Suprarenocortical Syndrome and Pituitary Basophilism
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Morphology and Histology of a Certain Structure Connected with the Pars Intermedia of the Pituitary Body Ofthe Ox1
THE MORPHOLOGY AND HISTOLOGY OF A CERTAIN STRUCTURE CONNECTED WITH THE PARS INTERMEDIA OF THE PITUITARY BODY OFTHE OX1 ROSALIND \VULZEX From the Hearst Anatomical Laboratory oj the University oj California SEVENTEEN FIGURES Certain physiological experiments are now being conducted in the Rudolph Spreckels Physiological Laboratory of this University which necessitate the separation of a great number of ox pituitaries into their two main divisions. As an interesting anatomical feature was in this way brought to our attention the material was used in addition for this anatomical study. This feature has not been mentioned by the following who have written more or less fully upon the pituitary body of the ox, Peremeschko ('67), Dostojewski ('86), Herring ('08)' and Traut- mann ('11). The pituitary body of the ox, like that of other vertebrates, is composed of two distinct portions. One, the pars nervosa, is derived from the brain as an outgrowth of the hypothalamus. The other originates as a hollow buccal evagination which in time is completely separated from the digestive tract. That portion of this evagination which comes into contact with the pars nervosa is called the pars intermedia. It is a comparatively thin sheet of epithelium which spreads as a coating over much Material amounting to thousands of pituitary bodies was most kindly sup- plied by the Oakland Meat and Packing Company through the courtesy of the Superintendent. It was derived from cows, bulls and steers. As the cone struc- ture was present indifferently in these three varieties, its appearance can have little to do with sex or castration. -

Human General Histology
135 اووم څپرکي انډوکراين سيستم (Endocrine system) (hormones) (target cells) (receptors) autonomic (sinusoids) ductless glands thyroid gland Pineal gland Hypophysis cerebri(pituitary glands) supra renal( adrenal glands) parathyroid glands 136 اووم څپرکي انډوکراين سيسټم islets cell corpora lutea interstitial tissue (placenta) GIT amines neurotransmitters amines neuromodulator 137 اووم څپرکي انډوکراين سيسټم APUD cells neuroendocrine system system adrenaline, (amino acid derivatives) thyroxin noradrenalin thyroid vasopressin encephalin (small peptides) releasing hormone(TRH) TSH(thyroid stimulating parathormone hormone) cortisol Testosterone estrogen (steroids) 5,12,3 (Hypophysis Cerebri) (brain) pituitary gland (stalk) Ventricle infundibulum stalk pituitary fossa sphenoid pineal hypothalamus body 138 اووم څپرکي انډوکراين سيسټم Hypophysis cerebri Pars pars anterior pars nervosa pars posterior intermediate hypothalamus infundibulum infundibulum stalk )Pars posterior neurohypophysis median eminence (tuber cinereum) infundibulum pars neurohypophysis median eminence pars intermediate pars distalis anterior Adenohypophysis infundibulum pars anterior pars tuberalis adenohypophysis 139 اووم څپرکي انډوکراين سيسټم Adenohypophysis pars intermediate pars anterior adenohypophyisis Pars anterior fenestrated sinusoids (cords) chromophil chromophobic acidophil chromophil basophils orange G eosin PAS-positive hematoxylline Beta cells basophil Alpha cells Acidophil basophils acidophil (dese cored vesicles) alpha Beta Histochemical 140 اووم څپرکي انډوکراين -

The Physiology of Growth by S
Postgrad Med J: first published as 10.1136/pgmj.26.298.417 on 1 August 1950. Downloaded from 417 THE PHYSIOLOGY OF GROWTH BY S. LEONARD SIMPSON, M.A., M.D., F.R.C.P. Consultant Endocrinologist, St. Mary's Hospital, etc.; Formerly Research Wor7Aer, Lister Institute Although clinical and experimental evidence postulated an antagonism between growth and had previously indicated that skeletal growth sex-stimulating hormones. Further observations depended upon the pituitary gland, it was not suggested that corpora lutea were formed before until I92I that Evans and Long, at the University ovulation occurred, and that his emulsions con- of California, demonstrated that a saline emulsion tained gonadotrophic luteinizing hormone. Al- made from the anterior pituitary lobe of fresh though Evans' original giant rats were apparently glands of cattle contained a growth hormone. The adipose, later work (Lee and Schaffer, 1934), hypophyses were thrown into 40 per cent. ethyl showed that there was a retention of nitrogen and alcohol, agitated with a glass rod, transferred to a relative excess of body protein. This was also two changes of sterile normal saline, and triturated true of the excess of tissue deposited in and with force and speed with ocean sand, diluted with around the abdomen. Evans stated in a recent saline, and decanted. The layers of sand, cell discussion in London that rats treated with pure fragments and opaque pink fluid permitted the growth hormone, unlike those in the initial latter to be decanted. This emulsion, when experiments with crude extracts, were not injected daily in doses of I to i ml. -

