Print Version of OSICS9
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Fractures Fractura Pathologica
Fractures Fractura pathologica Myeloma Fractura traumatica Fractura aperta/clausa Fractura simplex/multiplex Fractura comminutiva Fractura transversa/obliqua Fractura spiralis/longitudinalis Fractura compressiva/impressiva Fractura incuneata Infractio = f. partialis = f. incompleta Fractura cum dislocatione ad axim ad latus ad longitudinem cum contractione ad longitudinem cum distractione AO ClassificationAuthentic reports of fractures : 2 S 4220 Fractura colli chirurgici humeri l. dx. comminutiva AO 11-C3 Fracture Healing: 1: REPOSITIO = REDUCTIO fragmentorum CLOSED (short /long term) Fracture Healing: 2: FIXATIO = STABILISATIO fragmentorum PLASTER CAST INTERNAL FIXATION Fracture Healing: 2: FIXATIO = STABILISATIO fragmentorum INTERNAL FIXATION Fracture Healing: 2: FIXATIO = STABILISATIO fragmentorum Name the type of fracture A B C D E F Choose a bone and break it. Try to write as much detailed diagnosis as possible. Authentic reports :1 collement = severe damage of soft tissues Authentic reports :2 Fr. aperta TSCHERNE I - open fracture with small skin injury without its contusion - negligible bacterial contamination Profesor Dr. Harald Tscherne (1933), Traumatology Clinic, Hannover: Classification of fractures published in 1982, T. divides fracture into open and closed. The most important for him is the degree of the soft tissues damage. Authentic reports :3 1 A 45-year-old woman presented with a 3-month history of generalized body pains nonresponsive to analgesic agents. Along with low back pain, she had progressive difficulty in getting up from sitting and supine positions and in walking. There was no history of trauma or any medication intake. She is an orthodox believer who wears a black veil outdoors and is completely covered, with little exposure to the sun. An anteroposterior radio- graph of the pelvis showed an undisplaced transverse fracture of the shaft of both femurs. -

