Birth Injury Documentation in ICD-10-CM
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

N35.12 Postinfective Urethral Stricture, NEC, Female N35.811 Other
N35.12 Postinfective urethral stricture, NEC, female N35.811 Other urethral stricture, male, meatal N35.812 Other urethral bulbous stricture, male N35.813 Other membranous urethral stricture, male N35.814 Other anterior urethral stricture, male, anterior N35.816 Other urethral stricture, male, overlapping sites N35.819 Other urethral stricture, male, unspecified site N35.82 Other urethral stricture, female N35.911 Unspecified urethral stricture, male, meatal N35.912 Unspecified bulbous urethral stricture, male N35.913 Unspecified membranous urethral stricture, male N35.914 Unspecified anterior urethral stricture, male N35.916 Unspecified urethral stricture, male, overlapping sites N35.919 Unspecified urethral stricture, male, unspecified site N35.92 Unspecified urethral stricture, female N36.0 Urethral fistula N36.1 Urethral diverticulum N36.2 Urethral caruncle N36.41 Hypermobility of urethra N36.42 Intrinsic sphincter deficiency (ISD) N36.43 Combined hypermobility of urethra and intrns sphincter defic N36.44 Muscular disorders of urethra N36.5 Urethral false passage N36.8 Other specified disorders of urethra N36.9 Urethral disorder, unspecified N37 Urethral disorders in diseases classified elsewhere N39.0 Urinary tract infection, site not specified N39.3 Stress incontinence (female) (male) N39.41 Urge incontinence N39.42 Incontinence without sensory awareness N39.43 Post-void dribbling N39.44 Nocturnal enuresis N39.45 Continuous leakage N39.46 Mixed incontinence N39.490 Overflow incontinence N39.491 Coital incontinence N39.492 Postural -
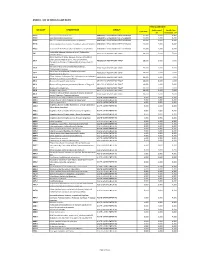
Annex 1: List of Medical Case Rates
ANNEX 1. LIST OF MEDICAL CASE RATES FIRST CASE RATE ICD CODE DESCRIPTION GROUP Professional Health Care Case Rate Fee Institution Fee P91.3 Neonatal cerebral irritability ABNORMAL SENSORIUM IN THE NEWBORN 12,000 3,600 8,400 P91.4 Neonatal cerebral depression ABNORMAL SENSORIUM IN THE NEWBORN 12,000 3,600 8,400 P91.6 Hypoxic ischemic encephalopathy of newborn ABNORMAL SENSORIUM IN THE NEWBORN 12,000 3,600 8,400 P91.8 Other specified disturbances of cerebral status of newborn ABNORMAL SENSORIUM IN THE NEWBORN 12,000 3,600 8,400 P91.9 Disturbance of cerebral status of newborn, unspecified ABNORMAL SENSORIUM IN THE NEWBORN 12,000 3,600 8,400 Peritonsillar abscess; Abscess of tonsil; Peritonsillar J36 ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 cellulitis; Quinsy Other diseases of larynx; Abscess of larynx; Cellulitis of larynx; Disease NOS of larynx; Necrosis of larynx; J38.7 ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 Pachyderma of larynx; Perichondritis of larynx; Ulcer of larynx Retropharyngeal and parapharyngeal abscess; J39.0 ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 Peripharyngeal abscess Other abscess of pharynx; Cellulitis of pharynx; J39.1 ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 Nasopharyngeal abscess Other diseases of pharynx; Cyst of pharynx or nasopharynx; J39.2 ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 Oedema of pharynx or nasopharynx J85.1 Abscess of lung with pneumonia ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 J85.2 Abscess of lung without pneumonia; Abscess of lung NOS ABSCESS OF RESPIRATORY -

