Alpha Letter
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Corporation of the Town of Bradford West Gwillimbury Agenda Committee of the Whole Meeting C30 December 9,2008
The Corporation of the Town of Bradford West Gwillimbury Agenda Committee of the Whole Meeting C30 December 9,2008 (a) OPENING That this meeting of Committee come to order at p.m. (b) DISCLOSURE OF PECUNIARY INTEREST (c) REPORTS OF MUNICIPAL OFFICERS 1. REPORT OF THE DIRECTOR OF ENGINEERING SERVICES pgs. 5 - 12 Status Update on Phase II Water Treatment Plant Expansion in the Town of lnnisfil That Committee of the Whole recommend to Council that Report No. 016-ENG-2008 titled Status Update on Phase II Water Treatment Plant Expansion in the Town of lnnisfil be received for information. 2. REPORTS OF FINANCE DEPARTMENT 2.1 2009 lnterim Tax Levy By-law That Committee of the Whole recommend to Council that the report of the Director of Finance & Treasurer entitled "2009 lnterim Tax Levy By-law" dated December 9, 2008 be received; and That Committee of the Whole recommends to Council the adoption of the 2009 lnterim Tax Levy By-law." 2.2 Administration Fee - Ms. Palazzolo pgs. 18 - 23 That Committee of the Whole recommend to Council that the report of the Director of Finance & Treasurer entitled "Administration Fee - Ms. Palazzolo" dated December 9, 2008 be received; and That Ms. Palazzolols request to have the $25.00 administration fee waived from her tax account be denied. Committee Meetina C30 -2- December 9,2008 3. REPORTS OF PLANNING & DEVELOPMENT SERVICES DEPARTMENT 3.1 National Homes - REVISED Draft Approval of Subdivision S-06-05 pgs. 24 - 49 743 Line 8, Part of the North l/2 of Lot 13, Concession 7, Former Township of West Gwillimbury -

Edited by Denise Doherty-Delorme and Erika Shaker
MissingMissing PiecesPieces VV AN ALTERNATIVE GUIDE TO CANADIAN POST-SECONDARY EDUCATION Edited by Denise Doherty-Delorme and Erika Shaker Missing Pieces V: An Alternative Guide to Canadian Post-secondary Education i Missing Pieces V: An Alternative Guide to Canadian Post-secondary Education Edited by Erika Shaker and Denise Doherty-Delorme ISBN 0-88627-379-X August 2004 $12.00 410-75 Albert Street Ottawa, ON K1P 5E7 tel: 613-563-1341 fax: 613-233-1458 email: [email protected] http://www.policyalternatives.ca CAW 567 ii Canadian Centre for Policy Alternatives Contents Contributors ...................................................................................................................................................v Introduction................................................................................................................................................... 1 Rankings......................................................................................................................................................... 3 Overall .................................................................................................................................................................................... 3 Access ..................................................................................................................................................................................... 5 Accountability ...................................................................................................................................................................... -

Mail Boxes Etc
7ERESTILLAROUND THECORNER /URNEWADDRESSIS %DWARD3TREET 5NIT 0/"OX !URORA /.,', 4 #ALLUSFORAQUOTEORCOMEVISIT Aurora’s Community Newspaper 7% (!6% ! ()34/29 /& 02/4%#4).' 