Quantitation of Corticotrophs in the Pars Distalis of Stress-Prone Swine Beverly Ann Bedford Iowa State University
Iowa State University Capstones, Theses and Retrospective Theses and Dissertations Dissertations 1-1-1976 Quantitation of corticotrophs in the pars distalis of stress-prone swine Beverly Ann Bedford Iowa State University Follow this and additional works at: https://lib.dr.iastate.edu/rtd Part of the Veterinary Anatomy Commons Recommended Citation Bedford, Beverly Ann, "Quantitation of corticotrophs in the pars distalis of stress-prone swine" (1976). Retrospective Theses and Dissertations. 17953. https://lib.dr.iastate.edu/rtd/17953 This Thesis is brought to you for free and open access by the Iowa State University Capstones, Theses and Dissertations at Iowa State University Digital Repository. It has been accepted for inclusion in Retrospective Theses and Dissertations by an authorized administrator of Iowa State University Digital Repository. For more information, please contact [email protected]. Quantitation of corticotrophs in the pars distalis of stress-prone swine by Beverly Ann Bedford A Thesis Submitted to the Graduate Faculty in Partial Fulfillment of The Requirements for the Degr~e of MASTER OF SCIENCE Department: Veterinary Anatomy, Pharmacology and Physiology Major: Veterinary Anatomy ., Signatures have been redacted for privacy ' I Iowa State University Ames, Iowa 1976 ii :E5 ll I q7(p ,g3r TABLE OF CONTENTS c,J. Page INTRODUCTION 1 LITERATURE REVIEW 4 Pituitary Gland 4 General morphology 4 Development 5 Blood supply 7 Staining techniques 7 Pars distalis 13 . Pars tuberalis 25 ·pars intermedia 28 Process of secretion 36 Neurohypophysis 41 Porcine Stress Syndrome 45 MATERIALS AND MET!iODS' 52 RESULTS 56 DISCUSSION 64 SUMMARY AND CONCLUSIONS 72 BIBLIOGRAPHY 73 ACKNOWLEDGMENTS 85 APPENDIX 86 1111408 1 INTRODUCTION As early as 1953, there came reports (Ludvigsen, 1953; Briskey et al., 1959) of pale soft exudative (PSE) post-mortem porcine muscu- lature which later stimulated research into the mechanisms responsible for this condition. -
Unit-4 Structure and Functions of Pituitary Gland
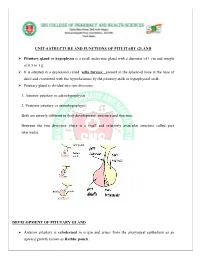
UNIT-4 STRUCTURE AND FUNCTIONS OF PITUITARY GLAND Pituitary gland or hypophysis is a small endocrine gland with a diameter of 1 cm and weight of 0.5 to 1 g. It is situated in a depression called ‘sella turcica’, present in the sphenoid bone at the base of skull and connected with the hypothalamus by the pituitary stalk or hypophyseal stalk. Pituitary gland is divided into two divisions: 1. Anterior pituitary or adenohypophysis 2. Posterior pituitary or neurohypophysis. Both are entirely different in their development, structure and function. Between the two divisions, there is a small and relatively avascular structure called pars intermedia. DEVELOPMENT OF PITUTARY GLAND Anterior pituitary is ectodermal in origin and arises from the pharyngeal epithelium as an upward growth known as Rathke pouch. Posterior pituitary is neuroectodermal in origin and arises from hypothalamus as a downward diverticulum. Rathke pouch and the downward diverticulum from hypothalamus grow towards each other and meet in the midway between the roof of the buccal cavity and base of brain. There, the two structures lie close together. ANTERIOR PITUITARY OR ADENOHYPOPHYSIS Anterior pituitary is also known as the master gland because it regulates many other endocrine glands through its hormones. Anterior pituitary consists of three parts 1. Pars distalis 2. Pars tuberalis 3. Pars intermedia. Anterior pituitary has two types of cells 1. Chromophobe cells 2. Chromophil cells. Chromophobe Cells Chromophobe cells are not secretory in nature, but are the precursors of chromophil cells. Chromophil Cells On the basis of secretory nature chromophil cells are classified into five types: i. -