Subset of Alphabetical Index to Diseases and Nature of Injury for Use with Perinatal Conditions (P00-P96)
Subset of alphabetical index to diseases and nature of injury for use with perinatal conditions (P00-P96) SUBSET OF ALPHABETICAL INDEX TO DISEASES AND NATURE OF INJURY FOR USE WITH PERINATAL CONDITIONS (P00-P96) Conditions arising in the perinatal period Conditions arising—continued - abnormal, abnormality—continued Note - Conditions arising in the perinatal - - fetus, fetal period, even though death or morbidity - - - causing disproportion occurs later, should, as far as possible, be - - - - affecting fetus or newborn P03.1 coded to chapter XVI, which takes - - forces of labor precedence over chapters containing codes - - - affecting fetus or newborn P03.6 for diseases by their anatomical site. - - labor NEC - - - affecting fetus or newborn P03.6 These exclude: - - membranes (fetal) Congenital malformations, deformations - - - affecting fetus or newborn P02.9 and chromosomal abnormalities - - - specified type NEC, affecting fetus or (Q00-Q99) newborn P02.8 Endocrine, nutritional and metabolic - - organs or tissues of maternal pelvis diseases (E00-E99) - - - in pregnancy or childbirth Injury, poisoning and certain other - - - - affecting fetus or newborn P03.8 consequences of external causes (S00-T99) - - - - causing obstructed labor Neoplasms (C00-D48) - - - - - affecting fetus or newborn P03.1 Tetanus neonatorum (A33) - - parturition - - - affecting fetus or newborn P03.9 - ablatio, ablation - - presentation (fetus) (see also Presentation, - - placentae (see also Abruptio placentae) fetal, abnormal) - - - affecting fetus or newborn -

Mortality Perinatal Subset, 2013
ICD-10 Mortality Perinatal Subset (2013) Subset of alphabetical index to diseases and nature of injury for use with perinatal conditions (P00-P96) Conditions arising in the perinatal period Note - Conditions arising in the perinatal period, even though death or morbidity occurs later, should, as far as possible, be coded to chapter XVI, which takes precedence over chapters containing codes for diseases by their anatomical site. These exclude: Congenital malformations, deformations and chromosomal abnormalities (Q00-Q99) Endocrine, nutritional and metabolic diseases (E00-E99) Injury, poisoning and certain other consequences of external causes (S00-T99) Neoplasms (C00-D48) Tetanus neonatorum (A33 2a) A -ablatio, ablation - - placentae (see alsoAbruptio placentae) - - - affecting fetus or newborn P02.1 2a -abnormal, abnormality, abnormalities - see also Anomaly - - alphafetoprotein - - - maternal, affecting fetus or newborn P00.8 - - amnion, amniotic fluid - - - affecting fetus or newborn P02.9 - - anticoagulation - - - newborn (transient) P61.6 - - cervix NEC, maternal (acquired) (congenital), in pregnancy or childbirth - - - causing obstructed labor - - - - affecting fetus or newborn P03.1 - - chorion - - - affecting fetus or newborn P02.9 - - coagulation - - - newborn, transient P61.6 - - fetus, fetal 1 ICD-10 Mortality Perinatal Subset (2013) - - - causing disproportion - - - - affecting fetus or newborn P03.1 - - forces of labor - - - affecting fetus or newborn P03.6 - - labor NEC - - - affecting fetus or newborn P03.6 - - membranes -

