arcliive in 2014 Iittps://arcliive.org/details/b20457194 PUBLICATIONS OF THE WELLCOME HISTORICAL MEDICAL MUSEUM NEW SERIES, NO. 7 GALEN ON ANATOMICAL PROCEDURES PUBLICATIONS OF THE WELLCOME HISTORICAL MEDICAL MUSEUM NEW SERIES {General Editor: Dr. -

Axillary Brachial Plexus Block: Landmark Techniques
AXILLARY BRACHIAL PLEXUS BLOCK LANDMARK TECHNIQUES TUTORIAL OF THE WEEK 165 11TH JANUARY 2010 Dr Z Harclerode, Dr S Michael Northern General Hospital, Sheffield, UK Correspondence to [email protected] QUESTIONS Before continuing, try to answer the following questions. The answers can be found at the end of the article, together with an explanation. 1. Which of the following statements is correct? a. The median nerve is outside the axillary sheath and is easily missed b. The brachial plexus is formed from the nerve roots of C3-T1 c. The cords are named according to their arrangement around the axillary artery d. The ulnar nerve supplies the extensor muscles of the hand and forearm 2. Name three absolute contraindications to performing an axillary plexus block 3. Which of the following statements is false? a. When using a peripheral nerve stimulator, intraneural injection is reduced by lack of motor response at 0.3mA b. A multiple stimulation technique has a higher success rate for axillary blocks than a single stimulation technique c. Blocking the intercostobrachial nerve can decrease upper limb tourniquet pain d. 0.375% Bupivacaine can give analgesia for up to 14-16 hours. INTRODUCTION The axillary brachial plexus block is a popular nerve block for forearm, wrist and hand surgery. It can be used to provide regional anaesthesia or as an analgesic technique to be used in combination with general anaesthesia. It has the advantage of being performed away from the pleura and neuraxial structures. The block was first described in New York in 1884 by Halstead, being performed using cocaine under direct vision of the plexus.