Peripheral Nerves and Plexus. Questions. Questions 1 – 12
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Gross Anatomy
www.BookOfLinks.com THE BIG PICTURE GROSS ANATOMY www.BookOfLinks.com Notice Medicine is an ever-changing science. As new research and clinical experience broaden our knowledge, changes in treatment and drug therapy are required. The authors and the publisher of this work have checked with sources believed to be reliable in their efforts to provide information that is complete and generally in accord with the standards accepted at the time of publication. However, in view of the possibility of human error or changes in medical sciences, neither the authors nor the publisher nor any other party who has been involved in the preparation or publication of this work warrants that the information contained herein is in every respect accurate or complete, and they disclaim all responsibility for any errors or omissions or for the results obtained from use of the information contained in this work. Readers are encouraged to confirm the infor- mation contained herein with other sources. For example and in particular, readers are advised to check the product information sheet included in the package of each drug they plan to administer to be certain that the information contained in this work is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. This recommendation is of particular importance in connection with new or infrequently used drugs. www.BookOfLinks.com THE BIG PICTURE GROSS ANATOMY David A. Morton, PhD Associate Professor Anatomy Director Department of Neurobiology and Anatomy University of Utah School of Medicine Salt Lake City, Utah K. Bo Foreman, PhD, PT Assistant Professor Anatomy Director University of Utah College of Health Salt Lake City, Utah Kurt H. -

Infraclavicular Topography of the Brachial Plexus Fascicles in Different Upper Limb Positions
Int. J. Morphol., 34(3):1063-1068, 2016. Infraclavicular Topography of the Brachial Plexus Fascicles in Different Upper Limb Positions Topografía Infraclavicular de los Fascículos del Plexo Braquial en Diferentes Posiciones del Miembro Superior Daniel Alves dos Santos*; Amilton Iatecola*; Cesar Adriano Dias Vecina*; Eduardo Jose Caldeira**; Ricardo Noboro Isayama**; Erivelto Luis Chacon**; Marianna Carla Alves**; Evanisi Teresa Palomari***; Maria Jose Salete Viotto**** & Marcelo Rodrigues da Cunha*,** ALVES DOS SANTOS, D.; IATECOLA, A.; DIAS VECINA, C. A.; CALDEIRA, E. J.; NOBORO ISAYAMA, R.; CHACON, E. L.; ALVES, M. C.; PALOMARI, E. T.; SALETE VIOTTO, M. J. & RODRIGUES DA CUNHA, M. Infraclavicular topography of the brachial plexus fascicles in different upper limb positions. Int. J. Morphol., 34 (3):1063-1068, 2016. SUMMARY: Brachial plexus neuropathies are common complaints among patients seen at orthopedic clinics. The causes range from traumatic to occupational factors and symptoms include paresthesia, paresis, and functional disability of the upper limb. Treatment can be surgical or conservative, but detailed knowledge of the brachial plexus is required in both cases to avoid iatrogenic injuries and to facilitate anesthetic block, preventing possible vascular punctures. Therefore, the objective of this study was to evaluate the topography of the infraclavicular brachial plexus fascicles in different upper limb positions adopted during some clinical procedures. A formalin- preserved, adult, male cadaver was used. The infraclavicular and axillary regions were dissected and the distance of the brachial plexus fascicles from adjacent bone structures was measured. No anatomical variation in the formation of the brachial plexus was observed. The metric relationships between the brachial plexus and adjacent bone prominences differed depending on the degree of shoulder abduction. -
