Paramedian Mandibular Cleft in a Patient Who Also Had Goldenhar 2
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Is the Skeleton Male Or Female? the Pelvis Tells the Story
Activity: Is the Skeleton Male or Female? The pelvis tells the story. Distinct features adapted for childbearing distinguish adult females from males. Other bones and the skull also have features that can indicate sex, though less reliably. In young children, these sex-related features are less obvious and more difficult to interpret. Subtle sex differences are detectable in younger skeletons, but they become more defined following puberty and sexual maturation. What are the differences? Compare the two illustrations below in Figure 1. Female Pelvic Bones Male Pelvic Bones Broader sciatic notch Narrower sciatic notch Raised auricular surface Flat auricular surface Figure 1. Female and male pelvic bones. (Source: Smithsonian Institution, illustrated by Diana Marques) Figure 2. Pelvic bone of the skeleton in the cellar. (Source: Smithsonian Institution) Skull (Cranium and Mandible) Male Skulls Generally larger than female Larger projections behind the Larger brow ridges, with sloping, ears (mastoid processes) less rounded forehead Square chin with a more vertical Greater definition of muscle (acute) angle of the jaw attachment areas on the back of the head Figure 3. Male skulls. (Source: Smithsonian Institution, illustrated by Diana Marques) Female Skulls Smoother bone surfaces where Smaller projections behind the muscles attach ears (mastoid processes) Less pronounced brow ridges, Chin more pointed, with a larger, with more vertical forehead obtuse angle of the jaw Sharp upper margins of the eye orbits Figure 4. Female skulls. (Source: Smithsonian Institution, illustrated by Diana Marques) What Do You Think? Comparing the skull from the cellar in Figure 5 (below) with the illustrated male and female skulls in Figures 3 and 4, write Male or Female to note the sex depicted by each feature. -

The Cat Mandible (II): Manipulation of the Jaw, with a New Prosthesis Proposal, to Avoid Iatrogenic Complications
animals Review The Cat Mandible (II): Manipulation of the Jaw, with a New Prosthesis Proposal, to Avoid Iatrogenic Complications Matilde Lombardero 1,*,† , Mario López-Lombardero 2,†, Diana Alonso-Peñarando 3,4 and María del Mar Yllera 1 1 Unit of Veterinary Anatomy and Embryology, Department of Anatomy, Animal Production and Clinical Veterinary Sciences, Faculty of Veterinary Sciences, Campus of Lugo—University of Santiago de Compostela, 27002 Lugo, Spain; [email protected] 2 Engineering Polytechnic School of Gijón, University of Oviedo, 33203 Gijón, Spain; [email protected] 3 Department of Animal Pathology, Faculty of Veterinary Sciences, Campus of Lugo—University of Santiago de Compostela, 27002 Lugo, Spain; [email protected] 4 Veterinary Clinic Villaluenga, calle Centro n◦ 2, Villaluenga de la Sagra, 45520 Toledo, Spain * Correspondence: [email protected]; Tel.: +34-982-822-333 † Both authors contributed equally to this manuscript. Simple Summary: The small size of the feline mandible makes its manipulation difficult when fixing dislocations of the temporomandibular joint or mandibular fractures. In both cases, non-invasive techniques should be considered first. When not possible, fracture repair with internal fixation using bone plates would be the best option. Simple jaw fractures should be repaired first, and caudal to rostral. In addition, a ventral approach makes the bone fragments exposure and its manipulation easier. However, the cat mandible has little space to safely place the bone plate screws without damaging the tooth roots and/or the mandibular blood and nervous supply. As a consequence, we propose a conceptual model of a mandibular prosthesis that would provide biomechanical Citation: Lombardero, M.; stabilization, avoiding any unintended (iatrogenic) damage to those structures. -

