Larimer County | Health & Environment
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Café Car Menu
Café Car Menu BREAKFAST SNACKSM BEVERAGES Combo: Blueberry Muffin and Coffee M ..... $3.75 Cheese and Cracker Tray ..........................$5.50 Starbucks® Iced Coffee .............................$3.50 Jimmy Dean® Sausage Egg Muffin ........... $4.50 Fresh Fruit Cup ......................................... $4.50 Monster® Energy Drink ..............................$3.50 Three Meat and Cheese Breakfast Burrito ... $3.50 Almonds / Pistachios ................................$4.00 Pure Leaf® Iced Tea .................................. $3.00 ® Cold Cereal / Quaker® Oatmeal(with milk)M ... $2.50 Guacamole / Hummus Snack Kit .............. $3.00 San Pellegrino Sparkling Water ...............$2.75 Bagel and Cream Cheese M ....................... $2.50 Chips (assorted) ............................................................................. $2.00 Soft Drinks .................................................$2.25 Blueberry Muffin M ..................................... $2.75 Bottled Spring Water/Flavored Water ....... $2.25 Cinnamon Roll M ........................................ $2.75 Apple/Orange/Cranberry Juice .................$2.50 Chobani® Greek YogurtM ........................... $2.50$ Coffee, Hot Tea or Hot Chocolate .............$2.00 Milk ............................................................ $1.50 Cup of Hot Water ...................................... $0.25 SUNDRIES BikeLink Card ..........................................$20.00 Ear Buds ....................................................$5.00 Bungee Cord 24” .......................................$3.00 -

Download Nutritional Guide
Taco Villa Nutritional Guide The nutritional information that is represented here is composed of data that was provided by Taco Villa LTD., Analytical Food Laboratories, and ESHA Genesis R&D. The nutritional data was initially completed in May 2003. The nutritional data is figured based upon normal product formulation. There is a possibility of variations in the data because of geographical region, area suppliers, portioning and/or time of year. Serving Size (g) Size Serving Calories Calories Fat Fat (g) Total Carbohydrates (g) (mg) Cholesterol (mg) Sodium (g) Fiber (g) Protein Menu Items Crispy Taco - Taco Shell, Beef Taco Meat, Lettuce, Cheese, and Tomato 113 240 130 15 13 40 190 1 13 Steak Fajita Taco w/ 2 Corn Tortillas - 2 Corn Tortillas, Steak, Cheese, and Pico de Gallo 112 240 80 9 22 10 510 3 15 Steak Fajita Taco w/ Flour Tortilla - Flour Tortilla, Steak, Cheese, and Pico de Gallo 91 210 90 10 15 10 680 1 15 Steak Fajita Taco on Corn Tortillas w/ Guacamole - 2 Corn Tortillas, Steak, Cheese, Guacamole, and Pico de Gallo 140 290 120 14 24 10 590 4 16 Steak Fajita Taco on Flour Tortilla w/ Guacamole - Flour Tortilla, Steak, Cheese, Guacamole, and Pico de Gallo 119 260 130 14 17 10 760 2 16 Steak Fajita Taco Grande w/ 2 Corn Tortillas- 2 Corn Tortillas, Steak, Cheese, Pico de Gallo, Sour Cream, Lettuce, and Tomatoes 140 250 90 10 23 15 520 4 16 Steak Fajita Taco Grande 2/ Flour Tortilla - Flour Tortilla, Steak, Cheese, Pico de Gallo, Sour Cream, Lettuce, and Tomatoes 119 230 100 11 16 15 690 2 16 ** Nutrition for Combo Meals does not include drink. -

Report No Available from Abstract Document
DOCUMENT RESUME ED 433 127 PS 027 842 TITLE Food, Family and Fun: A Seasonal Guide to Healthy Eating. Commemorating 50 Years of School Lunch. INSTITUTION Food and Consumer Service (USDA), Washington, DC. REPORT NO FCS-298 PUB DATE 1996-06-00 NOTE 129p. AVAILABLE FROM Superintendent of Documents, Government Printing Office, Washington, DC 20402; Tel: 202-512-1800 (Stock No. 001-000-04627-6). PUB TYPE Guides Non-Classroom (055) EDRS PRICE MF01/PC06 Plus Postage. DESCRIPTORS *Children; *Cooking Instruction; Elementary Secondary Education; Learning Activities; Lunch Programs; *Nutrition; *Nutrition Instruction; Parent Materials; *Recipes (Food) IDENTIFIERS *Cook Books; Family Activities; School Lunch Program; *Seasons ABSTRACT Helping children make food choices for a healthy diet can be challenging. This book is designed as a resource guide and cookbook for parents to help them make healthful eating and cooking with children tasty, simple, affordable, and fun. The book is a collection of 50 recipes organized by season, and featuring family nutrition education activities. The book concludes with a resource section including community resources such as a list of local farmers' markets and state extension contacts for the United States Department of Agriculture's Team Nutrition; hotline numbers and Internet addresses; and healthful eatin; st,:igestions such as making food substitutions. (KB) ******************************************************************************** Reproductions supplied by EDRS are the best that can be made from the original -

