Interrelationships of the Anterior Pituitary and Thyroid Glands
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Human General Histology
135 اووم څپرکي انډوکراين سيستم (Endocrine system) (hormones) (target cells) (receptors) autonomic (sinusoids) ductless glands thyroid gland Pineal gland Hypophysis cerebri(pituitary glands) supra renal( adrenal glands) parathyroid glands 136 اووم څپرکي انډوکراين سيسټم islets cell corpora lutea interstitial tissue (placenta) GIT amines neurotransmitters amines neuromodulator 137 اووم څپرکي انډوکراين سيسټم APUD cells neuroendocrine system system adrenaline, (amino acid derivatives) thyroxin noradrenalin thyroid vasopressin encephalin (small peptides) releasing hormone(TRH) TSH(thyroid stimulating parathormone hormone) cortisol Testosterone estrogen (steroids) 5,12,3 (Hypophysis Cerebri) (brain) pituitary gland (stalk) Ventricle infundibulum stalk pituitary fossa sphenoid pineal hypothalamus body 138 اووم څپرکي انډوکراين سيسټم Hypophysis cerebri Pars pars anterior pars nervosa pars posterior intermediate hypothalamus infundibulum infundibulum stalk )Pars posterior neurohypophysis median eminence (tuber cinereum) infundibulum pars neurohypophysis median eminence pars intermediate pars distalis anterior Adenohypophysis infundibulum pars anterior pars tuberalis adenohypophysis 139 اووم څپرکي انډوکراين سيسټم Adenohypophysis pars intermediate pars anterior adenohypophyisis Pars anterior fenestrated sinusoids (cords) chromophil chromophobic acidophil chromophil basophils orange G eosin PAS-positive hematoxylline Beta cells basophil Alpha cells Acidophil basophils acidophil (dese cored vesicles) alpha Beta Histochemical 140 اووم څپرکي انډوکراين -

1-Anatomy of the Pituitary Gland
Color Code Important Anatomy of Pituitary Gland Doctors Notes Notes/Extra explanation Please view our Editing File before studying this lecture to check for any changes. Objectives At the end of the lecture, students should be able to: ✓ Describe the position of the pituitary gland. ✓ List the structures related to the pituitary gland. ✓ Differentiate between the lobes of the gland. ✓ Describe the blood supply of pituitary gland & the hypophyseal portal system. الغدة النخامية Pituitary Gland (also called Hypophysis Cerebri) o It is referred to as the master of endocrine glands. o It is a small oval structure 1 cm in diameter. o It doubles its size during pregnancy. lactation ,(الحمل) pregnancy ,(الحيض) A women experiences changes in her hormone levels during menstruation But only the pituitary gland will only increase in size during pregnancy .(سن اليأس) and menopause ,(الرضاعة) X-RAY SKULL: LATERAL VIEW SAGITTAL SECTION OF HEAD & NECK Extra Pituitary Gland Position o It lies in the middle cranial fossa. o It is well protected in sella turcica* (hypophyseal fossa) of body of sphenoid o It lies between optic chiasma (anteriorly) & mamillary bodies** (posteriorly). Clinical point: *سرج الحصان Anterior to the pituitary gland is the optic chiasm, so if there was a tumor in the pituitary gland or it was ** Part of hypothalamus enlarged this could press on the chiasm and disrupt the patients vision (loss of temporal field). Extra Pictures The purple part is the sphenoid bone Hypophyseal fossa Pituitary Gland The relations are important Important Relations • SUPERIOR: Diaphragma sellae: A fold of dura mater covers the pituitary gland & has an opening for passage of infundibulum (pituitary stalk) connecting the gland to hypothalamus. -