Biomechanical Comparison of Fixation Stability Using a Lisfranc Plate
Foot and Ankle Surgery 25 (2019) 71–78 Contents lists available at ScienceDirect Foot and Ankle Surgery journa l homepage: www.elsevier.com/locate/fas Biomechanical comparison of fixation stability using a Lisfranc plate $ versus transarticular screws a,b a,c, d d Nathan C. Ho , Sophia N. Sangiorgio *, Spenser Cassinelli , Stephen Shymon , d a,b a,c d John Fleming , Virat Agrawal , Edward Ebramzadeh , Thomas G. Harris a The J. Vernon Luck, Sr., M.D. Orthopaedic Research Center, Orthopaedic Institute for Children, in Alliance with UCLA, 403 W. Adams Blvd., Los Angeles, CA 90007, United States b University of Southern California Department of Biomedical Engineering, Los Angeles, CA, United States c University of California, Los Angeles Department of Orthopaedic Surgery, Los Angeles, CA, United States d Los Angeles County Harbor—UCLA Medical Center, Los Angeles, CA, United States A R T I C L E I N F O A B S T R A C T Article history: Background: To obtain adequate fixation in treating Lisfranc soft tissue injuries, the joint is commonly Received 3 March 2017 stabilized using multiple transarticular screws; however iatrogenic injury is a concern. Alternatively, two Received in revised form 28 July 2017 parallel, longitudinally placed plates, can be used to stabilize the 1st and 2nd tarsometatarsal joints; Accepted 8 August 2017 however this may not provide adequate stability along the Lisfranc ligament. Several biomechanical studies have comparedearliermethodsoffixation using platestothestandardtransarticularscrew fixationmethod, Keywords: highlighting the potential issue of transverse stability using plates. A novel dorsal plate is introduced, Lisfranc injury intended to provide transverse and longitudinal stability, without injury to the articular cartilage. -
Shoulder Injuries: Dislocated Shoulder and Labral Tear
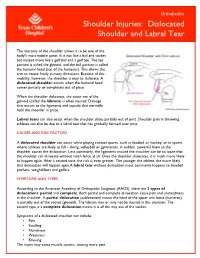
Orthopedics Shoulder Injuries: Dislocated Shoulder and Labral Tear The anatomy of the shoulder allows it to be one of the body's most mobile joints. It is not like a ball and socket but instead more like a golf ball and a golf tee. The tee portion is called the glenoid, and the ball portion is called the humeral head (top of the humerus). This allows the arm to rotate freely in many directions. Because of this mobility, however, the shoulder is easy to dislocate. A dislocated shoulder occurs when the humeral head comes partially or completely out of place. When the shoulder dislocates, the outer rim of the glenoid (called the labrum) is often injured. Damage also occurs to the ligaments and capsule that normally hold the shoulder in place. Labral tears can also occur when the shoulder slides partially out of joint. Shoulder pain in throwing athletes can also be due to a labral tear that has gradually formed over time. CAUSES AND RISK FACTORS A dislocated shoulder can occur while playing contact sports, such as football or hockey, or in sports where athletes are likely to fall – skiing, volleyball or gymnastics. A sudden, powerful blow to the shoulder causes the dislocation. Less commonly, the ligaments around the shoulder can be so loose that the shoulder can dislocate without much force at all. Once the shoulder dislocates, it is much more likely to happen again. After a second time, the risk is even greater. The younger the athlete, the more likely that dislocation will happen again.A labral tear without dislocation most commonly happens to baseball pitchers, weightlifters and golfers. -
Dislocated Shoulder -Orthoinfo - AAOS Page 1 of 2
Dislocated Shoulder -OrthoInfo - AAOS Page 1 of 2 Dislocated Shoulder The shoulder joint is the body's most mobile joint. It can turn in many directions. But, this advantage also makes the shoulder an easy joint to dislocate. A partial dislocation (subluxation) means the head of the upper arm bone (humerus) is partially out of the socket (glenoid). A complete dislocation means it is all the way out of the socket. Both partial and complete dislocation cause pain and unsteadiness in the shoulder. Shoulder instability Symptoms Symptoms to look for include: • Swelling • Numbness • Weakness • Bruising Sometimes dislocation may tear ligaments or tendons in the shoulder or damage nerves. The shoulder joint can dislocate forward, backward, or downward. A common type of shoulder dislocation is when the shoulder slips forward (anterior instability). This means the upper arm bone moved forward and down out of its joint. It may happen when the arm is put in a throwing position. Diagnosis The muscles may have spasms from the disruption, and this can make it hurt more. When the shoulder dislocates time and again, there is shoulder instability. The doctor will examine the shoulder and may order an X-ray. It is important that the doctor know how the dislocation happened and whether the shoulder had ever been dislocated before. Treatment http://orthoinfo.aaos.org/topic.cfm?topic=A00035 2/2/2015 Dislocated Shoulder -OrthoInfo - AAOS Page 2 of 2 The doctor will place the ball of the upper arm bone (humerus) back into the joint socket. This process is called closed reduction. Severe pain stops almost immediately once the shoulder joint is back in place. -

An Old Mismanaged Lisfranc Injury Treated by Gradual Deformity Correction Followed by the Second-Stage Internal fixation
Strat Traum Limb Recon (2017) 12:59–62 DOI 10.1007/s11751-016-0273-3 CASE REPORT An old mismanaged Lisfranc injury treated by gradual deformity correction followed by the second-stage internal fixation 1 1 1 1 Mehraj D. Tantray • Khurshid Kangoo • Asif Nazir • Muzamil Baba • 1 1 1 Raja Rameez • Syed Tabish • Syed Shahnawaz Received: 29 May 2016 / Accepted: 27 December 2016 / Published online: 5 January 2017 Ó The Author(s) 2017. This article is published with open access at Springerlink.com Abstract The Lisfranc fracture-dislocation of the foot is Keywords Lisfranc injury Á Ilizarov Á Late diagnosis uncommon and diagnosis is often missed. The Lisfranc joint involves the articulation between medial cuneiform and base of the second metatarsal and is considered a Introduction keystone to structural integrity to the midfoot. The articu- lation has a stabilization effect on longitudinal and trans- Injuries to the tarsometatarsal joints are not common and verse arches of the foot. A neglected or untreated injury to represent less than 0.2% of all orthopaedic injuries with the Lisfranc joint can lead to secondary arthritis and sig- a reported incidence of 1 per 55,000 individuals [1]. The nificant morbidity and disability. We present a case of a injury is commonly missed due to gross swelling mask- neglected Lisfranc fracture-dislocation in a 28-year-old ing the deformity and subtle findings on radiological female patient who presented 3 months after injury. A evaluation which requires careful attention. Re-examina- staged treatment of distraction with an Ilizarov ring fixator tion after the decrease in oedema for persistent pain and followed in the second stage by the removal of ring fixator aggravation of pain or instability on stress examination and internal fixation with K wires was performed. -