Light and Electron Microscopic Observations on the Anterior Pituitary of the Mouse Injected with Dl-Thyroxine By
Okajimas Fol. anat. jap., 43: 21-51, 1967 Light and Electron Microscopic Observations on the Anterior Pituitary of the Mouse injected with dl-Thyroxine By Tomiji Uchida Department of Anatomy, Nagoya University School of Medicine, Nagoya, Japan (Director : Prof. Dr. Ka z u m a r o Y a m ad a) Introduction Probably, the first suggestion of the existence of a functional relationship between the thyroid and hypophysis was given by Niepce (1851) who described pituitary enlargement in a series of goitrous cretins. Since then numerous studies have provided detailed evidence of this relationship. The reciprocal interrelationship be- tween thyroid stimulating hormone (TSH) secretion in the anterior hypophysis and the circulating levels of thyroid hormone has been well established, and in general, procedures which reduce effective plasma concentrations of thyroid hormone increase thyrotrophic hormone release in the anterior pituitary, whereas increased circulat- ing levels of thyroxine inhibit thyrotophic hormone secretion. This negative feedback mechanism resides both in the level of the pituitary and of a hypothalamic " TSH releasing center " (S o 1 o m on and Dowling, '60). Earlier views (Ma rin e, Rosen and Spar k, '35; Morris, '52) favored pituitary acidophile cell as the source of thyrotrophic hormone, but results of many recent studies implicate the basophile cell (Zeckwer, '38a and '38b; Griesbach and Purves, '45 Pur v es and Griesbac h, '46a, '46b, '51a, '51b, '51c, '57a and '57b; Goldberg and Chaikoff, '50; Salter, '50, Halmi, '50, '51, '52a , '52b, and 52c ; R ennel s, '53; Halm i and G u d e, '54 D'Angelo, '53 and '55; Knigge, '55; Elf tman, '58; Mura - s h i m a, '60 and others). -
Introduction to Geomicrobiology
ITGA01 18/7/06 18:06 Page iii Introduction to Geomicrobiology Kurt Konhauser ITGC03 18/7/06 18:11 Page 93 3 Cell surface reactivity and metal sorption One of the consequences of being extremely 3.1 The cell envelope small is that most microorganisms cannot out swim their surrounding aqueous environment. Instead they are subject to viscous forces that 3.1.1 Bacterial cell walls cause them to drag around a thin film of bound water molecules at all times. The im- Bacterial surfaces are highly variable, but one plication of having a watery shell is that micro- common constituent amongst them is a unique organisms must rely on diffusional processes material called peptidoglycan, a polymer con- to extract essential solutes from their local sisting of a network of linear polysaccharide milieu and discard metabolic wastes. As a (or glycan) strands linked together by proteins result, there is a prime necessity for those cells (Schleifer and Kandler, 1972). The backbone to maintain a reactive hydrophilic interface. of the molecule is composed of two amine sugar To a large extent this is facilitated by having derivatives, N-acetylglucosamine and N-acetyl- outer surfaces with anionic organic ligands and muramic acid, that form an alternating, and high surface area:volume ratios that provide repeating, strand. Short peptide chains, with four a large contact area for chemical exchange. or five amino acids, are covalently bound to some Most microorganisms further enhance their of the N-acetylmuramic acid groups (Fig. 3.1). chances for survival by growing attached to They serve to enhance the stability of the submerged solids. -