The Physiology of Growth by S
Postgrad Med J: first published as 10.1136/pgmj.26.298.417 on 1 August 1950. Downloaded from 417 THE PHYSIOLOGY OF GROWTH BY S. LEONARD SIMPSON, M.A., M.D., F.R.C.P. Consultant Endocrinologist, St. Mary's Hospital, etc.; Formerly Research Wor7Aer, Lister Institute Although clinical and experimental evidence postulated an antagonism between growth and had previously indicated that skeletal growth sex-stimulating hormones. Further observations depended upon the pituitary gland, it was not suggested that corpora lutea were formed before until I92I that Evans and Long, at the University ovulation occurred, and that his emulsions con- of California, demonstrated that a saline emulsion tained gonadotrophic luteinizing hormone. Al- made from the anterior pituitary lobe of fresh though Evans' original giant rats were apparently glands of cattle contained a growth hormone. The adipose, later work (Lee and Schaffer, 1934), hypophyses were thrown into 40 per cent. ethyl showed that there was a retention of nitrogen and alcohol, agitated with a glass rod, transferred to a relative excess of body protein. This was also two changes of sterile normal saline, and triturated true of the excess of tissue deposited in and with force and speed with ocean sand, diluted with around the abdomen. Evans stated in a recent saline, and decanted. The layers of sand, cell discussion in London that rats treated with pure fragments and opaque pink fluid permitted the growth hormone, unlike those in the initial latter to be decanted. This emulsion, when experiments with crude extracts, were not injected daily in doses of I to i ml. -
Endocrinology Review – Adrenal and Thyroid Disorders
FOCUS: ENDOCRINOLOGY Endocrinology Review – Adrenal and Thyroid Disorders LINDA S. GORMAN, JANELLE M. CHIASERA LEARNING OBJECTIVES This article represents the first of three articles focusing 1. Define endocrinology and list the major endocrine on the endocrine system. The first article will provide glands of the body. you with fundamental theory regarding the endocrine system that will serve as a basis for understanding the 2. Explain how feedback (positive and negative) Downloaded from promotes maintenance of normal levels of next two articles focusing on two specific endocrine hormones. glands, the thyroid and adrenal glands. 3. Differentiate between steroid and peptide hormones with regard to their mechanism of Endocrinology is the branch of medical science that action. deals with the endocrine system, a system that consists 4. Provide examples of peptide and steroid hormones. of several glands located in different parts of the body http://hwmaint.clsjournal.ascls.org/ 5. Explain how endocrine disorders are categorized. that secrete hormones directly into the bloodstream. Although every organ system in the body may respond ABBREVIATIONS: ACTH - adrenocorticotropic hor- to hormones, endocrinology focuses specifically on mone; ADH - antidiuretic hormone; CRH – cortico- endocrine glands whose primary function is hormone tropin releasing hormone; DHEA – dehydroepian- secretion. Major endocrine glands include the pituitary drosterone; FSH - follicle stimulating hormone; GHRH (anterior and posterior), hypothalamus, thyroid, - growth hormone -

Quantitation of Corticotrophs in the Pars Distalis of Stress-Prone Swine Beverly Ann Bedford Iowa State University
Iowa State University Capstones, Theses and Retrospective Theses and Dissertations Dissertations 1-1-1976 Quantitation of corticotrophs in the pars distalis of stress-prone swine Beverly Ann Bedford Iowa State University Follow this and additional works at: https://lib.dr.iastate.edu/rtd Part of the Veterinary Anatomy Commons Recommended Citation Bedford, Beverly Ann, "Quantitation of corticotrophs in the pars distalis of stress-prone swine" (1976). Retrospective Theses and Dissertations. 17953. https://lib.dr.iastate.edu/rtd/17953 This Thesis is brought to you for free and open access by the Iowa State University Capstones, Theses and Dissertations at Iowa State University Digital Repository. It has been accepted for inclusion in Retrospective Theses and Dissertations by an authorized administrator of Iowa State University Digital Repository. For more information, please contact [email protected]. Quantitation of corticotrophs in the pars distalis of stress-prone swine by Beverly Ann Bedford A Thesis Submitted to the Graduate Faculty in Partial Fulfillment of The Requirements for the Degr~e of MASTER OF SCIENCE Department: Veterinary Anatomy, Pharmacology and Physiology Major: Veterinary Anatomy ., Signatures have been redacted for privacy ' I Iowa State University Ames, Iowa 1976 ii :E5 ll I q7(p ,g3r TABLE OF CONTENTS c,J. Page INTRODUCTION 1 LITERATURE REVIEW 4 Pituitary Gland 4 General morphology 4 Development 5 Blood supply 7 Staining techniques 7 Pars distalis 13 . Pars tuberalis 25 ·pars intermedia 28 Process of secretion 36 Neurohypophysis 41 Porcine Stress Syndrome 45 MATERIALS AND MET!iODS' 52 RESULTS 56 DISCUSSION 64 SUMMARY AND CONCLUSIONS 72 BIBLIOGRAPHY 73 ACKNOWLEDGMENTS 85 APPENDIX 86 1111408 1 INTRODUCTION As early as 1953, there came reports (Ludvigsen, 1953; Briskey et al., 1959) of pale soft exudative (PSE) post-mortem porcine muscu- lature which later stimulated research into the mechanisms responsible for this condition. -

