Challenges in Implementation of the ANISA Protocol at the Odisha Site in India
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Adoption Behavior of Farmers in Khordha District of Odisha, India
Asian Journal of Agricultural Extension, Economics & Sociology 38(12): 102-106, 2020; Article no.AJAEES.63222 ISSN: 2320-7027 Adoption Behavior of Farmers in Khordha District of Odisha, India Mita Meher1*, Sushree Purabi Panigrahi1 and Debasmita Nayak2 1Department of Extension Education, School of Agriculture, GIETU, India. 2Department of Extension Education, OUAT, Bhubaneswar, India. Authors’ contributions This work was carried out in collaboration among all authors. Author MM designed the study, performed the statistical analysis, wrote the protocol and wrote the first draft of the manuscript. Authors SPP and DN managed the analyses of the study. Author DN managed the literature searches. All authors read and approved the final manuscript. Article Information DOI: 10.9734/AJAEES/2020/v38i1230493 Editor(s): (1) Dr. Tulus T. H. Tambunan, University of Trisakti, Indonesia. (2) Dr. Ian McFarlane, University of Reading, UK. (3) Dr. Roxana Plesa, University of Petrosani, Romania. Reviewers: (1) Burhanuddin Daeng Pasiga, Hasanuddin University, Indonesia. (2) Dedehouanou Houinsou, University of Abomey-Calavi, Rep. of Benin. Complete Peer review History: http://www.sdiarticle4.com/review-history/63222 Received 25 October 2020 Accepted 30 December 2020 Original Research Article Published 31 December 2020 ABSTRACT It is a generic concept that farmers like other kind of entrepreneurs; do not adopt innovation simultaneously as they crop up on the market. Diffusion typically takes a number of years, scarcely reaches a level of 100% of the potential adopters’ population and mostly follows S-shaped curve in time. Apparently, some farmers choose to be the first users while others prefer to be early adopters or late adopters, some prefers not to adopt. -

Ethnomedicines in the Khordha Forest Division of Khordha District, Odisha, India
Int.J.Curr.Microbiol.App.Sci (2014) 3(1): 274-280 ISSN: 2319-7706 Volume 3 Number 1 (2014) pp. 274-280 http://www.ijcmas.com Original Research Article Ethnomedicines in the Khordha forest division of Khordha District, Odisha, India Mukesh Kumar1*, Tariq Ahmad Butt2, S.A.Hussaini1, Kishore Kumar1, Hakimuddin Khan1, Aminuddin3, and L.Samiulla1 1Regional Research Institute of Unani Medicine, Bhadrak-756 100, Odisha, India 2Regional Research Institute of Unani Medicine, Srinagar, J. andK., India 3Central Council for Research in Unani Medicine, New Delhi-110 058, India *Corresponding author A B S T R A C T Based on an ethnopharmacological survey of Khordha Forest Division of Khordha K e y w o r d s district in Odisha conducted during 2012, the paper presents some 54 contemporary folk recipes comprising 43 taxa of folk medicinal plants used by Kondh, Sabra, Naik tribes of the area, for treatment of various common and chronic diseases and Ethnobotanical conditions. Botanical name, family in bracket, locality with field book number, survey; local name, Unani name, part(s) used, name of the disease against which used, traditional mode of administration and informant is given for each recipe discussed in the text. medicine; The need for their phytochemical and pharmacological investigations in the context Khordha; of claims reported has been suggested in an effort to discover new drugs of natural Odisha. origin for many of the diseases for which modern medicine has, thus far, no satisfactory cure. Introduction Ethnomedicines have gained new uses of plants for treatment of various disease and conditions was recorded. -

