Morphometric Study on Occurrence of Accessory Foramina in Middle Cranial Fossa S
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

MR Imaging of the Orbital Apex
J Korean Radiol Soc 2000;4 :26 9-0 6 1 6 MR Imaging of the Orbital Apex: An a to m y and Pat h o l o g y 1 Ho Kyu Lee, M.D., Chang Jin Kim, M.D.2, Hyosook Ahn, M.D.3, Ji Hoon Shin, M.D., Choong Gon Choi, M.D., Dae Chul Suh, M.D. The apex of the orbit is basically formed by the optic canal, the superior orbital fis- su r e , and their contents. Space-occupying lesions in this area can result in clinical d- eficits caused by compression of the optic nerve or extraocular muscles. Even vas c u l a r changes in the cavernous sinus can produce a direct mass effect and affect the orbit ap e x. When pathologic changes in this region is suspected, contrast-enhanced MR imaging with fat saturation is very useful. According to the anatomic regions from which the lesions arise, they can be classi- fied as belonging to one of five groups; lesions of the optic nerve-sheath complex, of the conal and intraconal spaces, of the extraconal space and bony orbit, of the cav- ernous sinus or diffuse. The characteristic MR findings of various orbital lesions will be described in this paper. Index words : Orbit, diseases Orbit, MR The apex of the orbit is a complex region which con- tains many nerves, vessels, soft tissues, and bony struc- Anatomy of the orbital apex tures such as the superior orbital fissure and the optic canal (1-3), and is likely to be involved in various dis- The orbital apex region consists of the optic nerve- eases (3). -

CT of Perineural Tumor Extension: Pterygopalatine Fossa
731 CT of Perineural Tumor Extension: Pterygopalatine Fossa Hugh D. Curtin1.2 Tumors of the oral cavity and paranasal sinuses can spread along nerves to areas Richard Williams 1 apparently removed from the primary tumor. In tumors of the palate, sinuses, and face, Jonas Johnson3 this "perineural" spread usually involves the maxillary division of the trigeminal nerve. The pterygopalatine fossa is a pathway of the maxillary nerve and becomes a key landmark in the detection of neural metastasis by computed tomogaphy (CT). Oblitera tion of the fat in the fossa suggests pathology. Case material illustrating neural extension is presented and the CT findings are described. Perineural extension is possibly the most insidious form of tumor spread of head and neck malignancy. After invading a nerve, tumor follows the sheath to reach the deeper connections of the nerve, escaping the area of a planned resection. Thus, detection of this form of extension is important in treatment planning and estimation of prognosis. The pterygopalatine fossa (PPF) is a key crossroad in extension along cranial nerve V. The second branch of the trigeminal nerve passes from the gasserian ganglion through the foramen rotundum into the PPF. Here the nerve branches send communications to the palate, sinus, nasal cavity, and face. Tumor can follow any of these routes proximally into the PPF and eventually to the gasserian ganglion in the middle cranial fossa. The PPF contains enough fat to be an ideal subject for computed tomographic (CT) evaluation. Obliteration of this fat is an important indicator of pathology, including perineural tumor spread. Other signs of perineural extension include enlargement of foramina, increased enhancement in the region of Meckel cave (gasserian ganglion), and atrophy of the muscles innervated by the trigeminal nerve. -