Craniofacial Development After Three Different Palatoplasties in Children Born with Isolated Cleft Palate
From the DEPARTMENT OF DENTAL MEDICINE Karolinska Institutet, Stockholm, Sweden CRANIOFACIAL DEVELOPMENT AFTER THREE DIFFERENT PALATOPLASTIES IN CHILDREN BORN WITH ISOLATED CLEFT PALATE Konstantinos A. Parikakis Stockholm 2018 All previously published papers were reproduced with permission from the publisher Published by Karolinska Institutet Printed by Eprint AB 2018 © Konstantinos A. Parikakis, 2018 ISBN 978-91-7831-277-1 Craniofacial development after three different palatoplasties in children born with isolated cleft palate THESIS FOR DOCTORAL DEGREE (Ph.D.) By Konstantinos A. Parikakis Principal Supervisor: Opponent: Associate Professor Agneta Karsten Professor David Rice Karolinska Institutet University of Helsinki Department of Dental Medicine Department of Orthodontics Division of Orthodontics and Pedodontics Examination Board: Co-supervisor(s): Associate Professor Magnus Becker Associate Professor Ola Larson University of Lund Karolinska University Hospital Department of Plastic and Reconstructive Surgery Department of Reconstructive Plastic Surgery Professor Britt Gustafsson Karolinska Institutet Department of Clinical Science, Intervention and Technology (CLINTEC) Division of Pediatrics Associate Professor Farhan Bazargani University of Örebro Centrum för Specialisttandvard Department of Orthodontics To Christina, little Anastasios and…forthcoming Vassilios “Wherever the art of Medicine is loved, there is also a love of Humanity” Hippocrates of Kos, c.460-370 B.C. ABSTRACT Introduction: Different palatoplasties are applied for -

Results Description of the SKULLS. the Overall Size of Both Skulls Was Considered to Be Within Normal Limits for Their Ethnic
Ossification Defects and Craniofacial Morphology In Incomplete Forms of Mandibulofacial Dysostosis A Description of Two Dry Skulls ERIK DAHL, D.D.S., DR. ODONT. ARNE BJORK, D.D.S., ODONT. DR. Copenhagen, Denmark The morphology of two East Indian dry skulls exhibiting anomalies which were suggested to represent incomplete forms of mandibulofacial dysostosis is described. Obvious although minor ossification anomalies were found localized to the temporal, sphenoid, the zygomatic, the maxillary and the mandibular bones. The observations substantiate the concept of the regional and bilateral nature of this malformation syndrome. Bilateral orbital deviations, hypoplasia of the malar bones, and incomplete zygomatic arches appear to be hard tissue aberrations which may be helpful in exami- nation for subclinical carrier status. Changes in mandibular morphology seem to be less distinguishing features in incomplete or abortive types of mandibulofacial dysostosis. KEY WORDS craniofacial problems, mandible, mandibulofacial dysostosis, maxilla, sphenoid bone, temporal bone, zygomatic bone Mandibulofacial dysostosis (MFD) often roentgencephalometric examinations were results in the development of a characteristic made of the skulls, and tomograms were ob- facial disfigurement with considerable simi- tained of the internal and middle ear. Com- larity between affected individuals. However, parisons were made with normal adult skulls the symptoms may vary highly in respect to and with an adult skull exhibiting the char- type and degree, and both incomplete and acteristics of MFD. All of the skulls were from abortive forms of the syndrome have been the same ethnic group. ' reported in the literature (Franceschetti and Klein, 1949; Moss et al., 1964; Rogers, 1964). Results In previous papers, we have shown the DEsCRIPTION OF THE SKULLS. -

GLOSSARY of MEDICAL and ANATOMICAL TERMS
GLOSSARY of MEDICAL and ANATOMICAL TERMS Abbreviations: • A. Arabic • abb. = abbreviation • c. circa = about • F. French • adj. adjective • G. Greek • Ge. German • cf. compare • L. Latin • dim. = diminutive • OF. Old French • ( ) plural form in brackets A-band abb. of anisotropic band G. anisos = unequal + tropos = turning; meaning having not equal properties in every direction; transverse bands in living skeletal muscle which rotate the plane of polarised light, cf. I-band. Abbé, Ernst. 1840-1905. German physicist; mathematical analysis of optics as a basis for constructing better microscopes; devised oil immersion lens; Abbé condenser. absorption L. absorbere = to suck up. acervulus L. = sand, gritty; brain sand (cf. psammoma body). acetylcholine an ester of choline found in many tissue, synapses & neuromuscular junctions, where it is a neural transmitter. acetylcholinesterase enzyme at motor end-plate responsible for rapid destruction of acetylcholine, a neurotransmitter. acidophilic adj. L. acidus = sour + G. philein = to love; affinity for an acidic dye, such as eosin staining cytoplasmic proteins. acinus (-i) L. = a juicy berry, a grape; applied to small, rounded terminal secretory units of compound exocrine glands that have a small lumen (adj. acinar). acrosome G. akron = extremity + soma = body; head of spermatozoon. actin polymer protein filament found in the intracellular cytoskeleton, particularly in the thin (I-) bands of striated muscle. adenohypophysis G. ade = an acorn + hypophyses = an undergrowth; anterior lobe of hypophysis (cf. pituitary). adenoid G. " + -oeides = in form of; in the form of a gland, glandular; the pharyngeal tonsil. adipocyte L. adeps = fat (of an animal) + G. kytos = a container; cells responsible for storage and metabolism of lipids, found in white fat and brown fat. -