9/52 &5452% Vol. 5 No. 38 Week of July 12, 2005 905-727-3300 Now you see them... You walked on the wild side if you were part of the Aurora Garden & Horticultural Society’s garden tour Sunday and you visited Henning Malmholt’s incredible efforts on Clubine Court. A partial view of his garden is shown, inset. His was one of eight Aurora and area gardens available on the tour which attracted scores of visitors. Auroran photos by David Falconer ...now you don’t Aurora retail bustled years ago Long before the current con- first IGA store in Canada operated There was the mother and the venience store opened on there by Larry Rubin. father, sons Phil and Harvey and Wellington Street East, just east of Even earlier, the building was daughter Shirley. the bank, there was a Home once the site of a general store It was a combination grocery Hardware store but before that the operated by the Fingold family. and dry goods store with a huge opening in the wall of what was once two stores. Aurora student joins Years ago, Rolling's fruit store was across the street from the Fingold store while Joe Mitchell's Historica Fair group hardware store and Frank Teasdale's grocery store were Aurora’s Caitlin Nishimura has Purpose of the play was not located farther east on Wellington been selected to join the Ontario only to tell this story, but also allow Street. -
Year in Review
Bill 65, passed on May 10, 2000 during the 37th Session, founded the Ontario Association of Former OAFP Parliamentarians. It was the first bill in Ontario history to be introduced by a Legislative Committee. The Ontario Association of Former Parliamentarians Year in Review - 2015 page 1|InFormer Year In Review 2015 Bill 65, passed on May 10, 2000 during the 37th Session, founded the Ontario Association of Former OAFP Parliamentarians. It was the first bill in Ontario history to be introduced by a Legislative Committee. Our Colleagues Who Passed Away in 2015 They served their constituents, their Party and their Province Eric Gordon Cunningham (April 14, 1949 – January 1, 2015) Liberal, Wentworth North 1975 – 1984 Wayne Wettlaufer (December 16, 1943 – June 21, 2015) Progressive Conservative, Kitchener Centre 1995 – 2003 Keith Brown (November 7, 1926 – July 7, 2015) Progressive Conserva- tive, Peterborough 1959 – 1967 Robert TS Frankford (August 1, 1939 – August 1, 2015) New Demo- crat, Scarborough East 1990-1995 Joan Fawcett (April 19, 1937 – August 16, 2015) Liberal, Northumber- land 1987-1995 Derwyn Shea (September 1, 1937 – August 15, 2015) Progressive Conservative High Park - Swansea 1995-1999 Hugh O’Neil (July 10, 1936 – September 14, 2015) Liberal, Quinte 1975-1995 John Ferris (January 29, 1933 - September 27, 2015) Liberal, London South 1975-1977 William Leo Jordan (December 29, 1929 – February 15, 2015) Progres- sive Conservative, Lanark – Renfrew 1990 - 1999 Year In Review 2015 page 2|InFormer Bill 65, passed on May 10, 2000 during the 37th Session, founded the Ontario Association of Former OAFP Parliamentarians. It was the first bill in Ontario history to be introduced by a Legislative Committee. -

The CANADA Philes
Appeal/Counter Application No C45333, M34053, M34044, 34079, M34080, M34070, M33872(A), M33872 (B) M34103 ETC. Ex-parte Motions (x2) Court file No.: 05-FA-013780 and 01-FA-10663, and C11178/04-A1, and file no. C42332 Sending start date: Sept. 2006 New No. M34561 Dec. 20, 006 THE COURT OF APPEAL FOR ONTARIO 130 Queen St. W. Toronto, Ontario M5H 2N5 PH: 416-327-5020 & FX: 416-327-5032 If this information is important to you, save it independently. UPDATED FEB RUARY 02 , 2007 OF The CANADA Philes copy right for the public of the world INTERNATIONAL PEDOPHILE TRACING I rely on freedom of expression of my experiences & views of those experiences in light of the risk to my daughter & lack of police protection to post this site. This sight explains an overview of my position & circumstances that are long awaiting relief. I am requesting public assistance in investigating the abduction of my daughter, 6 year old, Annie Ivy- Lee Aviado. She was abducted by a "cult" like group of pedo & or necrophiles that are imposters in positions of authority in Ontario. The children of the public belong to the public & we all have the legal & innate right to investigate & enforce the Charter section 7., we are a family of human beings. Please provide any factual information regarding these issues & forward to [email protected]. with names, dates, locations and leads on where to locate any possible supporting evidence. Be the police of pedophiles as our most important purpose & possessions beside the environment issues. The authorities appear to have formed a "cult" in "Criminal Breach of Trust" section 336. -