Simplified Summary NPS for Chronic Tacos 1-21-16.Xlsx
Bases Quantity For: Calories Calories fromfat fat(g) Total Saturated fat(g) fat(g) Trans Cholesterol (mg) (mg) Sodium Carbohydrates (g) Dietary fiber (g) Sugars (g) (g) Protein Burritos and Quesadillas Tortilla - 13" Flour Regular 250 50 6 1.5 420 42 7 Tortilla - 10" Flour Small/Kids 110 20 2.5 0.5 180 18 1 3 Tacos Potato Taco (1 Each) 1 Taco 290 190 22 5 0 10 190 18 1 4 Tortillas - 6" Corn (1 Each) 1 Taco 60 0 0 30 11 1 Tortillas - 6" Corn (2 Each) 1 Taco 120 10 1 60 22 2 Tortillas - 6" Flour (1 Each) 1 Taco 70 15 1.5 120 12 2 Tortillas - Crispy Shell (1 Each) 1 Taco 130 80 9 1 120 12 2 Tostada Bowls Tostada Bowl Tostada Bowls 190 110 12 2 0 160 16 3 Tortas Telera Bread Tortas 300 20 2.5 580 58 5 9 Chronic Nachos/Fries Tortilla Chips Chronic Nachos 390 210 24 3 0 550 44 6 6 Fries Chronic Fries 850 530 59 12 0 85 71 7 3 7 Chronic Salads Half Lettuce, Half Cabbage Chronic Salad 35 0 0 40 7 3 3 2 Shredded Cabbage Chronic Salad 45 0 0 0 30 10 4 5 2 Shredded Lettuce Chronic Salad 25 0 0 50 5 2 1 2 Flautas Flautas - Beef 3 Flautas 1080 740 84 17 1 75 1070 55 2 2 29 Flautas - Chicken 3 Flautas 1070 710 81 15 1 75 1090 55 2 2 32 Taquitos Taquitos - Beef 3 Taquitos 870 550 63 12 1 115 1270 35 2 40 Taquitos - Chicken 3 Taquitos 840 490 56 9 0 115 1450 35 2 45 Breakfast Chorizo Breakfast Bowl Breakfast Bowls 640 410 46 11 0 845 1290 25 3 3 33 Gringo Breakfast Bowl Breakfast Bowls 640 420 47 12 0 650 930 21 2 2 33 Machaca Breakfast Bowl Breakfast Bowls 410 250 28 8 0 690 810 4 3 38 Veggie Breakfast Bowl Breakfast Bowls 490 330 37 3 0 635 450 21 -

Antojitos (Appetizers)
EAT IN TAKE OUT OPEN 7 DAYS A WEEK FROM 11AM HAPPY HOUR MON-FRI 4–6PM IN A HURRY? CALL AHEAD AND PLACE YOUR TO GO ORDER AND WE’LL HAVE IT READY AND WAITING WHEN YOU ARRIVE. DINING IN? 207·883·TACO FEEL FREE TO CALL ONE HOUR AHEAD TO GET YOUR www.elrayotaqueria.com NAME ON OUR WAITING LIST. ANTOJITOS (APPETIZERS) GOLDEN LOADED TOT NACHOS – 8.95 CORN CHIPS – 1.50 JET PINEAPPLE – 3.95 fried tater tots topped with crema, w/ salsa – 3.95 on a stick dusted with chile powder, melted monterey jack cheese, w/ guacamole – 5.95 salt & lime pickled jalapeños, pico de gallo w/ salsa & guacamole – 8.95 & scallions FUNDIDO – 8.95 CHEESE NACHOS – 5.95 warm cheese dip with cilantro, rajas & FRIED BRUSSEL w/ organic black beans – 6.95 your choice of mushrooms or SPROUTS – 8.95 w/ choice of chorizo, shredded pork, housemade chorizo tossed in a chili-lime vinaigrette grilled chicken, steak OR Served with corn chips with toasted sesame seeds, ground beef – 9.95 red onion escabeche & jalapeños MEXICO CITY STYLE CORN Make your nachos GRANDE ON THE COB – 4.95 YUCCA FRIES – 7.95 by adding guacamole, shredded basted with chipotle mayo & golden fried yucca fries served with a lettuce, housemade crema, radishes, dusted with cotija cheese chimichurri aioli† and citrus habanero pickled jalapeños, cilantro & bbq dipping sauces taquerera salsa add 5.95 FRIED PLANTAINS – 6.95 with chipotle mayo CHICKEN TAQUITOS – 8.95 three corn tortillas filled with rajas, PAPAS FRITAS – 4.95 jack cheese & chicken, rolled and fried. -