Craniofacial Center
Craniofacial Center The team concept The Craniofacial Center at Children’s Hospital New Orleans is dedicated to providing holistic, coordinated, state-of-the-art care to children with craniofacial differences. All team members specialize in complexities of caring for children with clefts and other craniofacial conditions. Children with clefts and craniofacial differences thrive best when cared for by specialists from many different disciplines. The team approach ensures that healthcare providers work together to implement a single, coordinated, and patient-centered treatment plan unique to your child. Craniofacial Center Craniofacial Pediatrics Genetics Otolaryngology The craniofacial pediatrician will Many babies with craniofacial Our otolaryngologists are surgeons diagnose your child and manage conditions have “isolated” problems with expertise in treating disorders medical problems related to that do not affect their general of the head, neck, ears, nose and their craniofacial differences. The health. The geneticist identifies throat in children of all ages. They physician guides your child’s overall those few patients who may have a assess and monitor your child’s treatment and works with other more complicated genetic condition hearing, ears, feeding, breathing team members to coordinate associated with other medical and speech development. specialty care. Your craniofacial problems and/or family history. They pediatrician will be familiar with all can advise you about the pros and Neurosurgery aspects of your child’s condition and cons of genetic testing, counsel the Neurosurgeons specialize in treating with your family’s needs and desires. family, and give information about children with abnormalities of the The craniofacial pediatrician will the prognosis and recurrence risks. -

A Guide to Safety Protocols for International Craniofacial Outreach
CE: R.R.; SCS-20-0960; Total nos of Pages: 4; SCS-20-0960 SPECIAL EDITORIAL A Guide to Developing Safety Protocols for International Craniofacial Outreach Programs During the COVID-19 Era Parsa P. Salehi, MD,Ã Adam B. Johnson, MD, PhD,y Brian Rubinstein, MD,z Nima Pahlavan, MD, DDS,§ Babak Azizzadeh, MD, FACS,jj and Usama S. Hamdan, MDô procedures to the ‘‘new normal.’’ One important area of health 07/23/2020 on BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AWnYQp/IlQrHD3yRlXg5VZA8ta0m8jqCQrWIIm7WEcSSNRoQmV8QkFTwQ= by https://journals.lww.com/jcraniofacialsurgery from Downloaded Downloaded Abstract: The ongoing COVID-19 outbreak has created obstacles to care delivery that merits attention is the future of craniofacial health care delivery on a global scale. Low- and middle-income outreach programs (CFOP) in the COVID-19 era. from countries (LMICs), many of which already suffered from unmet CFOP provide an essential service to low- and middle-income 1–3 https://journals.lww.com/jcraniofacialsurgery surgical and medical needs, are at great risk of suffering poor health countries (LMICs). Even before the COVID pandemic, the outcomes due to health care access troubles brought on by the surgical needs of LMICs were unmet by existing nongovernmental organizations (NGOs).2 Hence, the pandemic will likely exacerbate pandemic. Craniofacial outreach programs (CFOP)—a staple for 4 craniofacial surgeons—have historically provided essential care to LMICs’ surgical needs. In particular, CFOP are a staple for craniofacial surgeons (which include facial plastic and reconstruc- LMICs. To date, there has not been literature discussing the process of tive surgeons, plastic surgeons, otolaryngologists-head and neck resuming CFOP mission trips. -