MBB: Head & Neck Anatomy
MBB: Head & Neck Anatomy Skull Osteology • This is a comprehensive guide of all the skull features you must know by the practical exam. • Many of these structures will be presented multiple times during upcoming labs. • This PowerPoint Handout is the resource you will use during lab when you have access to skulls. Mind, Brain & Behavior 2021 Osteology of the Skull Slide Title Slide Number Slide Title Slide Number Ethmoid Slide 3 Paranasal Sinuses Slide 19 Vomer, Nasal Bone, and Inferior Turbinate (Concha) Slide4 Paranasal Sinus Imaging Slide 20 Lacrimal and Palatine Bones Slide 5 Paranasal Sinus Imaging (Sagittal Section) Slide 21 Zygomatic Bone Slide 6 Skull Sutures Slide 22 Frontal Bone Slide 7 Foramen RevieW Slide 23 Mandible Slide 8 Skull Subdivisions Slide 24 Maxilla Slide 9 Sphenoid Bone Slide 10 Skull Subdivisions: Viscerocranium Slide 25 Temporal Bone Slide 11 Skull Subdivisions: Neurocranium Slide 26 Temporal Bone (Continued) Slide 12 Cranial Base: Cranial Fossae Slide 27 Temporal Bone (Middle Ear Cavity and Facial Canal) Slide 13 Skull Development: Intramembranous vs Endochondral Slide 28 Occipital Bone Slide 14 Ossification Structures/Spaces Formed by More Than One Bone Slide 15 Intramembranous Ossification: Fontanelles Slide 29 Structures/Apertures Formed by More Than One Bone Slide 16 Intramembranous Ossification: Craniosynostosis Slide 30 Nasal Septum Slide 17 Endochondral Ossification Slide 31 Infratemporal Fossa & Pterygopalatine Fossa Slide 18 Achondroplasia and Skull Growth Slide 32 Ethmoid • Cribriform plate/foramina -

Metoptic Canal and Warwick's Foramen: Incidence And
Eurasian J Med 2019; 51(1): 1-4 Original Article Metoptic Canal and Warwick’s Foramen: Incidence and Morphometric Analysis by Several Reference Points in the Human Orbit Arzu Hizay , Muzaffer Sindel ABSTRACT Objective: Several canals and foramens in the human orbit are well known in the literature. However, little is known about some minor canals or structures including metoptic canal and Warwick’s foramen. The aim of the present study was to make morphometric measurements and to determine the incidence of the metoptic canal and Warwick’s foramen in the Turkish population. Materials and Methods: Ninety-two dried human skulls were examined. All skulls were obtained from the Turkish population and collection of the Anatomy Department of the Akdeniz University. The metoptic canal and Warwick’s foramen were identified in the skulls. Incidence of these structures and diameters were determined. Morphometric measurements were made using various reference points in the orbit. Results: Of the 92 dry human skulls, the metoptic canal was detected in 20 of them. This canal was detected unilaterally. The metoptic canal was observed in 11 (11.9%) dry skulls in the right side, whereas it was ob- served in 9 (9.7%) dry skulls in the left side. There were no statistically significant differences according to the side for any of the measurements recorded (p>0.05). The Warwick’s foramen was observed in 12 (13.0%) skulls of all dry skulls. This foramen was also present unilaterally and was right sided in 7 (7.6%) skulls and left sided in 5 (5.4%) skulls. -
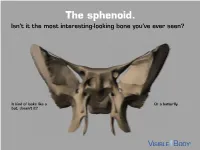
The Sphenoid. Isn’T It the Most Interesting-Looking Bone You’Ve Ever Seen?
The sphenoid. Isn’t it the most interesting-looking bone you’ve ever seen? It kind of looks like a Or a butterfly. bat, doesn’t it? The sphenoid articulates with 12 bones, both in the neurocranium and facial skeleton. The sphenoid is not just present in human skeletons, but also in mammalian ones. : A human has 1 Factoid sphenoid bone, but a dog has 8 bones that make up its sphenoid. The sphenoid is one of the 8 bones of the neurocranium (bones that protect the brain). It is the keystone* bone at the base of the skull. *In architecture, a keystone is the piece at the apex of an arch, locking all the other pieces together and bearing the weight of it all. The body of the sphenoid is the central part of the bone. It is a hollowed-out, cubical portion of the bone that forms the sphenoidal sinuses. The body is home to a deep depression known as the Sella turcica, which houses the pituitary gland. Factoid: sella turcica is Latin for “Turkish saddle” because of its resemblance to the saddles used by Turks, which had supports in the front and back. The greater wings of the sphenoid articulate with several bones, including the frontal, temporal, parietal, and zygomatic. They also serve as the attachment site for the temporalis muscles. The lesser wings are thin, triangular plates located above the greater wings. They, along with the body, form the optic canal. The optic nerve (II) passes through the optic canal to the eyes. The lateral and medial pterygoid plates project downward from the sphenoid body to give shape to the nasal cavity. -