Endocrine System Hormonal Regulation Endocrine Glands
Endocrine system Hormonal regulation Endocrine glands • Glands w/o ducts • Secretory cells release their products, hormones, into the extracellular space and blood stream • Alternatively, the hormones may affect neighbor cells (paracrine) • Structure: • c.t. – capsule + septs • irregular clumps or cords of the cells • network of capillaries • fenestrated capillaries • sinusoids Hypophysis – pituitary gland Pituitary gland – anterior pituitary Pituitary gland – anterior pituitary Chromophil cells - Acidophilic cells (produce proteins) somatotrophs mammotrophs (or lactotrophs) - Basophilic cells (produce glycoproteins) thyrotrophs produce thyroid stimulating hormone (TSH or thyrotropin). gonadotrophs produce follicle stimulating hormone (FSH) and luteinizing hormone (LH) corticotrophs (or adrenocorticolipotrophs) Chromophobe cells Adenohypophysis Adenohypophysis oranž G + PAS Neurohypophysis x Adenohypophysis Neurohypophysis - structure Structure unmyelinated nerve fibres derived from neurosecretory cells of the supraoptic and paraventricular hypothalamic nuclei pituicytes /neuroglia/ Function Two hormones are oxytocin, which stimulates the contraction of smooth muscle cell in the uterus and participates in the milk ejection reflex, and antidiuretic hormone (ADH or vasopressin), which facilitates the concentration of urine in the kidneys and, thereby, the retention of water. Usually only the oval or round nuclei of the pituicytes are visible. Hypothalamic nerve fibres typically terminate close to capillaries. Scattered, large -

On the Staining Capacity of the Nucleolus and Its Physiological Significance
On the Staining Capacity of the Nucleolus and its Physiological Significance. By Kunio Sato. Department of Anatomy. Okayama Medical college, (Director: Prof. K. Kosaka.) With 7 text figures. Contents. Introduction 717 Historical. ......• 717 Material and methods........ 719 Staining character of the Nucleolus 720 a. Fixingfluids 720 b. Stains.. .............•. 721 Relation ofthe Nucleolus to Reagents .. 726 Nucleoli inVariousDevelopmental Stages......Developmental 728 Comments...... .......... 731 Conclusions ..... .. 735 Introduction. Since the discovery of the nucleolus in nucleus b Fontana (1781), a host of investigators have striven to find its physiological significance and the origin of its peculiar stainability. To our regret, however, we have not as yet arrived at an acceptable conclusion ; some take it for a metabolic product with little significance to cell functions, while others think that it is a most important reservoir or pre-substance of chromatin, being stained partly acidophilously and partly basophilously. Still others consider it nothing other than a crystalloid. At the Institute of Anatomy Prof. KO saka suggested me to attack the nucleolus problem from its staining capacity, and in the following pages I shall describe some of my results. Historical. Carnoy and Lebrun (1897-1899), Nussbaum (1913), Lubosch 718 Kunio sato, (1914), Wagner (1923) et al. found double stainability of the nucleolus (germinal spot) and maintain that the nucleolus is acidophilic but its peripheral portion may be basophilic, although this condition varies a great deal according to the different kinds and physiologic phases of cells. What was said of the egg cells is also confirmed in the somatic cells. Macklin . (MO found that the nucleolus of connective tissue cell very finely stained by haematoxylin and gentian violet. -

A Histological and Histochemical Study of Transplanted Pituitary Glands in Mice Thomas Warner Tillack Yale University
Yale University EliScholar – A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine 1963 A histological and histochemical study of transplanted pituitary glands in mice Thomas Warner Tillack Yale University Follow this and additional works at: http://elischolar.library.yale.edu/ymtdl Recommended Citation Tillack, Thomas Warner, "A histological and histochemical study of transplanted pituitary glands in mice" (1963). Yale Medicine Thesis Digital Library. 3248. http://elischolar.library.yale.edu/ymtdl/3248 This Open Access Thesis is brought to you for free and open access by the School of Medicine at EliScholar – A Digital Platform for Scholarly Publishing at Yale. It has been accepted for inclusion in Yale Medicine Thesis Digital Library by an authorized administrator of EliScholar – A Digital Platform for Scholarly Publishing at Yale. For more information, please contact [email protected]. i^'w^:na^^rnJ?imt^nTrrea,iniri«r.!«aBirh3W3»»nswi|!w-i»iaTsniS3f3«»* MUDD library 19 8 3 Medical Digitized by the Internet Archive in 2017 with funding from The National Endowment for the Humanities and the Arcadia Fund https://archive.org/details/histologicalhistOOtill A HISTOLOGICAL AND. HISTOCHEMICAL STUDY CF TRANSPLANTED PITUITARY GLANDS IN MICE Thomas W. Tillack, A*R. The University of Rochester, 1959 A Thesis Presented to the Faculty of the Yale University School of Medicine In Partial Fulfillment of the Requirements for the Degree of Doctor of Medicine The Department of Anatomy Yald University School of Medicine April 1963 ,i. oi.-;. Mamr. i-iu JAoiEO,xoxax-; » ■ - £ ft. • ACKNOWLEDGEMENTS I wish to sincerely thank Dr. W. U. Gardner for his thoughtful advice and assistance in every phase of this project. -