Lieshout Van Lieshout, M.J.S
EXPLORING ROBIN SEQUENCE Manouk van Lieshout Van Lieshout, M.J.S. ‘Exploring Robin Sequence’ Cover design: Iliana Boshoven-Gkini - www.agilecolor.com Thesis layout and printing by: Ridderprint BV - www.ridderprint.nl ISBN: 978-94-6299-693-9 Printing of this thesis has been financially supported by the Erasmus University Rotterdam. Copyright © M.J.S. van Lieshout, 2017, Rotterdam, the Netherlands All rights reserved. No parts of this thesis may be reproduced, stored in a retrieval system, or transmitted in any form or by any means without permission of the author or when appropriate, the corresponding journals Exploring Robin Sequence Verkenning van Robin Sequentie Proefschrift ter verkrijging van de graad van doctor aan de Erasmus Universiteit Rotterdam op gezag van de rector magnificus Prof.dr. H.A.P. Pols en volgens besluit van het College voor Promoties. De openbare verdediging zal plaatsvinden op woensdag 20 september 2017 om 09.30 uur door Manouk Ji Sook van Lieshout geboren te Seoul, Korea PROMOTIECOMMISSIE Promotoren: Prof.dr. E.B. Wolvius Prof.dr. I.M.J. Mathijssen Overige leden: Prof.dr. J.de Lange Prof.dr. M. De Hoog Prof.dr. R.J. Baatenburg de Jong Copromotoren: Dr. K.F.M. Joosten Dr. M.J. Koudstaal TABLE OF CONTENTS INTRODUCTION Chapter I: General introduction 9 Chapter II: Robin Sequence, A European survey on current 37 practice patterns Chapter III: Non-surgical and surgical interventions for airway 55 obstruction in children with Robin Sequence AIRWAY OBSTRUCTION Chapter IV: Unravelling Robin Sequence: Considerations 79 of diagnosis and treatment Chapter V: Management and outcomes of obstructive sleep 95 apnea in children with Robin Sequence, a cross-sectional study Chapter VI: Respiratory distress following palatal closure 111 in children with Robin Sequence QUALITY OF LIFE Chapter VII: Quality of life in children with Robin Sequence 129 GENERAL DISCUSSION AND SUMMARY Chapter VIII: General discussion 149 Chapter IX: Summary / Nederlandse samenvatting 169 APPENDICES About the author 181 List of publications 183 Ph.D. -

Pediatric/Craniofacial
PEDIATRIC/CRANIOFACIAL Counterclockwise Craniofacial Distraction Osteogenesis for Tracheostomy-Dependent Children with Treacher Collins Syndrome Richard A. Hopper, M.D., Background: The craniofacial rotation deformity in Treacher Collins syndrome M.Sc. results in airway compression that is not addressed by isolated mandibular Hitesh Kapadia, D.D.S., distraction osteogenesis. Our purpose is to present a surgical technique— Ph.D. counterclockwise craniofacial distraction osteogenesis—that improves airway Srinivas Susarla, D.M.D., morphology and occlusal rotation in tracheostomy-dependent patients with M.D., M.P.H. this condition. Randall Bly, M.D. Methods: All patients underwent subcranial Le Fort II osteotomies with simultane- Kaalan Johnson, M.D. ous mandibular osteotomies, followed by coordinated maxillomandibular distrac- Seattle, Wash. tion with counterclockwise rotation. We reviewed pretreatment, posttreatment, and end-treatment cephalograms. Airway changes were assessed using polysom- nography, sleep endoscopy, and direct laryngoscopy. Bivariate statistics were com- puted to compare pretreatment and posttreatment measures. Results: Five subjects (age range, 4.5 to 12.1 years) underwent this new pro- cedure; three had previously undergone mandibular distraction. The average palatal plane rotation was 17 degrees, the effective mandible length increase was 18 mm, and the facial plane relative to skull base rotation was 14 degrees. There was a symmetric 30 percent relapse of rotation with maintained occlusion in the SUPPLEMENTAL DIGITAL CONTENT IS AVAIL- first 9 months of follow-up that then stabilized. Four patients were successfully ABLE IN THE TEXT. decannulated following counterclockwise craniofacial distraction osteogenesis following polysomnography. Sleep endoscopy available on two patients demon- strated resolution of the upper airway obstruction. Conclusions: Counterclockwise craniofacial distraction osteogenesis provided greater palatal rotation than previous techniques. -
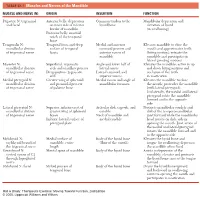
1 TABLE 23-1 Muscles and Nerves of the Mandible
0350 ch 23-Tab 10/12/04 12:19 PM Page 1 Chapter 23: The Temporomandibular Joint 1 TABLE 23-1 Muscles and Nerves of the Mandible MUSCLE AND NERVE (N) ORIGIN INSERTION FUNCTION Digastric N: trigeminal Anterior belly: depression Common tendon to the Mandibular depression and and facial on inner side of inferior hyoid bone elevation of hyoid border of mandible (in swallowing) Posterior belly: mastoid notch of the temporal bone Temporalis N: Temporal fossa and deep Medial and anterior Elevates mandible to close the mandibular division surface of temporal coronoid process and mouth and approximates teeth of trigeminal nerve fascia anterior ramus of (biting motion); retracts the mandible mandible and participates in lateral grinding motions Masseter N: Superficial: zygomatic Angle and lower half of Elevates the mandible; active in up mandibular division arch and maxillary process lateral ramus and down biting motions and of trigeminal nerve Deep portion: zygomatic Lateral coronoid and occlusion of the teeth arch superior ramus in mastication Medial pterygoid N: Greater wing of sphenoid Medial ramus and angle of Elevates the mandible to close mandibular division and pyramidal process mandibular foramen the mouth; protrudes the mandible of trigeminal nerve of palatine bone (with lateral pterygoid). Unilaterally, the medial and lateral pterygoid rotate the mandible forward and to the opposite side Lateral pterygoid N: Superior: inferior crest of Articular disk, capsule, and Protracts mandibular condyle and mandibular division greater wing of sphenoid condyle disk of the temporomandibular of trigeminal nerve bones Neck of mandible and joint forward while the mandibular Inferior: lateral surface of medial condyle head rotates on disk; aids in pterygoid plate opening the mouth. -