Key Anatomical Landmarks for Middle Fossa Surgery: a Surgical Anatomy Study
LABORATORY INVESTIGATION J Neurosurg 131:1561–1570, 2019 Key anatomical landmarks for middle fossa surgery: a surgical anatomy study Maria Peris-Celda, MD, PhD,1 Avital Perry, MD,1 Lucas P. Carlstrom, MD, PhD,1 Christopher S. Graffeo, MD,1 Colin L. W. Driscoll, MD,1,2 and Michael J. Link, MD1,2 Departments of 1Neurologic Surgery and 2Otolaryngology–Head and Neck Surgery, Mayo Clinic, Rochester, Minnesota OBJECTIVE Middle fossa surgery is challenging, and reliable surgical landmarks are essential to perform accurate and safe surgery. Although many descriptions of the middle fossa components have been published, a clinically practical description of this very complex anatomical region is lacking. Small structure arrangements in this area are often not well visualized or accurately demarcated with neuronavigation systems. The objective is to describe a “roadmap” of key surgi- cal reference points and landmarks during middle fossa surgery to help the surgeon predict where critical structures will be located. METHODS The authors studied 40 dry skulls (80 sides) obtained from the anatomical board at their institution. Mea- surements of anatomical structures in the middle fossa were made with a digital caliper and a protractor, taking as refer- ence the middle point of the external auditory canal (MEAC). The results were statistically analyzed. RESULTS The petrous part of the temporal bone was found at a mean of 16 mm anterior and 24 mm posterior to the MEAC. In 87% and 99% of the sides, the foramen ovale and foramen spinosum, respectively, were encountered deep to the zygomatic root. The posterior aspect of the greater superficial petrosal nerve (GSPN) groove was a mean of 6 mm anterior and 25 mm medial to the MEAC, nearly parallel to the petrous ridge. -
Gross Anatomy Assignment
Gross Anatomy Assignment 17/mhs01/227 Odewenwa Oluwatobiloba Samuel Question 1: Write an essay on the cavernous sinus. The cavernous sinus within the human head is one of the dural venous sinuses creating a cavity called the lateral sellar compartment bordered by the temporal bone of the skull and the sphenoid bone, lateral to the sella turcica. It takes its source from the middle cerebral vein, sphenoparietal sinus, superior and inferior ophthalmic veins. It drains to the inferior and superior petrosal sinuses. The cavernous sinus is one of the dural venous sinuses of the head. It is a network of veins that sit in a cavity, approximately 1 x 2 cm in size in an adult.[2] The carotid siphon of the internal carotid artery, and cranial nerves III, IV, V (branches V1 and V2) and VI all pass through this blood filled space. Nearby structures to the cavernous sinus Superiorly: optic tract, optic chiasma, internal carotid artery. Inferiorly: Foramen lacerum and the junction of the body and greater wing of sphenoid bone. Medially: Hypophysis cerebri or (pituitary gland) and sphenoidal air sinus. Laterally: temporal lobe with uncus. Anteriorly: superior orbital fissure and the apex of the orbit. Posteriorly: apex of petrous temporal bone Contents of the cavernous sinus Apart from the blood which passes through a venous sinus, several anatomical structures, including some cranial nerves and their branches, also pass through the sinus. Structures within the outer (lateral) wall of the compartment from superior to inferior: Oculomotor nerve, Trochlear nerve, Ophthalmic and maxillary branches of the trigeminal nerve, Structures passing through the midline (medial) wall: Abducens nerve, Internal carotid artery accompanied by the Internal carotid plexus. -