Mon 1 Nov 1999 / Lun 1Er Nov 1999
No. 7A No 7A ISSN 1180-2987 Legislative Assembly Assemblée législative of Ontario de l’Ontario First Session, 37th Parliament Première session, 37e législature Official Report Journal of Debates des débats (Hansard) (Hansard) Monday 1 November 1999 Lundi 1er novembre 1999 Speaker Président Honourable Gary Carr L’honorable Gary Carr Clerk Greffier Claude L. DesRosiers Claude L. DesRosiers Hansard on the Internet Le Journal des débats sur Internet Hansard and other documents of the Legislative Assembly L’adresse pour faire paraître sur votre ordinateur personnel can be on your personal computer within hours after each le Journal et d’autres documents de l’Assemblée législative sitting. The address is: en quelques heures seulement après la séance est : http://www.ontla.on.ca/ Index inquiries Renseignements sur l’index Reference to a cumulative index of previous issues may be Adressez vos questions portant sur des numéros précédents obtained by calling the Hansard Reporting Service indexing du Journal des débats au personnel de l’index, qui vous staff at 416-325-7410 or 325-3708. fourniront des références aux pages dans l’index cumulatif, en composant le 416-325-7410 ou le 325-3708. Copies of Hansard Exemplaires du Journal Information regarding purchase of copies of Hansard may Pour des exemplaires, veuillez prendre contact avec be obtained from Publications Ontario, Management Board Publications Ontario, Secrétariat du Conseil de gestion, Secretariat, 50 Grosvenor Street, Toronto, Ontario, M7A 50 rue Grosvenor, Toronto (Ontario) M7A 1N8. Par 1N8. Phone 416-326-5310, 326-5311 or toll-free téléphone : 416-326-5310, 326-5311, ou sans frais : 1-800-668-9938. -

Groups Finalize Building Leases
Thomas B. McPherson Colin A. Brown John T. Kalm Thomas McPherson & Associates LAW FIRM T: 905-727-3151 Aurora’s Community Newspaper F: 905-841-4395 Vol. 3 No. 44 Week of September 2, 2003 905-727-3300 Aurora bingo lease deal collapses in final hour The deal was set, as far as the It blew up last Wednesday when weren't interested in signing the book, that's exactly what it will be. opened Aurora's Bingo World Oct. tenant was concerned. the owners of the building at the lease. The sudden move puts Kereakou 1, is not finished yet. All it needed was a signature on corner of Engelhard and Edward It's expected the building will and 34 local charities, including "I need to find a place in Aurora the lease and Aurora's bingo hall told Perry Kereakou, who would become a storage area, and judg- 12 Aurora organizations, out in that can accommodate a bingo would continue after Sept. 30. own the new bingo business, they ing by a full page advertisement in the street. hall and has the parking to go Groups finalize the latest edition of the telephone But Kereakou, who would have Please see page 15 building leases It was a long time coming, but Jones that the two items, since two major Aurora organizations they were not called for discus- finalized leases with the Town at sion, had been approved. Tuesday's council meeting. Theatre Aurora has major reno- Theatre Aurora and the Aurora vation plans for the old cement Historical Society learned the factory, and the AHS plans to set leases had been approved giving up a Heritage Centre, which will them several years' use of include the museum, at the Factory Theatre and the Church Church Street School. -
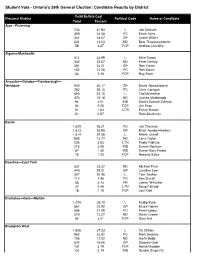
Candidate Results W Late Results