Bacterial Diversity at an Abandoned Coal Mine in Southeast Kansas
Pittsburg State University Pittsburg State University Digital Commons Electronic Thesis Collection Spring 5-12-2017 Bacterial Diversity at an Abandoned Coal Mine in Southeast Kansas Rachel Bechtold Pittsburg State University, [email protected] Follow this and additional works at: https://digitalcommons.pittstate.edu/etd Part of the Integrative Biology Commons, and the Other Ecology and Evolutionary Biology Commons Recommended Citation Bechtold, Rachel, "Bacterial Diversity at an Abandoned Coal Mine in Southeast Kansas" (2017). Electronic Thesis Collection. 335. https://digitalcommons.pittstate.edu/etd/335 This Thesis is brought to you for free and open access by Pittsburg State University Digital Commons. It has been accepted for inclusion in Electronic Thesis Collection by an authorized administrator of Pittsburg State University Digital Commons. For more information, please contact [email protected]. BACTERIAL DIVERSITY AT AN ABANDONED COAL MINE IN SOUTHEAST KANSAS A Thesis Submitted to the Graduate School in Partial Fulfillment of the Requirements for the Degree of Master of Science Rachel Bechtold Pittsburg State University Pittsburg, Kansas May 2017 BACTERIAL DIVERSITY AT AN ABANDONED COAL MINE IN SOUTHEAST KANSAS Rachel Bechtold APPROVED: Thesis Advisor ________________________________________________ Dr. Anuradha Ghosh, Biology Committee Member ________________________________________________ Dr. Dixie Smith, Biology Committee Member _________________________________________________ Dr. Ram Gupta, Chemistry ACKNOWLEDGEMENTS I would like to thank my professors and mentors at Pittsburg State University. Dr. Ghosh for her astute edits, positive attitude, and devotion to research. Dr. Smith for instilling in me a passion for soils. Dr. Gupta for his knowledge in subject of chemistry and amiable help. Dr. Chung and Kim Grissom have been a great help from the beginning in both laboratory prep and in learning new lab techniques. -

Preliminary Notice Upon the Cytology of the Brains of Some Amphibians
Preliminary Notice upon the Cytology of the Brains of Some Amphibians: 1. necturus. / V With Two Plates. BY Smith Ely Jelliffe, M.D. Reprinted from The Journal of Comparative Neurology, VoI. VIT, No. 2, Sept., 1897. PRELIMINARY NOTICE UPON THE CYTOLOGY OF THE BRAINS OF SOME AMPHIBIANS: I. NECTURUS. 1 By Smith Ely Jelliffe, M.D, With Plates XII and XIII. In view of the great impulse which has been given to cyto- logical work within recent years, the writer has felt that a study of the cells of the brains of some of the lower animal forms might give a clue to the correct interpretation of results ob- tained with human material both normal and diseased. The study of the nerve cells by means of the methylene blue stain (Nissl) has suggested a number of problems with far- reaching results. The past few years have seen a large acces- sion of workers using this method and the question, as the writer sees it, resolves itself into one of interpretation. It is true that the physico-chemical changes taking place in nerve cells are accompanied by constant changes in molar composi- tion as Nissl claims? Can these changes be registered and studied by technical microscopical methods as outlined by Hodge, Vas, Mann and numerous others; and finally is the Nissl method or its modifications such a method, and can its pictures be relied upon to give accurate and trustworthy re- sults ? Such a broad outline is, however, manifestly beyond the purpose of the present paper which will simply state some points of possible interest obtained thus far in a research which the writer will hardly be able to complete for the present.