An Osteologic Study of Human Ethmoidal Foramina with Special Reference to Their Classification and Symmetry
IJAE Vol. 121, n. 1: 66-76, 2016 ITALIAN JOURNAL OF ANATOMY AND EMBRYOLOGY Research article – Basic and applied anatomy An osteologic study of human ethmoidal foramina with special reference to their classification and symmetry Marì Regoli1, Eren Ogut2, Eugenio Bertelli1,* 1Department of Life Sciences, University of Siena, Siena, Italy, and 2Department of Anatomy, University of Akdeniz, Antalya, Turkey Abstract The present investigation was designed to study the anatomy of the ethmoidal foramina in adult human dry skulls. In addition to investigate the number of ethmoidal foramina that can be found on the orbital wall, we also addressed their classification and symmetry. The analy- sis of 1089 orbits demonstrated that the average number of ethmoidal foramina/orbit was 2.07 (range 0 to 4). As for their classification, we devised the relative depth index (RDI) to differenti- ate the anterior from the posterior ethmoidal foramina. The index represents the ratio “distance of the foramen from the anterior lacrimal crest/length of the medial orbital wall”. The average index of the anterior and posterior ethmoidal foramina were 0.53±0.04 and 0.84±0.06 respective- ly. As the mean of the two indexes was 0.685, we used the latter value as a sort of numerical watershed to define the domains of the anterior and of the posterior ethmoidal foramina on the orbital wall. Thus all ethmoidal foramina with an RDI ≤ 0.68 were considered anterior ethmoi- dal foramina and all ethmoidal foramina with an RDI ≥ 0.69 were considered posterior ethmoi- dal foramina. In this way it is possible to properly classify foramina on orbits with 1, 3 or 4 ethmoidal foramina. -

Anatomic Variations in Foramen Ovale and Foramen Spinosum
JK SCIENCE ORIGINAL ARTICLE Anatomic Variations In Foramen Ovale and Foramen Spinosum Berjina Farooq, Sangeeta Gupta, Sunanda Raina Abstract An anatomical study was conducted to observe the shapes of foramen ovale and foramen spinosum with their anatomical variants. The foramen ovale being one of the important foramina in the middle cranial fossa, is present in the superior surface of greater wing of sphenoid bone. Foramen spinosum is located posterolateral to foramen ovale. We studied seventeen human skulls and three sphenoid bones (i.e. total 40 foramen ovale and 40 foramen spinosum were studied, since foramen of right as well as left sides were taken for study). They were obtained from the Post graduate Department of Anatomy, Government Medical College, Jammu. Posterior part of the greater wing of sphenoid was observed for visualising the foramen ovale and foramen spinosum. Oval, round, almond and slit like foramen ovale were found. The maximum number was that of oval shaped foramina followed by almond, round and slit like foramen . Moreover, bony outgrowths in the form of spines were observed in two foramen ovale, and in the form of bony plate was seen in one foramen ovale. Furthermore, confluent foramen ovale and spinosum was seen on left side in one skull and on right side in another skull. Double foramen spinosum was seen in one skull on right side. Absence of foramen spinosum was observed in one of the skulls on right side. Foramen ovale is of surgical importance in percutaneous trigeminal rhizotomy in trigeminal neuralgias. For surgical procedures in the middle cranial fossa, the knowledge about the variations of these foramina should be taken into account. -

Imaging of Skull Base
MINI-SYMPOSIA-HEAD AND NECK Imaging of skull base: Pictorial essay Abhijit A Raut, Prashant S Naphade1, Ashish Chawla2 Department of Radiology, Seven Hills Hospital, Mumbai, 1Department of Radiology, Employee’s State Insurance Corporation Hospital, Mumbai, Maharashtra, 2Department of Radiology, Sri Aurobindo Medical College and Postgraduate Institute, Indore, Madhya Pradesh, India Correspondence: Dr. Abhijit Raut, Department of Radiology, Seven Hills Hospital, Marol Maroshi Road, Andheri East, Mumbai ‑ 400 059, India. E‑mail: [email protected] Abstract The skull base anatomy is complex. Numerous vital neurovascular structures pass through multiple channels and foramina located in the base skull. With the advent of computerized tomography (CT) and magnetic resonance imaging (MRI), accurate preoperative lesion localization and evaluation of its relationship with adjacent neurovascular structures is possible. It is imperative that the radiologist and skull base surgeons are familiar with this complex anatomy for localizing the skull base lesion, reaching appropriate differential diagnosis, and deciding the optimal surgical approach. CT and MRI are complementary to each other and are often used together for the demonstration of the full disease extent. This article focuses on the radiological anatomy of the skull base and discusses few of the common pathologies affecting the skull base. Key words: Computed tomography; magnetic resonance imaging; skull base Introduction The skull base is composed of five bones: (1) ethmoid, (2) sphenoid, (3) occipital, (4) paired temporal, and (5) paired The skull base forms the floor of the cranial cavity that frontal bones. Three naturally contoured regions can be separates brain from facial structures and suprahyoid identified when skull base is viewed from above [Figure 1]. -