Student Vote - Ontario's 39th General Election: Candidate Results by District Valid Ballots Cast Electoral District Political Code Name of Candidate Total Percent Ajax—Pickering 743 41.93 L Joe Dickson 409 23.08 PC Kevin Ashe 331 18.67 GP Cecile Willert 231 13.03 ND Bala Thavarajasoorier 58 3.27 FCP Andrew Carvalho Algoma-Manitoulin 514 33.99 L Mike Brown 432 28.57 ND Peter Denley 351 23.21 GP Ron Yurick 152 10.05 PC Ron Swain 63 4.16 FCP Ray Scott Ancaster—Dundas—Flamborough— Westdale 940 30.17 GP David Januczkowski 782 25.10 PC Chris Corrigan 690 22.15 L Ted Mcmeekin 473 15.18 ND Juanita Maldonado 94 3.01 IND Martin Samuel Zuliniak 64 2.05 FCP Jim Enos 51 1.63 COR Eileen Butson 21 0.67 Sam Zaslavsky Barrie 1,629 26.21 PC Joe Tascona 1,613 25.95 GP Erich Jacoby-Hawkins 1,514 24.36 L Aileen Carroll 856 13.77 ND Larry Taylor 226 3.63 LTN Paolo Fabrizio 215 3.45 IND Darren Roskam 87 1.39 IND Daniel Gary Predie 75 1.20 FCP Roberto Sales Beaches—East York 531 35.37 ND Michael Prue 440 29.31 GP Caroline Law 307 20.45 L Tom Teahen 112 7.46 PC Don Duvall 56 3.73 FR James Whitaker 37 2.46 LTN Doug Patfield 18 1.19 FCP Joel Kidd Bramalea—Gore—Malton 1,079 38.70 L Kuldip Kular 667 23.92 GP Bruce Haines 588 21.09 PC Pam Hundal 370 13.27 ND Glenn Crowe 84 3.01 FCP Gary Nail Brampton West 1,526 37.23 L Vic Dhillon 962 23.47 PC Mark Beckles 706 17.22 ND Garth Bobb 642 15.66 GP Sanjeev Goel 131 3.19 FCP Norah Madden 131 3.19 IND Gurdial Singh Fiji Brampton—Springdale 1,057 33.95 ND Mani Singh 983 31.57 L Linda Jeffrey 497 15.96 PC Carman Mcclelland -

633058129179308750 Christop
By Christopher Twardawa [email protected] To be presented to the Ontario Citizens’ Assembly on Electoral Reform January 2007 Version ONE-070.131 www.ctess.ca www.TwardawaModel.org Any opinion or view presented in the document is that of and only of the author, Christopher Twardawa, and may not necessarily reflect those of any organization he is or has been associated with. Reproduction of this document in whole or in part is permitted, provided the source (Christopher Twardawa and www.ctess.ca or www.TwardawaModel.org ) is fully acknowledged. © Christopher Twardawa, 2007 TwardawaModel.org CTESS.ca Sometimes the simplest solution is the best. Christopher Twardawa Electoral System Solution ii TwardawaModel.org CTESS.ca About CTESS The Christopher Twardawa Electoral System Solution (CTESS) is the creation of its author – Christopher Twardawa and is designed to provide a better electoral system than what Canada and its provinces now have. With the belief that the current system is good but requires improvements, CTESS strengthens it by identifying deficiencies and proposing innovations. Unlike any other electoral system currently in use and which all have tradeoffs, CTESS has no tradeoffs and therefore eliminates the need to change electoral systems as a whole. Christopher first started thinking about this after the 1993 Canadian federal elections, since the results of those elections appeared to him to be inconsistent with how the voters voted. Ten years later in 2003, while still in university, he came up with the current model (the Twardawa Model) which is a simple yet considerate and sophisticated model. It can be applied to any democratic state under the Westminster model of government and similar systems. -

The Informer
Bill 65, passed on May 10, 2000 during the 37th Session, founded the Ontario Association of Former OAFP Parliamentarians. It was the first bill in Ontario history to be introduced by a Legislative Committee. Spring 2016 Bill 65, passed on May 10, 2000 during the 37th Session, founded the Ontario Association of Former OAFP Parliamentarians. It was the first bill in Ontario history to be introduced by a Legislative Committee. Table of Contents 1. Interview: Consul General of France...pg. 3 2. Order of Canada: Jim Gordon, Bob Rae...pg. 8 3. Remarkable Women Parliamentarians – Christine Elliott...pg. 9 4. Series: Meet the Premiers – Bob Rae...pg. 12 5. Notice – Annual General Meeting...pg. 15 6. Notice – Distinguished Service Award...pg. 17 7. Obituary – Charlie Tatham...pg. 18 8. Obituary – Joan Smith...pg. 20 9. Obituary - Ian Deans...pg. 22 10. Order of Ontario: Isabel Bassett, Mary Anne Chambers...pg. 24 11. Notice – Legislative Intern Programme Anniversary...pg. 25 12. Book review: “What’s