Ten Leading Causes of Death by Age Group,Race/Ethnicity, and Gender
Ten Leading Causes of Death by Age Group, Race/Ethnicity, and Gender Suburban Cook County 2006-2008 Suggested Citation: Cook County Department of Public Health. (2013). Ten Leading Causes of Death Tables 2008. Oak Forest, IL: Community Epidemiology and Health Planning Unit Table of Contents All Suburban Cook County: All Deaths By Gender: Females Males By Race/Ethnicity and Gender: Hispanic Hispanic Females Hispanic Males Non Hispanic Asian/Pacific Islander Non Hispanic Asian/Pacific Islander Females Non Hispanic Asian/Pacific Islander Males Non Hispanic Black Non Hispanic Black Females Non Hispanic Black Males Non Hispanic White Non Hispanic White Females Non Hispanic White Males By District: Cook County Department of Public Health Jurisdiction North District West District Southwest District South District Resources: District Map Rankable Causes of Death Rankable Causes of Infant Death 10 Leading Causes of Death by Age Group, Suburban Cook County, 2006-2008 (Counts/Percent of Total Deaths) All Deaths Rank <1 1-4 5-17 18-24 25-34 35-44 45-54 55-64 65+ Total Unintentional Unintentional Unintentional Unintentional Malignant Malignant Malignant Short Gestation Heart Disease Heart Disease 1 Injury Injury Injury Injury Neoplasms Neoplasms Neoplasms 170 24.9% 24 23.8% 57 24.6% 196 37.0% 281 34.4% 300 19.2% 1,251 31.7% 2,489 38.9% 13,422 28.2% 16,345 26.4% Congenital Congenital Unintentional Malignant Malignant Homicide Homicide Homicide Heart Disease Heart Disease 2 Anomalies Anomalies Injury Neoplasms Neoplasms 127 18.6% 9 8.9% 44 19.0% 135 -
Instructions / સૂચના Candidate Must Ensure Compliance to the Instructions Mentioned Below, Else Objections Shall Not Be Considered:
ANK PROVISIONAL ANSWER KEY [CBRT] Name of The Post Associate Professor, Obstetrics and Gynaecology, General State Service, (Special Recruitment) ,Class-1 | Advertisement No 57/2019-20 Preliminary Test Held On 24-02-2021 Que. No. 001-200 Publish Date 25-02-2021 Last Date to Send Suggestion (S) 05-03 -2021 Instructions / સૂચના Candidate must ensure compliance to the instructions mentioned below, else objections shall not be considered: - (1) All the suggestion should be submitted in prescribed format of suggestion sheet Physically. (2) Question wise suggestion to be submitted in the prescribed formatr (Suggestion rSheet) published on the website.r r (3) All suggestions are to be submitted with reference to the Maste Question Pape withr provisional answe key (Maste Question Paper), published herewith on the website. Objections should be sent referring to the Question, rQuestion No. & options ofr the Maste Question Paper. (4) Suggestions regarding question nos. and options othe than provisional answe key (Master Question Paper) shall not be considered. r (5) Objections and answers suggestedr by the candidate should be in compliance with the responses givenr by him in his answe sheet. Objections shall not be considered, r in case, if responses given in the answe sheet /response sheet and submitted suggestions are differed. (6) Objection fo each question shall be made on separate sheet. Objection fo more than one question in single sheet shall not be considered & treated as cancelled. ઉમેદવાર ે નીચેની સૂચનાઓનું પાલન કરવાની તકેદારી રાખવી, અયથા વાંધા-સૂચન અંગે કર ેલ રજૂઆતો યાને લેવાશે નહીં (1) ઉમેદવારે વાંધા-સૂચનો િનયત કરવામાં આવેલ વાંધા-સૂચન પકથી રજૂ કરવાના રહેશે. -

Helping Mothers Defend Their Decision to Breastfeed
University of Central Florida STARS Electronic Theses and Dissertations, 2004-2019 2015 Helping Mothers Defend their Decision to Breastfeed Kandis Natoli University of Central Florida Part of the Nursing Commons Find similar works at: https://stars.library.ucf.edu/etd University of Central Florida Libraries http://library.ucf.edu This Doctoral Dissertation (Open Access) is brought to you for free and open access by STARS. It has been accepted for inclusion in Electronic Theses and Dissertations, 2004-2019 by an authorized administrator of STARS. For more information, please contact [email protected]. STARS Citation Natoli, Kandis, "Helping Mothers Defend their Decision to Breastfeed" (2015). Electronic Theses and Dissertations, 2004-2019. 1392. https://stars.library.ucf.edu/etd/1392 HELPING MOTHERS DEFEND THEIR DECISION TO BREASTFEED by KANDIS M. NATOLI M.S.N. University of Central Florida, 2006 B.S.N. University of Central Florida, 2005 A dissertation submitted in partial fulfillment of the requirements for the Degree of Doctor of Philosophy in Nursing in the College of Nursing at the University of Central Florida Orlando Florida Fall Term 2015 Major Professor: Karen Arioan © 2015 Kandis M. Natoli ii ABSTRACT The United States has established breastfeeding as an important health indicator within the Healthy People agenda. Healthy People target goals for breastfeeding initiation, duration, and exclusivity remain unmet. The US Surgeon General’s Office reports that lack of knowledge and widespread misinformation about breastfeeding are barriers to meeting Healthy People goals. Breastfeeding mothers are vulnerable to messages that cast doubt on their ability to breastfeed. Very little research has examined specific approaches to help people resist negative messages about health beliefs and behaviors. -