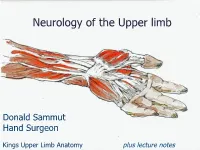
Neurology of the Upper Limb
Neurology of the Upper limb Donald Sammut Hand Surgeon Kings Upper Limb Anatomy plus lecture notes The$Neck$ The$Nerve$roots$which$supply$the$Upper$Limb$are$C5$to$T1$ Pre<fixed$(C4$to$C8)$and$Post<fixed$(C6$to$T2)$plexus$not$uncommon.$ Also$common$contributions$from$C4$and$from$T2$in$a$normally$rooted$plexus.$ $ The$anterior$nerve$roots$emerge$between$the$vertebrae$and$immediately$pass$ $through$the$first$area$of$possible$compression:$ The$root$nerve$canal$is$bounded$$ Anteriorly$by$the$posterior$margin$of$the$intervertebral$disc$and$$ Posteriorly,$by$the$facet$joint$between$vertebrae.$ $ Pathology$of$the$disc,$or$joint,$or$both,$can$narrow$this$channel$and$compress$ $the$nerve$root$ The$roots$emerge$from$the$cervical$spine$into$the$plane$between$$ Scalenius$Anterior$and$Scalenius$Medius.$$ $ Scalenius*Anterior:** Origin:$Anterior$tubercles$of$Cervical$vertebae$C3$to$6$(C6$tubercle$is$the$Carotid$tubercle)$ Insertion:$The$scalene$tubercle$on$inner$border/upper$surface$1st$rib$ $ Scalenius*Medius:* Origin:$Posterior$tubercles$of$all$cervical$vertebrae$ Insertion:$Quadrangular$area$between$the$neck$and$subclavian$groove$1st$rib$ $ Exiting$from$the$Scalenes,$the$trunks$lie$in$the$posterior$triangle$of$the$neck.$ The$posterior$triangle$is$bounded$anteriorly$by$SternoCleidoMastoid$and$$ posteriorly$by$the$Trapezius.$ The$inferior$border$is$the$clavicle$.$ The$apex$of$the$triangle$superiorly$is$at$the$back$of$the$skull$on$the$superior$nuchal$line$ $ $ The$Posterior$Triangle$ SternoCleidoMastoid$ Trapezius$ Scalenius$Medius$ Scalenius$Anterior$ -

Systemic Lupus Erythematosus Presenting with Finger Drop
DOI: 10.7860/JCDR/2018/36196.12107 Case Report Systemic Lupus Erythematosus Section Presenting with Finger Drop Internal Medicine MARJAN RAHIMI FARAHANI1, SAMIRA ALESAEIDI2 ABSTRACT Systemic Lupus Erythematosus (SLE) is an autoimmune disease with multiple organ involvement that can affect joints, skin, heart, lungs, kidneys and nervous system. SLE is a multisystem disorder resulting from abnormal immunological function. SLE affects women more than men. It affects both the central and the peripheral nervous system. Severe acute peripheral neuropathy in SLE is quite rare and it is always accompanied by evidence of active disease in other organs, including the central nervous system. The recognition of neurologic symptoms in SLE remains a clinical problem for physicians. Neurological manifestations are frequently present in SLE patients, although the peripheral nervous system involvement is rarer than the central one. Peripheral neuropathy is a known but uncommon presentation of SLE and the aim of this study is to report various forms of lupus-related neuropathies that may present as finger drop and discusses one of the rare neurological manifestations of lupus which remains a diagnostic challenge. Keywords: Autoimmune diseases, Nervous system, Pathology CASE REPORT A 33-year-old female was referred to the hospital with a chief compliant of symmetric finger drop of second, third and fourth fingers without any wrist drop for nine months before. She was able to use her fists but she had limitation on abduction of all fingers and also full extension of metacarpophalangeal and interphalangeal joints. The evaluation of sensation and reflexes were normal. The patient complained of shoulder, wrist, interphalangeal, knee, and elbow and ankle arthralgia. -