Anatomical Variations of Foramen Ovale Deepti Anna John, .Thenmozhi Saveetha Dental College, Chennai
Deepti Anna John et al /J. Pharm. Sci. & Res. Vol. 7(6), 2015, 327-329 Anatomical Variations of Foramen ovale Deepti Anna John, .Thenmozhi Saveetha Dental College, Chennai Abstract: The Foramen Ovale is found at the posterior part of the greater wing of sphenoid, it is one of the larger holes present in the Skull, through which many nerves pass. The foramen ovale has important clinical significance in neurological procedures.To locate and identify the various osseous structures and different shapes of foramen Ovale in across different skulls.To obtain dry skulls of unknown sex from the Department of Anatomy, Saveetha Dental College and Hospitals and observe the presence of the accessory bony structures such as Tubercles,spine and bony plates and the variants in the shape of foramen ovale.To collect data about the prevalence of these projections and variants in the shape of the foramen ovale .Anatomical knowledge of the variations of foramen ovale is important for neurosurgeons. Key Words:Foramen ovale,variations,bony outgrowths, mandibular nerve INTRODUCTION: the presence of a bony plate. Incidences of Spine, Tubercle The foramen ovale is an important foramen present in the and Bony plate were 13%, 6% and 11.6% respectively. middle cranial fossa.It is seen in the infratemporal surface of greater wing of the sphenoid bone, present lateral to the Table 1: Variations in Appearance of Foramen Ovale foramen rotundum. The mandibular nerve, accessory Total Shape Right(n=30) Left(n=30) meningeal artery, emissary vein and the lesser petrosal vein -

Pharynx, Larynx, Nasal Cavity and Pterygopalatine Fossa
Pharynx, Larynx, Nasal cavity And Pterygopalatine Fossa Mikel H. Snow, Ph.D. Dental Anatomy [email protected] July 29, 2018 Pharynx Food & Air Passage Pharynx The pharynx is a skeletal muscle tube that opens anteriorly with 3 regions. The upper part communicates with nasal cavity, the middle communicates with oral cavity, and the lower communicates with the larynx. Nasal cavity Nasal Oral cavity cavity Larynx Air Nasopharynx: between Oral sphenoid sinus & uvula Food/ cavity Oropharynx: between uvula & epiglottis drink Laryngopharynx: between epiglottis & esophagus Esophagus Trachea The posterior and lateral walls are 3 skeletal muscles (constrictors) that propel food/liquid inferiorly to the esophagus. Constrictors innervated by CNX. Additional muscles elevate the pharynx (stylopharyngeus is external). Stylopharyngeus innervated by CNIX. Stylopharyngeus Superior constrictor Middle constrictor Inferior constrictor Two additional internal muscles we’ll get to later… Key relationship: Glossopharyngeal nerve wraps around stylopharyngeus muscle. CN IX wraps around stylopharyngeus muscle and Stylopharyngeus innervates it. Pharyngeal constrictors Pharynx Interior 1 Nasopharynx: 1. Pharyngeal tonsils 2. Auditory tube ostia 2 3 3. Salpingopharyngeal fold 4 4 Oropharynx: 4. Palatine tonsils 5 5 Laryngopharynx: Slit open 5. Piriform recess constrictors to examine interior Lateral Wall of Pharynx 5. Salpingopharyngeus muscle 6. Levator veli palatini muscle 1. Pharyngeal tonsils 7. Tensor veli palatini muscle 2. Torus tubarius 8. Palatine tonsil 3.