Parturitional Brain Injury Definition of Parturitional Injury
Parturitional Brain Injury Definition of parturitional injury Thierry A.G.M. Huisman, MD • Any condition that affects the fetus adversely Director Pediatric Radiology and Pediatric Neuroradiology Johns Hopkins Hospital during labor and delivery • May be caused by: – Hypoxia and infection (birth injury) – Mechanical forces (birth trauma) Definition of parturitional injury Introduction • Life starts with a mechanical trauma – Squeezed together by a muscular wrapping • Any condition that affects the fetus adversely – Pushed through a narrow, bony canal with multiple bumps during labor and delivery – Getting your neck extended, rotated and pulled – Life line (umbilical cord) may be compressed – Possibly additional “medieval” instrumentation • May be caused by: – All of this for many minutes or even hours – Hypoxia and infection (birth injury) – Mechanical forces (birth trauma) Introduction Introduction • Life starts with a mechanical trauma • Life starts with a “stress” trauma – Or even worse, within minutes you are squeezed – And than suddenly lots of light, noise and many and “ejected” crying/emotional people around you,…. 1 Subjects who try to relive the „Scientific approach” “I am stuck feeling” Tortuguero expedition. www.philsheldon.wordpress.com Guettler FV, et al. Magnetic resonance imaging of the active second stage of labour: Proof of principle Eur Radiol 2012;22:2020-2026 Epidemiology Epidemiology • Significant variability across the world • Dramatically decreased in last decades • Birth trauma in 3% of all live births • Accounts for less than 2% of neonatal deaths • Even when the injuries are benign, birth trauma may result in significant anxiety for a family Disability adjusted life year (DALY): Measure of overall disease burden expressed as number of years lost due to ill-health, disability or early death Reichard R. -

Alphabetical Index to Diseases and Nature of Injury for Use with Perinatal Conditions (P00-P96)
Subset of alphabetical index to diseases and nature of injury for use with perinatal conditions (P00-P96) SUBSET OF ALPHABETICAL INDEX TO DISEASES AND NATURE OF INJURY FOR USE WITH PERINATAL CONDITIONS (P00-P96) Conditions arising in the perinatal period Conditions arising—continued - abnormal, abnormality—continued Note - Conditions arising in the perinatal - - fetus, fetal period, even though death or morbidity occurs - - - causing disproportion later, should, as far as possible, be coded to - - - - affecting fetus or newborn P03.1 chapter XVI, which takes precedence over - - forces of labor chapters containing codes for diseases by - - - affecting fetus or newborn P03.6 their anatomical site. - - labor NEC - - - affecting fetus or newborn P03.6 These exclude: - - membranes (fetal) Congenital malformations, deformations - - - affecting fetus or newborn P02.9 and chromosomal abnormalities - - - specified type NEC, affecting fetus or (Q00-Q99) newborn P02.8 Endocrine, nutritional and metabolic - - organs or tissues of maternal pelvis diseases (E00-E99) - - - in pregnancy or childbirth Injury, poisoning and certain other - - - - affecting fetus or newborn P03.8 consequences of external causes (S00-T99) - - - - causing obstructed labor Neoplasms (C00-D48) - - - - - affecting fetus or newborn P03.1 Tetanus neonatorum (A33) - - parturition - - - affecting fetus or newborn P03.9 - ablatio, ablation - - presentation (fetus) (see also Presentation, - - placentae (see also Abruptio placentae) fetal, abnormal) - - - affecting fetus or newborn P02.1 -

Operative Vaginal Delivery
FOURTH EDITION OF THE ALARM INTERNATIONAL PROGRAM CHAPTER 18 OPERATIVE VAGINAL DELIVERY Learning Objectives By the end of this chapter, the participant will: 1. Compare and contrast the methods available for operative vaginal delivery including the benefits, risks and indications for each method. 2. Describe the mnemonic for the safe use of vacuum and forceps for operative vaginal delivery. 3. Describe the appropriate documentation that should be recorded after every operative vaginal delivery. Introduction Operative vaginal delivery refers to the use of a vacuum or forceps in vaginal deliveries. Both methods are safe and reliable for assisting childbirth, if appropriate attention is paid to the indications and contraindications for the procedures. The benefits and risks to both the woman and her fetus of using either instrument or the risks associated with proceeding to the alternative of cesarean section delivery must be considered in every case. The choice of instrument should suit both the clinical circumstances, the skill of the health care provider and the acceptance of the woman. The health care provider should have training, experience and judgmental ability with the instrument chosen. Informed consent is an essential step in preparing for an operative vaginal delivery. Operative vaginal delivery should be avoided in women who are HIV positive to reduce mother-to-child transmission. If forceps or vacuum is necessary, avoid performing an episiotomy. Assessing the Descent of the Baby Prior to performing an operative delivery, it is essential to determine that the vertex is fully engaged. Descent of the baby may be assessed abdominally or vaginally. When there is a significant degree of caput (swelling) or molding (overlapping of the fetal skull bones), assessment by abdominal palpation using ―fifths of head palpable‖ is more useful than assessment by vaginal examination. -