Anatomical, Clinical, and Electrodiagnostic Features of Radial Neuropathies
Anatomical, Clinical, and Electrodiagnostic Features of Radial Neuropathies a, b Leo H. Wang, MD, PhD *, Michael D. Weiss, MD KEYWORDS Radial Posterior interosseous Neuropathy Electrodiagnostic study KEY POINTS The radial nerve subserves the extensor compartment of the arm. Radial nerve lesions are common because of the length and winding course of the nerve. The radial nerve is in direct contact with bone at the midpoint and distal third of the humerus, and therefore most vulnerable to compression or contusion from fractures. Electrodiagnostic studies are useful to localize and characterize the injury as axonal or demyelinating. Radial neuropathies at the midhumeral shaft tend to have good prognosis. INTRODUCTION The radial nerve is the principal nerve in the upper extremity that subserves the extensor compartments of the arm. It has a long and winding course rendering it vulnerable to injury. Radial neuropathies are commonly a consequence of acute trau- matic injury and only rarely caused by entrapment in the absence of such an injury. This article reviews the anatomy of the radial nerve, common sites of injury and their presentation, and the electrodiagnostic approach to localizing the lesion. ANATOMY OF THE RADIAL NERVE Course of the Radial Nerve The radial nerve subserves the extensors of the arms and fingers and the sensory nerves of the extensor surface of the arm.1–3 Because it serves the sensory and motor Disclosures: Dr Wang has no relevant disclosures. Dr Weiss is a consultant for CSL-Behring and a speaker for Grifols Inc. and Walgreens. He has research support from the Northeast ALS Consortium and ALS Therapy Alliance. -
Brachial Plexus and Branches Axillary A
Regional Anatomy of the Upper Limb 1 Wu Genghua Medical College Yangzhou University Anterior surface of the •Incisions: Upper Limb Make the skin incisions indicated in figure and reflect the skin flaps. Be careful not to cut too deep. As you remove the skin, look for the cephalic v., basilic v. and median cubital v. Superficial veins and nerves Mamma Structures Contains skin, mammary glands and adipose tissue Consists of 15 to 20 Lobes of mammary gland that radiate outward from the nipple lactiferous duct lactiferous sinuse Suspensory ligaments of breast (cooper’s ligaments): connective tissue septa that extend from the skin to the deep fascia Pectoral Region Superficial structures Superficial n. Supraclavicular n. Anterior cutaneous branches of intercostal n. lateral cutaneous branches of intercostal n. Muscles connecting the upper limb to the thoracic wall Pectoralis major 胸大肌 Subclevius 锁骨下肌 Pectoralis minor 胸小肌 Serratus anterior 前锯肌 Pectoral Region Deep structures clavipectoral fascia The deep fascia which extends between subclavius, coracoid process and pectoralis minor muscles The structures pass through the clavipectoral fascia . Cephalic v. Thoracoacromial a. Lateral pectoral n. Axillary region 腋区 Boundaries of the axillary fossa Apex is bounded by Middle 1/3 of clavicle Lateral border of first rib Upper border of the scapula Base is formed by the skin stretching between the anterior and posterior walls Anterior wall Formed by pectoralis major, pectoralis minor and subclavius muscles Boundaries of the axillary fossa The posterior wall latissimus dorsi teres major subscapularis and scapula Trilateral and quadrilateral space The posterior humeral circumflex a. and axillary n. pass through the quadrilateral foramen. -

Examination of the Shoulder Bruce S