Sports Injuries
Sports Injuries Lacrosse Lacrosse is America’s oldest game. It can be dated back to the Native Americans, and was used astraining for war. It is both played by boys and girls,however, some rules are drastically different between genders. Nonetheless, the combination of contact, a stick, a hard ball, and quick changes of direction, puts lacrosse players at risk for injury. Protective Equipment There is a wide range of equipment that lacrosse players wear. For girls, goggles and mouth pieces are mandatory. Lightweight gloves and headgear is optional. For boys, helmets with full face guards, shoulder pads, padded gloves, and mouth pieces are used. It is most important for this equipment to fit properly. If equipment does not fit properly it can actually cause injury. There is no helmet which has been proven through research that confused with a “dislocated shoulder,” which is when prevents concussions. the shoulder comes out of socket. Dislocated shoulders What are the most common types are not common in lacrosse. of lacrosse injuries? Concussions Contusions Concussions are quite common in lacrosse. For more information, please refer to our concussion handout. Because of the nature of the sport, bruises or contusions are very common in lacrosse. Contusions How can lacrosse injuries be prevented? are best initially treated with ice, compression, and elevation of the affected area. • Stay active year round Knee Injuries • Incorporate strength training and stretching into your normal routine Lacrosse players commonly injure their knees. Sprains of the medial and lateral collateral ligaments • Wear properly fitted equipment (MCL/LCL) occur. More serious injuries of the anterior and posterior cruciate ligaments (ACL/PCL) and to the • Hydrate adequately before, during, and menisci (cartilage of the knee) can also happen. -

“Swollen Ankle” Due to the Presence Of
f Bone R o e al s n e r a u r c o h J Journal of Bone Research Bojinca et al., J Bone Res 2017, 5:2 ISSN: 2572-4916 DOI: 10.4172/2572-4916.1000177 Case Report Open Access “Swollen Ankle” Due to the Presence of Accessory Soleus Muscle - Case Report Violeta Claudia Bojinca¹*, Teodora Andreea Serban² and Mihai Bojinca² ¹Department of Internal Medicine and Rheumatology, Hospital “Sfanta Maria”, University of Medicine and Pharmacy “Carol Davila”, Romania ²Department of Internal Medicine and Rheumatology, Hospital “Dr. Ion Cantacuzino”, University of Medicine and Pharmacy “Carol Davila”, Romania *Corresponding author: Violeta Claudia Bojinca, Department of Internal Medicine and Rheumatology, Hospital “Sfanta Maria”, Ion Mihalache Blv. 37-39, University of Medicine and Pharmacy “Carol Davila”, Bucharest, Romania, Tel: +40723924823; Fax +40212224064; E-mail: [email protected] Received Date: June 26, 2017; Accepted Date: July 10, 2017; Published Date: July 17, 2017 Copyright: © 2017 Bojinca CV, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract Swollen ankle might be a problem of differential diagnosis in young patients performing physical exercises. A mass on the posteromedial region of the ankle might be attributed to the presence of Accessory Soleus Muscle (ASM), the most common supernumerary muscle in the lower leg. We present the case of a young male with swelling and moderate pain on the posteromedial part of the right ankle after prolonged physical exercise. -