Happened to Politics?” by Bob Rae...pg. 26 13. Interview: Gordon Carton...pg. 29 14. Frances Lankin appointed Canadian Senate...pg. 32 15. The Back Story – David Turnbull...pg. 33 16. Queen’s Park to Campus...pg. 35 17. Membership Renewal Form...pg. 36 18. Our new intern...pg. 37 19. Contact...pg. 38 Page 2 | InFormer Spring 2016 Bill 65, passed on May 10, 2000 during the 37th Session, founded the Ontario Association of Former OAFP Parliamentarians. It was the first bill in Ontario history to be introduced by a Legislative Committee. Interview: Marc Trouyet Consul General of France in Toronto There are more than 100 Consulates in Toronto, the second largest consular city in the world. -
June 7, 2006 Page 1 of 2
425 University Avenue, Suite 502 Toronto ON M5G 1T6 Tel: (416) 595-0006 Fax: (416) 595-0030 E-mail: [email protected] Providing leadership in public health management June 7, 2006 Mr. Wayne Arthurs, MPP, Pickering-Ajax-Uxbridge Hon. Sandra Pupatello, MPP, Windsor West Mr. Bas Balkissoon, MPP, Scarborough-Rouge River Mr. Shafiq Qaadri, MPP, Etobicoke North Hon. Rick Bartolucci, MPP, Sudbury Mr. Mario Racco, MPP, Thornhill Hon. Chris Bentley, MPP, London West Mr. Khalil Ramal, MPP, London-Fanshawe Mr. Lorenzo Berardinetti, MPP, Scarborough- Southwest Hon. David Ramsay, MPP, Timiskaming-Cochrane Hon. Marie Bountrogianni, MPP, Hamilton Mountain Mr. Lou Rinaldi, MPP, Northumberland Hon. Jim Bradley, MPP, St. Catharines Mr. Tony Ruprecht, MPP, Davenport Hon. Laurel Broten, MPP, Etobicoke-Lakeshore Ms. Liz Sandals, MPP, Guelph-Wellington Hon. Mike Brown, MPP, Algoma-Manitoulin Mr. Mario Sergio, MPP, York West Mr. Jim Brownell, MPP, Stormont-Dundas-Charlottenburg Ms. Monique Smith, MPP, Nipissing Hon. Michael Bryant, MPP, St. Paul’s Mr. Greg Sorbara, MPP, Vaughan-King-Aurora Hon. Donna Cansfield, MPP, Etobicoke Centre Hon. Harinder Takhar, MPP, Mississauga Centre Hon. David Caplan, MPP, Don Valley East Ms. Maria Van Bommel, MPP, Lambton-Kent-Middlesex Hon. Mary Anne Chambers, MPP, Scarborough East Hon. Jim Watson, MPP, Ottawa West-Nepean Hon. Mike Colle, MPP, Eglinton-Lawrence Mr. John Wilkinson, MPP, Perth-Middlesex Hon. Joe Cordiano, MPP, York South-Weston Mr. Tony Wong, MPP, Markham Mr. Kim Craitor, MPP, Niagara Falls Ms. Kathleen Wynne, MPP, Don Valley West Mr. Bruce Crozier,MPP, Essex Mr. David Zimmer, MPP, Willowdale Mr. Bob Delaney, MPP, Mississauga West Mr. Gilles Bisson, MPP, Timmins-James Bay Mr. -
Provincial Legislatures
PROVINCIAL LEGISLATURES ◆ PROVINCIAL & TERRITORIAL LEGISLATORS ◆ PROVINCIAL & TERRITORIAL MINISTRIES ◆ COMPLETE CONTACT NUMBERS & ADDRESSES Completely updated with latest cabinet changes! 80 / PROVINCIAL RIDINGS PROVINCIAL RIDINGS British Columbia Surrey-Cloverdale...................................Kevin Falcon.......................................90 Surrey-Green Timbers ............................Sue Hammell ......................................90 Total number of seats ................79 Surrey-Newton........................................Harry Bains.........................................88 Liberal..........................................46 Surrey-Panorama Ridge..........................Jagrup Brar..........................................88 New Democratic Party ...............33 Surrey-Tynehead.....................................Dave S. Hayer.....................................90 Surrey-Whalley.......................................Bruce Ralston......................................92 Abbotsford-Clayburn..............................John van Dongen ................................93 Surrey-White Rock .................................Gordon Hogg ......................................90 Abbotsford-Mount Lehman....................Michael de Jong..................................89 Vancouver-Burrard.................................Lorne Mayencourt ..............................91 Alberni-Qualicum...................................Scott Fraser .........................................90 Vancouver-Fairview ...............................Gregor