Relation of the Anterior Pituitary to Ovarian Function
University of Nebraska Medical Center DigitalCommons@UNMC MD Theses Special Collections 5-1-1934 Relation of the anterior pituitary to ovarian function Clyde S. Martin University of Nebraska Medical Center This manuscript is historical in nature and may not reflect current medical research and practice. Search PubMed for current research. Follow this and additional works at: https://digitalcommons.unmc.edu/mdtheses Part of the Medical Education Commons Recommended Citation Martin, Clyde S., "Relation of the anterior pituitary to ovarian function" (1934). MD Theses. 621. https://digitalcommons.unmc.edu/mdtheses/621 This Thesis is brought to you for free and open access by the Special Collections at DigitalCommons@UNMC. It has been accepted for inclusion in MD Theses by an authorized administrator of DigitalCommons@UNMC. For more information, please contact [email protected]. e .,.,.~, THE RELATION OF THE ANTERIOR PITUITARY TO OVARIAN FUNCTION BY CLYDE S. MARTIN SE!HOR THESIS UNIVERSITY OF NEBRASKA SCHOOL OF MEDICINE APRIL I934 THE RELATIOM OF THE ANTERIOR PITUITARY TO OV ARIAJ.T FUNCTION !n ~be last ten years especially, there has been demonstrated and proved, a definite relationship between the pituitary and the sex glands. This is of importance to every clinician, and gynecologist. In order to understand these various phenomena produced by the internal secretion of the pituitary, it is advisable to give here a brief discussion of the anatomical structure, with slight reference to histology. ANATOMY A~TD HI~TOLOGY The pituitary body is situated in the cranium a.t the base of the brain, surrounded by a bony encasement the sella turcica. -
Unit-4 Structure and Functions of Pituitary Gland
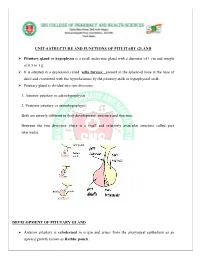
UNIT-4 STRUCTURE AND FUNCTIONS OF PITUITARY GLAND Pituitary gland or hypophysis is a small endocrine gland with a diameter of 1 cm and weight of 0.5 to 1 g. It is situated in a depression called ‘sella turcica’, present in the sphenoid bone at the base of skull and connected with the hypothalamus by the pituitary stalk or hypophyseal stalk. Pituitary gland is divided into two divisions: 1. Anterior pituitary or adenohypophysis 2. Posterior pituitary or neurohypophysis. Both are entirely different in their development, structure and function. Between the two divisions, there is a small and relatively avascular structure called pars intermedia. DEVELOPMENT OF PITUTARY GLAND Anterior pituitary is ectodermal in origin and arises from the pharyngeal epithelium as an upward growth known as Rathke pouch. Posterior pituitary is neuroectodermal in origin and arises from hypothalamus as a downward diverticulum. Rathke pouch and the downward diverticulum from hypothalamus grow towards each other and meet in the midway between the roof of the buccal cavity and base of brain. There, the two structures lie close together. ANTERIOR PITUITARY OR ADENOHYPOPHYSIS Anterior pituitary is also known as the master gland because it regulates many other endocrine glands through its hormones. Anterior pituitary consists of three parts 1. Pars distalis 2. Pars tuberalis 3. Pars intermedia. Anterior pituitary has two types of cells 1. Chromophobe cells 2. Chromophil cells. Chromophobe Cells Chromophobe cells are not secretory in nature, but are the precursors of chromophil cells. Chromophil Cells On the basis of secretory nature chromophil cells are classified into five types: i. -