Orissa Flood 2003
ORISSA FLOOD SITREP 7th September 2003, 2300 hrs ORISSA FLOOD 2003 SITUATION REPORT - NATURE OF DISASTER - MEASURES TAKEN - CURRENT NEEDS - WEATHER FORECAST - COORDINATION - DAMAGE DETAIL REPORT - COMMUNITY AND GOVERNMENT - PROJECTED THREATS PREPAREDNESS - DISTRICT-WISE DAMAGE DETAILS - IMPORTANT INFORMATION - HEALTH INTERVENTION - SOURCE OF INFORMATION 1 ORISSA FLOOD SITREP 7th September 2003, 2300 hrs NATURE OF DISASTER: FLOODS Return to Main The state of Orissa is reeling under severe floods since the 27th of August 2003. Continuous rains in the upper and lower catchment areas of the Mahanadi river system adjoining the state of Chhattisgarh have worsened the current situation. 19 out of 30 districts have been affected so far, namely Angul, Bargarh, Boudh, Bolangir, Cuttack, Ganjam, Jagatsinghpur, Jajpur, Jharsuguda, Kalahandi, Kendrapada, Khordha, Nayagarh, Puri, Sambalpur, Deogarh, Sonepur, Koraput, and Nuapada. National, State, military, and paramilitary forces have been mobilized to assist in the severely affected districts. Road and communication infrastructure have also been badly hit in some parts of the state. Sundergarh has experienced flash floods on the 5th of September affecting Gurundia and Bonai blocks. No damage has been reported so far. The water level of Hirakud reservoir as on 7th September, 2003 at 1800 hrs was 628.65 feet. The inflow to the reservoir is 5, 78,000 and the outflow is 5, 78,000. Naraj Barrage is releasing 9.6 lakhs cusecs of water resulting in the rise of water level in River Kathjodi but no serious threats are being assesses now and the situation is being closely monitored. WEATHER FORECAST: Yesterday's low pressure area over northwest & adjoining west-central Bay of Bengal now lies over Northwest Bay of Bengal & with associated upper air cyclonic circulation extending up to mid-tropospheric level. -

Activity Report for the Year 2013-14
THE ROLE OF REVENUE & DISASTER MANAGEMENT DEPARTMENT Revenue administration is closely associated with the all round development of the State and the prosperity of its people. Land is an important source of livelihood of people and their shelter. Revenue administration touches individuals and is concerned with their problems. The activities of the Revenue Department are not merely confined to solving people’s problems relating to land; these also include providing land to the landless and protecting the Government land. This Department shoulders the responsibility of providing immediate relief to the people affected by natural calamities such as floods, droughts, cyclones, hailstorms, earthquakes, fire accidents, etc. It also takes initiatives for rehabilitation and restoration work. In the matter of transfer of property, particularly the transfer of immovable property, the Registration Offices play a key role in serving people and contributing to the resources of the State by collecting Registration Fee and Stamp Duty. Distribution of Government wasteland for agriculture/ homestead purposes, distribution of ceiling surplus land, prohibition of tribal land alienation, computerisation of Registration and Tehsil Offices, updating of land records and conversion/ regularisation of pre-1980 forest villages and encroached human habitations in forest areas, preparation and distribution of Land Pass Books and formulation of comprehensive rehabilitation and resettlement policy for displaced persons are a few noteworthy programmes of this Department. Appropriate steps are being taken to make Revenue Administration more effective and responsive to the public. The important activities and achievements of this Department during the year 2013-2014 are indicated below: 1. National Land Records Modernization Programme (NLRMP) The National Land Records Modernization Programme (NLRMP), a Centrally Sponsored Scheme which aims at developing a modern, comprehensive and transparent land records management system is being implemented in the State since 2009-10. -
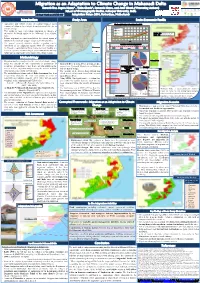
Migration As an Adaptation to Climate Change in Mahanadi Delta
Migration as an Adaptation to Climate Change in Mahanadi Delta Shouvik Das, Sugata Hazra* , Tuhin Ghosh*, Somnath Hazra, and Amit Ghosh (*Presenting Authors) School of Oceanographic Studies, Jadavpur University, India Abstract Number: ABSSUB-989 Adaptation Future 2016, Rotterdam, Netherlands Introduction Study Area Socio-Economic Profile • Agriculture and fishery sectors of natural resource based The Decadal Variation in Population Since 1901 Map of India economy of deltas are increasingly becoming unprofitable due to 2,500,000 Climate Change. Bhadrak 2,000,000 Kendrapara • This results in large scale labour migration, in absence of Jagatsinghapur 1,500,000 alternative livelihood option in the Mahanadi delta, Odisha, Mahanadi Delta Khordha Odisha: 270 persons per sq. km. 1,000,000 Puri India: 382 persons per sq. km. India. Population Total • Labour migration increased manifold in the coastal region of 500,000 Odisha in the aftermath of super cyclones of 1999 and 2013. - 1901 1911 1921 1931 1941 1951 Year 1961 1971 1981 1991 2001 2011 • The present research discusses whether migration can be 30 Population Growth Rate (%), 2001-2011 considered as an adaptation option when the mainstay of 20 Odisha: 14.05% livelihood, i.e. agriculture is threatened by repeated flooding, sea 10 0 level rise, cyclone and storm surges, salinization of soil and crop (%) Rate Growth Bhadrak Kendrapara Jagatsinghapur Khordha Puri 1% failure due to temperature stress imposed by climate change. 5% Malkangiri 205 9% Koraput 170 26% 157 5% Methodology Rayagada 146 -
Cuttack District, Odisha for River Sand
DISTRICT SURVEY REPORT (DSR) OF CUTTACK DISTRICT, ODISHA FOR RIVER SAND (FOR PLANNING & EXPLOITING OF MINOR MINERAL RESOURCES) ODISHA CUTTACK As per Notification No. S.O. 3611(E) New Delhi, 25th July, 2018 MINISTRY OF ENVIRONMENT, FOREST AND CLIMATE CHANGE (MoEF & CC) COLLECTORATE, CUTTACK CONTENT SL NO DESCRIPTION PAGE NO 1 INTRODUCTION 2 OVERVIEW OF MINING ACTIVITIES IN THE DISTRICT 3 LIST OF LEASES WITH LOCATION, AREA AND PERIOD OF VALIDITY 4 DETAILS OF ROYALTY COLLECTED 5 DETAILS OF PRODUCTION OF SAND 6 PROCESS OF DEPOSIT OF SEDIMENTS IN THE RIVERS 7 GENERAL PROFILE 8 LAND UTILISATION PATTERN 9 PHYSIOGRAPHY 10 RAINFALL 11 GEOLOGY AND MINERAL WALTH LIST OF PLATES DESCRIPTION PLATE NO INDEX MAP OF THE DISTRICT 1 MAP SHOWING TAHASILS 2 ROAD MAP OF THE DISTRICT 3 MINERAL MAP OF THE DISTRICT 4 LEASE/POTENTIAL AREA MAP OF THE DISTRICT 5 1 | Page PLATE NO- 1 INDEX MAP ODISHA PLATE NO- 2 MAP SHOWING THE TAHASILS OF CUTTACK DISTRICT ......'-.._-.j l CUTTACK ,/ "---. ....•..... TEHSILMAP '~. Jajapur Angul Dhe:nkanal 1"' ~ . ..••.•..•....._-- .•.. "",-, Khordha ayagarh Tehs i I Bou ndmy -- Ceestnne PLATE NO- 3 MAP SHOWING THE MAJOR ROADS OF CUTTACK DISTRICT CUTTACK DISTRICT JAJPUR ANGUL LEGEND Natiol1Bl Highway NAYAGARH = Major Road - - - Rlliway .••••••. [JislJicl Bmndml' . '-- - - _. state Boullllary .-". River ..- Map ...l.~~.,. ~'-'-,.-\ @ [Ji8tricl HQ • 0Che-10Vil'I COjJyri!ll1tC 2013 www.mapsolindiiO:b<>.h (Updaled an 241h .Jenuary 201:l'l. • MajorlOVil'l PREFACE In compliance to the notification issued by the Ministry of Environment and Forest and Climate Change Notification no. S.O.3611 (E) NEW DELHI dated 25-07-2018 the preparation of district survey report of road metal/building stone mining has been prepared in accordance with Clause II of Appendix X of the notification. -