Examination of the Shoulder Bruce S. Wolock, MD Towson Orthopaedic Associates 3 Joints, 1 Articulation 1. Sternoclavicular 2. Acromioclavicular 3. Glenohumeral 4. Scapulothoracic AC Separation Bony Landmarks 1. Suprasternal notch 2. Sternoclavicular joint 3. Coracoid 4. Acromioclavicular joint 5. Acromion 6. Greater tuberosity of the humerus 7. Bicipital groove 8. Scapular spine 9. Scapular borders-vertebral and lateral Sternoclavicular Dislocation Soft Tissues 1. Rotator Cuff 2. Subacromial bursa 3. Axilla 4. Muscles: a. Sternocleidomastoid b. Pectoralis major c. Biceps d. Deltoid Congenital Absence of Pectoralis Major Pectoralis Major Rupture Soft Tissues (con’t) e. Trapezius f. Rhomboid major and minor g. Latissimus dorsi h. Serratus anterior Range of Motion: Active and Passive 1. Abduction - 90 degrees 2. Adduction - 45 degrees 3. Extension - 45 degrees 4. Flexion - 180 degrees 5. Internal rotation – 90 degrees 6. External rotation – 45 degrees Muscle Testing 1. Flexion a. Primary - Anterior deltoid (axillary nerve, C5) - Coracobrachialis (musculocutaneous nerve, C5/6 b. Secondary - Pectoralis major - Biceps Biceps Rupture- Longhead Muscle Testing 2. Extension a. Primary - Latissimus dorsi (thoracodorsal nerve, C6/8) - Teres major (lower subscapular nerve, C5/6) - Posterior deltoid (axillary nerve, C5/6) b. Secondary - Teres minor - Triceps Abduction Primary a. Middle deltoid (axillary nerve, C5/6) b. Supraspinatus (suprascapular nerve, C5/6) Secondary a. Anterior and posterior deltoid b. Serratus anterior Deltoid Ruputure Axillary Nerve Palsy Adduction Primary a. Pectoralis major (medial and lateral pectoral nerves, C5-T1 b. Latissimus dorsi (thoracodorsal nerve, C6/8) Secondary a. Teres major b. Anterior deltoid External Rotation Primary a. Infraspinatus (suprascapular nerve, C5/6) b. Teres minor (axillary nerve, C5) Secondary a. -

Stichting Voor Ooglijders Prof. Dr. HJ
De publicatie van dit proefschrift werd mede mogelijk gemaakt met fmanciele steun van: Stichting voor Ooglijders Prof. Dr. H.J. Flieringa Stichting Medical Workshop BV Kabi Pharmacia Bournonville-Pharma BV Ter herinnering aan mijn vader Omslag: Henry Cannon I Ebbo Clerlo: CLINICAL ASPECTS AND ETIOLOGY OF FUCHS' HETEROCHROMIC CYCLITIS (KLINISCHE ASPECTEN EN ETIOLOGIE VAN DE HETEROCHROME CYCLITIS VAN FUCHS) proefschrift Ter verkrijging van de graad van doctor aan de Erasmus Universiteit Rotterdam op gezag van de Rector Magnificus Prof. dr. P.W.C. Akkermans M. Lit. en volgens besluit van het College van Dekanen. De openbare verdediding zal plaatsvinden op woensdag 3 November 1993 om 15.45 uur. door Ellen Carolien La Heij geboren te Arnstelveen PROMOTIE-COMMISSIE PROMOTORES' Prof. dr. P.T.V.M. de Jong Prof. dr. A. Kijlstra OVERIGE LEDEN, Prof. dr. F.T. Bosman Prof. dr. H.A. Drexhage CONTENTS Chapter 1 1.1 General Introduction ........................ 7 1. 2 Aim of the Thesis_ ................... __ ...... 8 Chapter 2 Fuchs' Heterochromic Cyclitis: Review of the Literature (submitted for publication) 2.1 Historical Background ........................ 9 2.2 Terminology and Classification ............... 9 2. 3 Epidemiology. .11 2. 4 Clinical Features ........................... 11. 2.5 Histopathology of the Iris ................. 22 2. 6 Etiologic Mechanisms ........................ 25 2.7 Therapy and Prognosis .................... ... 37 Chapter 3 Clin~c~l analysis of Fuchs' heterochromic cycl1t1s ........................................ 49 (Doc Ophthalmol. 1991;78:225-235). Chapter 4 Treatment and prognosis of secondary glaucoma in Fuchs' heterochromic cyclitis ............... .... 61 (Am J Ophthalmol. 1993, in press) Chapter 5 Quantitative analysis of iris translucency in Fuchs' heterochromic cyclitis ................. .. 83 (Invest Ophthalmol & Vis Sci. -