Bilateral Accessory Soleus Muscle
Turk J Med Sci 30 (2000) 393-395 © T†BÜTAK Short Report Zeliha KURTOÚLU Haluk ULUUTKU Bilateral Accessory Soleus Muscle Department of Anatomy, Faculty of Medicine, Black Sea Technical University, Trabzon-TURKEY Received: June 15, 1999 A bilateral occurrence of the accessory soleus muscle aponeurosis of this muscle and divided into two branches. (ASM) was encountered during lower extremity While one branch entered the SM, the other branch ran dissection of 20 newborn cadavers. downward and entered the ASM. The arterial branch to In the right leg, the muscle arose from the distal part the ASM was derived from the posterior tibial artery, and of the anterior aponeurosis of the soleus muscle (SM). reached the muscle at the upper third. Then it ran obliquely in a medial and inferior direction. In addition to the ASM, the plantaris muscle was ASM fibers did not contribute to SM fibers, and formed normally present in each leg. an independent tendon above the medial malleolus (Fig The ASM is a rare variation in the human SM. Frohse 1A). The smaller part of the tendon of the ASM attached and Frankel identified this anomalous muscle as a special to the calcaneus just anteromedial to the calcaneal plantaris muscle, the origin of which has migrated to the tendon. While the greater part contributed to the flexor anterior surface of the SM or to the tibia (1). In the other retinaculum, a branch from the tibial nerve and a branch studies, however, the plantaris muscle coexisted with the from the posterior tibial artery entered the ASM at the ASM (2,3). -

Pediatric MSK Protocols
UT Southwestern Department of Radiology Ankle and Foot Protocols - Last Update 5-18-2015 Protocol Indications Notes Axial Coronal Sagittal Ankle / Midfoot - Routine Ankle Pain Axial = In Relation to Leg "Footprint" (Long Axis to Foot) T1 FSE PD SPAIR T1 FSE Injury, Internal Derangement Coronal = In Relation to Leg (Short Axis Foot) PD SPAIR STIR Talar OCD, Coalition Protocol Indications Notes Axial Coronal Sagittal Ankle / Midfoot - Arthritis Arthritis Axial = In Relation to Leg "Footprint" (Long Axis to Foot) PD SPAIR PD SPAIR T1 FSE Coronal = In Relation to Leg (Short Axis Foot) STIR T1 SPIR POST T1 SPIR POST Protocol Indications Notes Axial Coronal Sagittal Foot - Routine Pain, AVN Axial = In Relation to Leg "Footprint" (Long Axis to Foot) T1 FSE PD FSE T1 FSE Coronal = In Relation to Leg (Short Axis Foot) PD SPAIR PD SPAIR STIR Protocol Indications Notes Axial Coronal Sagittal Foot - Arthritis Arthritis Axial = In Relation to Leg "Footprint" (Long Axis to Foot) T1 FSE PD SPAIR STIR Coronal = In Relation to Leg (Short Axis Foot) PD SPAIR T1 SPIR POST 3D WATS T1 SPIR POST Protocol Indications Notes Axial Coronal Sagittal Great Toe / MTP Joints Turf Toe Smallest Coil Possible (Microcoil if Available) PD FSE T1 FSE PD FSE Sesamoiditis FoV = Mid Metatarsal Through Distal Phalanges PD SPAIR PD SPAIR PD SPAIR Slice thickness = 2-3 mm, 10% gap Axial = In relation to the great toe (short axis foot) Coronal = In relation to the great toe (long axis foot / footprint) Appropriate Coronal Plane for Both Ankle and Foot Imaging UT Southwestern Department -

Differential Diagnosis and Treatment of Iliotibial Band Pain Secondary to a Hypomobile Cuboid in a 24-Year-Old Female Tri-Athlete
INTERNATIONAL ACADEMY OF ORTHOPEDIC MEDICINE VOLUME 4, ISSUE 1 WINTER 2015/2016 Differential Diagnosis and Treatment of Iliotibial Band Pain Secondary to a Hypomobile Cuboid in a 24-Year-Old Female Tri-Athlete Femoroacetabular Impingement in the Adolescent Population: A Review Immediate Changes in Widespread Pressure Pain Sensitivity, Neck Pain, and Cervical Spine Range of Motion after Cervical or Thoracic Thrust Manipulation in Patients with Bilateral Chronic Mechanical Neck Pain: A Randomized Clinical Trial IAOM-US CONNECTION DIRECTORY is published by John Hoops PT, COMT The International Managing Editor Academy of Orthopedic Medicine-US (IAOM-US) Valerie Phelps PT, ScD, OCS, FAAOMPT PO Box 65179 Chief Editor / Education Director Tucson, AZ 85728 (p) 866.426.6101 Tanya Smith PT, ScD, FAAOMPT (f) 866.698.4832 Senior Editor (e) [email protected] (w) www.iaom-us.com John Woolf MS, PT, ATC, COMT Business Director CONTACT (p) 866.426.6101 Sharon Fitzgerald (f) 866.698.4832 Executive Assistant (e) [email protected] (w) www.iaom-us.com Andrea Cameron All trademarks are the property Administrative Assistant/ of their respective owners. Marketing Liaison The IAOM-US CONNECTION VOLUME 4 CONNECTION Differential Diagnosis and Dear Colleagues: Treatment of Iliotibial Band Pain Secondary to a Hypomobile Cuboid We hope you’ve had a happy and healthy 2015 2 in a 24-Year-Old Female Tri-Athlete and are ready to set your sights on 2016. Our 2016 course schedule is set, though we’re always adding new course locations and topics. If you haven’t had a chance to see what’s coming to your neck of the woods, here’s a link to the schedule. -