Khordha District
Orissa Review (Census Special) KHORDHA DISTRICT the east and Ganjam district in the south. Khordha Khordha is the headquarters of the district of the district has a geographical area of 2813 sq. kms. same name and is situated on the National The hilly systems of the district are located in Highway No.5. The town is 11 kms. away from Khordha sub-division. Khordha district is situated Khordha Road Railway Station. The Local name in the southwest of the state. Also it touches the of the place was “Jajarsingh” which originally was ‘Chilika Lake’ in the south. a small village probably the place was known as The district of Khordha is constituted “KURADA” which means “Foul mouthed”. by 7 towns including 2 census towns and 1551 Khordha came into prominence with the first king villages spread over 10 C.D blocks. It has 18 of “Bhoi” dynasty Ramachandra Dev, who made lakhs population of which males constitute 52.57 it the capital of his kingdom during the last part of percent and females 47.43 percent. The 16th century A.D. The Bhoi kings lived in the fort population growth rate during the last decade of of Barunei hill. The fort is now completely ruined the twentieth century is 24.79 annually. The area and a few traces are there to remember the former of the district is 2813 sq.km and thus, population glory. Khordha suffered repeatedly from Muslim density works out to be 667. Sex ratio(females and Maratha cavalry but its royal house retained per 1000 males) works out to be 902 considering much of its independence till 1804 when the then the total population of each sex and that for Raja Mukunda Deva under the guidance of population of 0-6 years it is 925 indicating relative Rajguru Jayakrishna fought against the British deficit of females at younger ages. -