Orphanet Report Series Rare Diseases Collection
Marche des Maladies Rares – Alliance Maladies Rares Orphanet Report Series Rare Diseases collection DecemberOctober 2013 2009 List of rare diseases and synonyms Listed in alphabetical order www.orpha.net 20102206 Rare diseases listed in alphabetical order ORPHA ORPHA ORPHA Disease name Disease name Disease name Number Number Number 289157 1-alpha-hydroxylase deficiency 309127 3-hydroxyacyl-CoA dehydrogenase 228384 5q14.3 microdeletion syndrome deficiency 293948 1p21.3 microdeletion syndrome 314655 5q31.3 microdeletion syndrome 939 3-hydroxyisobutyric aciduria 1606 1p36 deletion syndrome 228415 5q35 microduplication syndrome 2616 3M syndrome 250989 1q21.1 microdeletion syndrome 96125 6p subtelomeric deletion syndrome 2616 3-M syndrome 250994 1q21.1 microduplication syndrome 251046 6p22 microdeletion syndrome 293843 3MC syndrome 250999 1q41q42 microdeletion syndrome 96125 6p25 microdeletion syndrome 6 3-methylcrotonylglycinuria 250999 1q41-q42 microdeletion syndrome 99135 6-phosphogluconate dehydrogenase 67046 3-methylglutaconic aciduria type 1 deficiency 238769 1q44 microdeletion syndrome 111 3-methylglutaconic aciduria type 2 13 6-pyruvoyl-tetrahydropterin synthase 976 2,8 dihydroxyadenine urolithiasis deficiency 67047 3-methylglutaconic aciduria type 3 869 2A syndrome 75857 6q terminal deletion 67048 3-methylglutaconic aciduria type 4 79154 2-aminoadipic 2-oxoadipic aciduria 171829 6q16 deletion syndrome 66634 3-methylglutaconic aciduria type 5 19 2-hydroxyglutaric acidemia 251056 6q25 microdeletion syndrome 352328 3-methylglutaconic -

M1 – Muscled Arm
M1 – Muscled Arm See diagram on next page 1. tendinous junction 38. brachial artery 2. dorsal interosseous muscles of hand 39. humerus 3. radial nerve 40. lateral epicondyle of humerus 4. radial artery 41. tendon of flexor carpi radialis muscle 5. extensor retinaculum 42. median nerve 6. abductor pollicis brevis muscle 43. flexor retinaculum 7. extensor carpi radialis brevis muscle 44. tendon of palmaris longus muscle 8. extensor carpi radialis longus muscle 45. common palmar digital nerves of 9. brachioradialis muscle median nerve 10. brachialis muscle 46. flexor pollicis brevis muscle 11. deltoid muscle 47. adductor pollicis muscle 12. supraspinatus muscle 48. lumbrical muscles of hand 13. scapular spine 49. tendon of flexor digitorium 14. trapezius muscle superficialis muscle 15. infraspinatus muscle 50. superficial transverse metacarpal 16. latissimus dorsi muscle ligament 17. teres major muscle 51. common palmar digital arteries 18. teres minor muscle 52. digital synovial sheath 19. triangular space 53. tendon of flexor digitorum profundus 20. long head of triceps brachii muscle muscle 21. lateral head of triceps brachii muscle 54. annular part of fibrous tendon 22. tendon of triceps brachii muscle sheaths 23. ulnar nerve 55. proper palmar digital nerves of ulnar 24. anconeus muscle nerve 25. medial epicondyle of humerus 56. cruciform part of fibrous tendon 26. olecranon process of ulna sheaths 27. flexor carpi ulnaris muscle 57. superficial palmar arch 28. extensor digitorum muscle of hand 58. abductor digiti minimi muscle of hand 29. extensor carpi ulnaris muscle 59. opponens digiti minimi muscle of 30. tendon of extensor digitorium muscle hand of hand 60. superficial branch of ulnar nerve 31. -

Dorsal Scapular Nerve Neuropathy: a Narrative Review of the Literature Brad Muir, Bsc.(Hons), DC, FRCCSS(C)1