Illustrated Review of the Embryology and Development of the Facial
REVIEW ARTICLE Illustrated Review of the Embryology and Development of the Facial Region, Part 2: Late Development of the Fetal Face and Changes in the Face from the Newborn to Adulthood P.M. Som and T.P. Naidich ABSTRACT SUMMARY: The later embryogenesis of the fetal face and the alteration in the facial structure from birth to adulthood have been reviewed. Part 3 of the review will address the molecular mechanisms that are responsible for the changes described in parts 1 and 2. art 1 of this 3-part review primarily dealt with the early em- first make contact, each is completely covered by a homoge- Pbryologic development of the face and nasal cavity. Part 2 will neous epithelium. A special epithelium arises at the edge of discuss the later embryonic and fetal development of the face, and each palatal shelf, facilitating the eventual fusion of these changes in facial appearance from neonate to adulthood will be shelves. The epithelium on the nasal cavity surface of the palate reviewed. will differentiate into columnar ciliated epithelium. The epi- thelium on the oral cavity side of the palate will differentiate Formation of the Palate into stratified squamous epithelium. Between the sixth and 12th weeks, the palate is formed from 3 The 2 palatal shelves also fuse with the triangular primary pal- primordia: a midline median palatine process and paired lateral ate anteromedially to form a y-shaped fusion line. The point of palatine processes (Fig 1). In the beginning of the sixth week, fusion of the secondary palatal shelves with the primary palate is merging of the paired medial nasal processes forms the intermax- marked in the adult by the incisive foramen. -
Fat Grafting in Orthognathic Surgery
SPECIAL EDITORIAL Fat Grafting in Orthognathic Surgery Rajiv J. Iyengar, MD, Kyle Gabrick, MD, Karl Bruckman, MD, DDS, and Derek M. Steinbacher, MD, DMD at grafting is a powerful tool in plastic surgery. The evolution of Background: Fat grafting is widely utilized in craniofacial surgery. F this technique is fascinating and has been described exten- The authors describe a series of consecutive patients who under- sively.1 At present, the broad procedural practice standards are went orthognathic surgery with fat grafting by the senior author and derived from the work of Coleman.1–5 The so-called lipostructure review relevant literature in the field; fat grafting technique is method involves harvesting fat using a 3-mm blunt cannula with a discussed in detail. The authors also highlight 3 patients to illustrate 10 mL syringe at low negative pressure to minimize adipocyte trauma; postoperative outcomes. Coleman advocates for low RPM centrifugation which allows for Methods: A retrospective cohort of consecutive orthognathic atraumatic separation of oily,aqueous, and fat components. Placement surgery patients was reviewed. Age, sex, BMI, procedure, area then involves the use of an 18-G cannula in the recipient site. Further of harvest, location of injection, donor site complications, and need technical descriptions are included later in this manuscript. The purpose of this paper is to review the benefits of fat grafting for repeat fat grafting were analyzed. Inclusion criteria included during orthognathic surgery; more specifically, we will delineate history of orthognathic surgery and concomitant fat grafting the biology, harvesting, processing, and technical considerations to performed by the senior author in 2015.