XI. COMPLICATIONS of PREGNANCY, Childbffith and the PUERPERIUM 630 Hydatidiform Mole Trophoblastic Disease NOS Vesicular Mole Ex
XI. COMPLICATIONS OF PREGNANCY, CHILDBffiTH AND THE PUERPERIUM PREGNANCY WITH ABORTIVE OUTCOME (630-639) 630 Hydatidiform mole Trophoblastic disease NOS Vesicular mole Excludes: chorionepithelioma (181) 631 Other abnormal product of conception Blighted ovum Mole: NOS carneous fleshy Excludes: with mention of conditions in 630 (630) 632 Missed abortion Early fetal death with retention of dead fetus Retained products of conception, not following spontaneous or induced abortion or delivery Excludes: failed induced abortion (638) missed delivery (656.4) with abnormal product of conception (630, 631) 633 Ectopic pregnancy Includes: ruptured ectopic pregnancy 633.0 Abdominal pregnancy 633.1 Tubalpregnancy Fallopian pregnancy Rupture of (fallopian) tube due to pregnancy Tubal abortion 633.2 Ovarian pregnancy 633.8 Other ectopic pregnancy Pregnancy: Pregnancy: cervical intraligamentous combined mesometric cornual mural - 355- 356 TABULAR LIST 633.9 Unspecified The following fourth-digit subdivisions are for use with categories 634-638: .0 Complicated by genital tract and pelvic infection [any condition listed in 639.0] .1 Complicated by delayed or excessive haemorrhage [any condition listed in 639.1] .2 Complicated by damage to pelvic organs and tissues [any condi- tion listed in 639.2] .3 Complicated by renal failure [any condition listed in 639.3] .4 Complicated by metabolic disorder [any condition listed in 639.4] .5 Complicated by shock [any condition listed in 639.5] .6 Complicated by embolism [any condition listed in 639.6] .7 With other -

ICD-10-Mortality Perinatal Subset - 2017
ICD-10-Mortality Perinatal Subset - 2017 Subset of alphabetical index to diseases and nature of injury for use with perinatal conditions (P00-P96) Conditions arising in the perinatal period Note - Conditions arising in the perinatal period, even though death or morbidity occurs later, should, as far as possible, be coded to chapter XVI, which takes precedence over chapters containing codes for diseases by their anatomical site. These exclude: Congenital malformations, deformations and chromosomal abnormalities (Q00-Q99) Endocrine, nutritional and metabolic diseases (E00-E99) Injury, poisoning and certain other consequences of external causes (S00-T99) Neoplasms (C00-D48) Tetanus neonatorum (A33 2a ) A - ablatio, ablation - - placentae (see also Abruptio placentae) - - - affecting fetus or newborn P02.1 2a - abnormal, abnormality, abnormalities - see also Anomaly - - alphafetoprotein - - - maternal, affecting fetus or newborn P00.8 - - amnion, amniotic fluid - - - affecting fetus or newborn P02.9 - - anticoagulation - - - newborn (transient) P61.6 - - cervix NEC, maternal (acquired) (congenital), in pregnancy or childbirth - - - causing obstructed labor - - - - affecting fetus or newborn P03.1 - - chorion - - - affecting fetus or newborn P02.9 - - coagulation - - - newborn, transient P61.6 - - fetus, fetal - - - causing disproportion - - - - affecting fetus or newborn P03.1 - - forces of labor - - - affecting fetus or newborn P03.6 - - labor NEC - - - affecting fetus or newborn P03.6 - - membranes (fetal) - - - affecting fetus or newborn