2. Endocrine Control of the Oestrous Cycle
2. ENDOCRINE CONTROL OF THE OESTROUS CYCLE Introduction 2.1 The cyclic changes that occur in the female reproductive tract are initiated and regulated by the hypothalamic-pituitary-ovarian (HPO) axis. Although folliculogenesis occurs independently of hormonal stimulation up until the formation of early tertiary follicles, the gonadotrophins luteinising hormone (LH) and follicle stimulating hormone (FSH) are essential for the completion of follicular maturation and development of mature preovulatory (Graafian) follicles. The sites of production and key functions of the major reproductive hormones in the female rat are summarised in Table 2.1. Pituitary gonadotrophin secretion drives follicular maturation and oestrogen secretion 2.2 Levels of LH and FSH begin to increase just after dioestrus. Both hormones are secreted by the same secretory cells (gonadotrophs) in the pars distalis of the anterior pituitary (adenohypophysis). FSH stimulates development of the zona granulosa and triggers expression of LH receptors by granulosa cells. LH initiates the synthesis and secretion of androstenedione and, to a lesser extent, testosterone by the theca interna; these androgens are utilised by granulosa cells as substrates in the synthesis of oestrogen. Pituitary release of gonadotrophins thus drives follicular maturation and secretion of oestrogen during prooestrus. 2.3 Gonadotrophin secretion by the anterior pituitary is regulated by luteinising hormone-releasing hormone (LHRH), produced by the hypothalamus. LHRH is transported along the axons of hypothalamic neurones to the median eminence where it is secreted into the hypothalamic-hypophyseal portal system and transported to the anterior pituitary. The hypothalamus secretes LHRH in rhythmic pulses; this pulsatility is essential for the normal activation of gonadotrophs and subsequent release of LH and FSH. -

Endocrine System Hormonal Regulation Endocrine Glands
Endocrine system Hormonal regulation Endocrine glands • Glands w/o ducts • Secretory cells release their products, hormones, into the extracellular space and blood stream • Alternatively, the hormones may affect neighbor cells (paracrine) • Structure: • c.t. – capsule + septs • irregular clumps or cords of the cells • network of capillaries • fenestrated capillaries • sinusoids Hypophysis – pituitary gland Pituitary gland – anterior pituitary Pituitary gland – anterior pituitary Chromophil cells - Acidophilic cells (produce proteins) somatotrophs mammotrophs (or lactotrophs) - Basophilic cells (produce glycoproteins) thyrotrophs produce thyroid stimulating hormone (TSH or thyrotropin). gonadotrophs produce follicle stimulating hormone (FSH) and luteinizing hormone (LH) corticotrophs (or adrenocorticolipotrophs) Chromophobe cells Adenohypophysis Adenohypophysis oranž G + PAS Neurohypophysis x Adenohypophysis Neurohypophysis - structure Structure unmyelinated nerve fibres derived from neurosecretory cells of the supraoptic and paraventricular hypothalamic nuclei pituicytes /neuroglia/ Function Two hormones are oxytocin, which stimulates the contraction of smooth muscle cell in the uterus and participates in the milk ejection reflex, and antidiuretic hormone (ADH or vasopressin), which facilitates the concentration of urine in the kidneys and, thereby, the retention of water. Usually only the oval or round nuclei of the pituicytes are visible. Hypothalamic nerve fibres typically terminate close to capillaries. Scattered, large -