Status of Elementary and Secondary Education in Odisha 2016-17
STATUS OF ELEMENTARY AND SECONDARY EDUCATION IN ODISHA 2016-17 SOURCE: Unified DISE 2016-17 (as on 30th September, 2016) ODISHA PRIMARY EDUCATION PROGRAMME AUTHORITY SHIKSHA SOUDHA, UNIT-V, BHUBANESWAR – 751001 Website: www.opepa.in Published by the Management Information System (MIS), OPEPA on behalf of Department of School & Mass Education, Government of Odisha Published by the Management Information System (MIS), OPEPA on behalf of Department of School and Mass Education, Government of Odisha. Project Team This publication is the outcome of the collaborative activities of the Department of School and Mass Education, Odisha Primary Education Programme Authority (OPEPA), State & District MIS Unit, SSA and entirely based on the DISE & CTS / HHS data as received from the 30 District Project Offices. The key officials of SSA involved in the collection and implementation of the DISE & CTS / HHS activities are as enlisted below: Location Name Designation Email Contact No. SPO Shri Pravat Kumar Mishra Asst. Director (MIS) [email protected] 9437126232 SPO Smt. Smita Mohanty Programmer [email protected] 9861391904 SPO Smt. Juthika Acharay Programmer [email protected] 9438826177 SPO Smt Namita Panda Programmer [email protected] 9437944067 SPO Shri Swaroop Ranjan Mohapatra System Administrator [email protected] 9437178244 SPO Shri Ashirbad Sahu Network Administrator [email protected] 9437406788 OMSM Shri Pravakar Pratihari Programmer [email protected] 9861333425 Angul Smt. P.Pujapanda Programmer [email protected] 9437281780 Balasore Shri Saroj Kumar Mohapatra Programmer (IC) [email protected] 9437944067 Bargarh Shri Pradeep Kumar Sahu Programmer [email protected] 9437201384 Bhadrak Shri Manoj Kumar Nayak Programmer [email protected] 9439444854 Bolangir Shri Debesh Mishra Programmer [email protected] 9437329961 Boudh Shri Saroj Behera Programmer [email protected] 9439885379 Cuttack Smt. -

Newsletter for Investment Promotion and Facilitation May 2018 | Volume 2, Issue 2
Invest Odisha e-Newsletter for Investment Promotion and Facilitation May 2018 | Volume 2, Issue 2 What’s Inside District in Focus- Khordha Khordha is an industrialized district of Ø District in Focus: Odisha and houses the capital city, Khordha Bhubaneswar. Blessed with the unique Ø Road to MIO Conclave advantages of quality industrial & social 2018 infrastructure and multi-modal connectivity, Khordha has today become one of the most Ø Did You Know? preferred investment destinations in East Ø Odisha in News India. To support cluster based industrial Ø GO SWIFT – FAQs & development, various industrial clusters have been developed in Khordha district as Testimonial Khordha summarized below: A. Sea Food Park, Deras: The sea food park at Deras is a 152 acres sea food processing cluster with dedicated common facilities for pre processing, cold storage, central processing centre and packaging units. It houses some of the major sea food producers such as Falcon Marine, Magnum Sea Foods etc. B. Khordha Food Park: The mega food park project in the district is home to some of the biggest players in the food processing industry such as ITC, Coca Cola, Parle, Indo Nissin etc. Several other companies are setting up manufacturing facilities in the Khordha Food Park. C. Infocity: The Infocity in the district is home to major IT companies such as Infosys, TCS, Wipro, Mindtree, Tech Mahindra etc. D. Chattabar: Situated in close vicinity of capital city, Bhubaneswar, Chattabar is being developed for apparel and food processing Domestic Air Connectivity of Khordha District (Bhubaneswar) industries. Spread across an area of 100 acres, with various cities the cluster has generated significant interest Manpasand Beverages is setting up a pulp-based beverage amongst the investor community. -