ISSN 0008-3194 (p)/ISSN 1715-6181 (e)/2017/128–144/$2.00/©JCCA 2017 Dorsal scapular nerve neuropathy: a narrative review of the literature Brad Muir, BSc.(Hons), DC, FRCCSS(C)1 Objective: The purpose of this paper is to elucidate Objectif : Ce document a pour objectif d’élucider this little known cause of upper back pain through a cette cause peu connue de douleur dans le haut du narrative review of the literature and to discuss the dos par un examen narratif de la littérature, ainsi que possible role of the dorsal scapular nerve (DSN) in de discuter du rôle possible du nerf scapulaire dorsal the etiopathology of other similar diagnoses in this (NSD) dans l’étiopathologie d’autres diagnostics area including cervicogenic dorsalgia (CD), notalgia semblables dans ce domaine, y compris la dorsalgie paresthetica (NP), SICK scapula and a posterolateral cervicogénique (DC), la notalgie paresthésique (NP), arm pain pattern. l’omoplate SICK et un schéma de douleur postéro- Background: Dorsal scapular nerve (DSN) latérale au bras. neuropathy has been a rarely thought of differential Contexte : La neuropathie du nerf scapulaire dorsal diagnosis for mid scapular, upper to mid back and (NSD) constitue un diagnostic différentiel rare pour la costovertebral pain. These are common conditions douleur mi-scapulaire, costo-vertébrale et au bas/haut presenting to chiropractic, physiotherapy, massage du dos. Il s’agit de troubles communs qui surgissent therapy and medical offices. dans les cabinets de chiropratique, de physiothérapie, de Methods: The methods used to gather articles for this massothérapie et de médecin. paper included: searching electronic databases; and Méthodologie : Les méthodes utilisées pour hand searching relevant references from journal articles rassembler les articles de ce document comprenaient la and textbook chapters. -

Anatomy, Shoulder and Upper Limb, Arm Quadrangular Space
NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Anatomy, Shoulder and Upper Limb, Arm Quadrangular Space Authors Irfan A. Khan1; Matthew Varacallo2. Affiliations 1 Florida International University 2 Department of Orthopaedic Surgery, University of Kentucky School of Medicine Last Update: December 21, 2018. Introduction The quadrangular (or quadrilateral) space (QS) is named based on the shape of its anatomic boundaries. Located along the posterolateral shoulder, the QS serves as a passageway for the axillary nerve and posterior humeral circumflex artery (PHCA). Quadrangular (or quadrilateral) space syndrome (QSS) can occur secondary to various compressive pathologies. Although the incidence of such pathologies is rare, QSS has a known predilection for subgroups of athletic populations and can often suffer misdiagnosis or are clinically under-appreciated. Thus, clinicians should maintain a heightened clinical suspicion for QSS in patients aged 20-40 years of age presenting with a history of current contact or overhead athletic performance (e.g., baseball pitchers, swimmers, etc.), [1][2] or overhead laborers secondary to repetitive stress mechanics on the shoulder.[3] Structure and Function The QS has four anatomic borders; the teres minor superiorly, the inferior border is the teres major muscle, the medial boundary is the long head of the triceps brachii muscle, and the humeral surgical neck forms the lateral bound. The QS functions as a passageway for the axillary nerve, and the posterior humeral circumflex artery (PHCA).[3] The latter provides the primary (two-thirds) of the blood supply to the humeral head.[4] Blood Supply and Lymphatics The posterior humeral circumflex artery (PHCA) within the quadrangular space originates from the axillary artery, and within the QS, the PHCA divides into anterior and posterior branches.