Pediatric Orthopedic Injuries… … from an ED State of Mind
Traumatic Orthopedics Peds RC Exam Review February 28, 2019 Dr. Naminder Sandhu, FRCPC Pediatric Emergency Medicine Objectives to cover today • Normal bone growth and function • Common radiographic abnormalities in MSK diseases • Part 1: Atraumatic – Congenital abnormalities – Joint and limb pain – Joint deformities – MSK infections – Bone tumors – Common gait disorders • Part 2: Traumatic – Common pediatric fractures and soft tissue injuries by site Overview of traumatic MSK pain Acute injuries • Fractures • Joint dislocations – Most common in ED: patella, digits, shoulder, elbow • Muscle strains – Eg. groin/adductors • Ligament sprains – Eg. Ankle, ACL/MCL, acromioclavicular joint separation Chronic/ overuse injuries • Stress fractures • Tendonitis • Bursitis • Fasciitis • Apophysitis Overuse injuries in the athlete WHY do they happen?? Extrinsic factors: • Errors in training • Inappropriate footwear Overuse injuries Intrinsic: • Poor conditioning – increased injuries early in season • Muscle imbalances – Weak muscle near strong (vastus medialus vs lateralus patellofemoral pain) – Excessive tightness: IT band, gastroc/soleus Sever disease • Anatomic misalignments – eg. pes planus, genu valgum or varum • Growth – strength and flexibility imbalances • Nutrition – eg. female athlete triad Misalignment – an intrinsic factor Apophysitis • *Apophysis = natural protruberance from a bone (2ndary ossification centres, often where tendons attach) • Examples – Sever disease (Calcaneal) – Osgood Schlatter disease (Tibial tubercle) – Sinding-Larsen-Johansson -

Desarrollo De La Podología En España
Desarrollo de la podología en España Virginia Novel Martí ADVERTIMENT. La consulta d’aquesta tesi queda condicionada a l’acceptació de les següents condicions d'ús: La difusió d’aquesta tesi per mitjà del servei TDX (www.tdx.cat) i a través del Dipòsit Digital de la UB (diposit.ub.edu) ha estat autoritzada pels titulars dels drets de propietat intelꞏlectual únicament per a usos privats emmarcats en activitats d’investigació i docència. No s’autoritza la seva reproducció amb finalitats de lucre ni la seva difusió i posada a disposició des d’un lloc aliè al servei TDX ni al Dipòsit Digital de la UB. No s’autoritza la presentació del seu contingut en una finestra o marc aliè a TDX o al Dipòsit Digital de la UB (framing). Aquesta reserva de drets afecta tant al resum de presentació de la tesi com als seus continguts. En la utilització o cita de parts de la tesi és obligat indicar el nom de la persona autora. ADVERTENCIA. La consulta de esta tesis queda condicionada a la aceptación de las siguientes condiciones de uso: La difusión de esta tesis por medio del servicio TDR (www.tdx.cat) y a través del Repositorio Digital de la UB (diposit.ub.edu) ha sido autorizada por los titulares de los derechos de propiedad intelectual únicamente para usos privados enmarcados en actividades de investigación y docencia. No se autoriza su reproducción con finalidades de lucro ni su difusión y puesta a disposición desde un sitio ajeno al servicio TDR o al Repositorio Digital de la UB.