1 General Overview of the Endocrine System Questions to Be Thinking
General Overview of the Endocrine System Questions to be thinking about to help organize your learning of the components of the Endocrine System: Anatomy 1) Where are the different hormone producing cells located? 2) What hormone does a particular type of endocrine cell or neuron produce? General Overview of the Endocrine System Questions to be thinking about to help organize your learning of the components of the Endocrine System: Hormones 1) What is their general chemical structure? 2) How does their structure affect their function? 3) Where are they produced? 4) What environmental or physiological stimuli regulate their production and secretion? 5) Is their production and secretion under direct neural or hormonal control? 6) What are their targets? 7) What effects do they produce on their targets? 8) How do they produce their effects on their targets (how is the signal transduced? i.e. receptor mechanisms) 1 Often endocrine cells are clumped together into a well defined gland (e.g. pituitary, thyroid, adrenal, testes, ovaries), but not always (e.g. gut, liver, lung). Often endocrine cells are clumped together into a well defined gland (e.g. pituitary, thyroid, adrenal, testes, ovaries), but not always (e.g. gut, liver, lung). Remember, it's cells that produce hormones, not glands. Although many glands secrete more than one type of hormone, most neurons or endocrine cells only produce one type of hormone (there are a few exceptions). 2 Some Terminology Neurohormone: a hormone that is produced by a neuron Some Terminology All of the hormones we discuss can be classified as belonging to one of 2 general functional categories: 1] Releasing hormone (or factors) — hormone that acts on endocrine cells to regulate the release of other hormones. -

Major Endocrine Glands of the Body Pineal Gland Pituitary Gland
Pituitary and Thyroid Hormones 1 Topics for today: • Anterior pituitary hormones • Posterior pituitary hormones • Portal system & releasing factors • Structure of thyroid gland • Action of thyroid hormones 2 Major endocrine glands of the body pineal gland pituitary gland parathyroid glands thyroid gland adrenal glands thymus gland pancreas ovaries (female) testes (male) 3 1 Hydrophilic hormone action mechanism cytoplasm Extracellular fluid second messenger hormone Multiple effects in the cell membrane receptor 4 Example: Action of Epinephrine 5 Pituitary/hypothalamus axis ...interaction of nervous system & endocrine system 6 2 Pituitary secretions neurosecretory cells anterior pituitary in hypothalamus - TSH - ACTH - growth hormone posterior pituitary - FSH - oxytocin - luteining hormone - antidiuretic hormone - prolactin 7 Pituitary secretions neurosecretory cells anterior pituitary in hypothalamus - TSH - ACTH - growth hormone posterior pituitary - FSH - oxytocin - luteining hormone - antidiuretic hormone - prolactin 8 Physiologic effects of hormones from the anterior pituitary • TSH - stimulates release of hormones from thyroid • ACTH - stimulates release of hormones from adrenal cortex • growth hormone - stimulate growth of somatic tissues • FSH - stimulates gamete formation and follicle development • luteining hormone - affects corpus luteum & Leydig cells • prolactin - stimulates development of mammary ductules 9 3 Physiologic effects of hormones from the posterior pituitary •ADH - increases reabsorption of water from kidney tubules -

The Endocrine System Dr
The Endocrine System Dr. Ali Ebneshahidi Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Endocrine System . The endocrine system interacts with the nervous system to coordinate and integrate body activities by means of hormones . Endocrine tissues and organs secrete hormone into body fluids (mainly blood and lymph) directly using diffusion. Exocrine tissues, such as salivary glands, and sebaceous glands, secrete chemical substances through ducts into an open space. Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Five major functions of hormones . a) Regulate metabolic processes (e.g. thyroid hormones). b) Control the rate of chemical reactions (e.g. growth hormone). c) Aid in the transport of substances across the cell membrane of target cells (e.g. insulin and glucagon). d) Regulate water and electrolyte balances (e.g. antidiurectic hormone, calcitonin, and aldosterone). e) Play a vital role in reproduction, growth and development (e.g. estrogens , progesterone, and testosterone). Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Major Endocrine Organs Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Chemistry of Hormones . Hormones are organic compounds secreted by endocrine glands, that have a potent effect in target cells Two types of hormones: . a) Protein hormones: made of amino acids joined by peptide bonds. fat – insoluble; as a result cannot diffuse across the membrane of target cells . most hormones belong to this group except hormones secreted by the gonads (testis and ovary) and the adrenal cortex. b) Steroid hormones: made of fatty acids using cholesterol as a functional group. Fat-soluble; as a result can diffuse into target cells .