Patterns and Potential of Urbanisation of Khordha District, Odisha, India
The Indian Journal of Spatial Science Vol - 7.0 No. 2 Winter Issue 2016 pp. 38 - 42 The Indian Journal of Spatial Science EISSN: 2249 - 4316 homepage: www.indiansss.org ISSN: 2249 - 3921 Patterns and Potential of Urbanisation of Khordha district, Odisha, India Debika Banerji Research Scholar, Research Scholar,Department of Geography, Visva-Bharati, Santiniketan,West Bengal Article Info Abstract ______________________ _________________________________________________________ Article History In a developing nation like India, the characteristics of the urbanisation are pronounced in Received on: migration patterns. By analysing the ever growing demand of the population in terms of its number 14 June 2016 and nature it is seen an ever increase in urban growth is concentrated in the cities. Thus a primate Accepted inRevised Form on: city develops, which leads to too much concentration and overcrowding in a small place. An 15 August 2016 overview of the Khordha District in Odisha gives us the results. AvailableOnline on and from: 23 September 2016 ________________ __ __ _ ___ Key Words Urbanisation Census Towns © 2016 ISSS. All Rights Reserved Primate city ___________________ _______________________________________________________________ Introduction Literature Review Urbanisation is an index of transformation from Urbanisation and the progressive associated changes traditional rural economies to modern industrial one. It is that are seen in a region lead to a change in the a progressive concentration (Davis, 1965;Datta, 2006) population characteristics of that region (Davis, 1965; of population in any urban unit. Kingsley Davis has Datta, 2006). The most important reportshave been the mentioned has mentioned a stage wise change from the Census of India, 2011, Provisional Population Totals for traditional rural agrarian economies to the industrial the Indian definitions of Towns and Cities. -

Download(210.23
Abstract of replies of the Departments regarding implementation of the approved Cabinet Memoranda till date for the Calendar Year 2017 Replies sent by the Departments regarding implementation of the decisions Sl. Name of the No. of Not implemented / No No. Department/s Memoranda Implemented reasons at detailed reply reply (Subject-wise) yet 1. Agriculture & Farmers’ 3 2 Empowerment 2. Commerce & Transport (Commerce) 3. Commerce & Transport 1 1 (Transport) 4. Cooperation 1 1 5. Electronics & 1 Information Technology 6. Energy 3 3 7. Excise 8. Finance 17 16 9. Fisheries & Animal 1 1 Resources Development 10. Food Supplies & 1 1 Consumer Welfare 11. Forest & Environment 4 3 12. General Administration 6 6 & Public Grievances 13. Handlooms, Textiles & 2 2 Handicrafts 14. Health & Family Welfare 2 2 15. Higher Education 3 3 16. Home 2 2 17. Housing & Urban 9 8 Development 18. Industries 19. Information & Public Relations 20. Labour & E.S.I. 21. Law 2 2 22. Micro, Small & Medium 3 3 Enterprises 23. Panchayati Raj & 1 1 Drinking Water 24. Parliamentary Affairs 1 1 25. Planning & 1 1 Convergence 26. Revenue & Disaster 9 8 Management 27. Rural Development 1 1 28. S.T. & S.C. Development 29. School & Mass 1 1 Replies sent by the Departments regarding implementation of the decisions Sl. Name of the No. of Not implemented / No No. Department/s Memoranda Implemented reasons at detailed reply reply (Subject-wise) yet Education 30. Science & Technology 1 1 31. Skill Development & 1 1 Technical Education 32. Social Security and Empowerment of Persons with Disability 33. Sports & Youth 1 1 Services 34. -

Brief Industrial Profile of Khordha District 2019-20
Government of India Ministry of MSME Brief Industrial Profile of Khordha District 2019-20 Carried out by MSME - Development Institute (Ministry of MSME, Govt. of India,) As per the Guidelines issued by O/o DC(MSME),New Delhi Phone:0671-2950011 Fax: 0671-2950011 E. Mail: [email protected] Website: www.msmedicuttack.gov.in i F O R E W O R D Every year Micro, Small & Medium Enterprises Development Institute, Cuttack under the Ministry of Micro, Small & Medium Enterprises, Government of India has been undertaking the Industrial Potentiality Survey for the districts in the state of Odisha and brings out the Survey Report as per the guidelines issued by the office of Development Commissioner (MSME), Ministry of MSME, Government of India, New Delhi. Under its Annual Action Plan 2019-20, all the districts of Odisha have been taken up for the survey. This Industrial Potentiality Survey Report of Khordha district covers various parameters like socio- economic indicators, present industrial structure of the district and availability of industrial clusters, problems and prospects in the district for industrial development with special emphasis on scope for setting up of potential MSMEs. The report provides useful information and a detailed idea of the industrial potentialities of the district. I hope this Industrial Potentiality Survey Report would be an effective tool to the existing and prospective entrepreneurs, financial institutions and promotional agencies while planning for development of MSME sector in the district. I would like to place on record my appreciation for Sri B. K. Moharana, Asst. Director (EI) of this Institute for his concerted efforts to prepare this report for the benefit of entrepreneurs and professionals in the state.