Great Sandwich Ideas
SPREADING GREAT SANDWICH IDEAS WITH LURPAK® With the Food-To-Go Sandwich market worth an estimated £5bn and annual spend up 1.7%, this suggests a continued growth. More people are buying sandwiches (footfall +7.2%) and there appears to be a willingness to pay more for good quality sandwiches (price per pack +3.2%).* Bread sales are in decline as busy people increasingly buy their lunchtime sandwich at work or in the high street. Sandwiches are the UK’s leading lunchtime meal, so it’s really not surprising your customers are seeking out new and exciting flavours, textures and ingredients. As the nation’s favourite butter brand, LURPAK® has commissioned exclusive research to DISCOVER BRITAIN’S NEXT TOP SANDWICH. We want to help you understand what’s next for our lunchtime favourite, so you can stay on-trend with a mouth-watering sandwich menu. *Source: Kantar Panel (52 w/e July 17, 2016) SUPERFOOD MULTIGRAIN FOCACCIA FLATBREAD RYE SOURDOUGH SPELT LOAF AHEAD Super bread with added superfoods. Italian cuisine is having a resurgence. Flatbreads have appeal as sandwich The traditional loaf may not be as Popular due to its sturdy nature and Enriching breads with chia seeds, This means a comeback for breads wraps, particularly when freshly popular but the rise in alternative ability to produce hearty sandwiches, WITH THE vitamin D, quinoa and pumpkin such as Focaccia. Ingredients baked baked and warmed. This includes breads is growing. along with the fact that the grain is seeds is perfect for health conscious in the bread, like sundried tomatoes Indian naan, Iranian sangak and non-GM and wholemeal. -

Manzano Mesa March 2020 Multigenerational Center $20 Yearly Membership Fee
Department of Senior Affairs Volume 18, Issue 3 Manzano Mesa March 2020 Multigenerational Center $20 Yearly Membership Fee Manzano Mesa Phone: 505.275.8731 Multigenerational Center Monday - Friday 8 a.m. - 9 p.m. 501 Elizabeth SE 87123 Saturday: 9 a.m.– 3 p.m. St. Patrick Day Tuesday, March 17th 11:30-1:00 p.m. Join us for a tradition Irish dish of corn beef and cabbage! Don’t forget to rock your green to win a door prize Reservations Required We are now on Social Media Inside this Issue: General Info ..……..……….…..Page 2 Classes …………………...……....Page 3 Menus ………………….……..…..Page 4 Happenings..…………….……..Page 5 Youth Program.……………... Page 5 Announcements ……………..Page 6 @cabqseniors Department of Senior Affairs Volume 18, Issue 3 READ to Me ABQ Department of Senior Affairs Collects new or gently used children’s books for distribution to children in our community. The goal Mayor Tim Keller of the program is to provide children with a personal book. Book drive through March 21, 2020. Anna Sanchez Director Open Computer Lab Nikki Peone Monday– Friday (No Wednesday) Division Manager 9 a.m. -11:30 a.m Wednesday 1:00 p.m. -2:45 p.m Please check in at front desk No Mondays during tax season Natasha Montoya Center Manager Bingo Vacant Thursday, 1:30 p.m. – 4 p.m. Center Supervisor Matt McCoy $3.00 for basic/special play, Youth Program Coordinator other games $0.25+ Courtney Morgan Office Assistant Mary Jo Church Program Assistant Vacant Friendship Coffee Program Assistant Tuesday 9:00 a.m. – 10:00 a.m. -

Breakfast All Nachos Are Served with Beans, Cheese, Pico De Gallo Sour Cream and Guacamole
Appetizers Nachos Breakfast All nachos are served with beans, cheese, pico de gallo Sour cream and guacamole. 1. Huevos Rancheros………………$7.50 Beans& cheese…………….…………………...………...$7.50 Two eggs ranch style, served on a fried tortilla with ranchero Chicken, ground beef, carnitas or al pastor….....$8.99 sauce. Served with rice, beans and your choice of corn or flour Carne asada, shredded beef or lengua…………....$9.75 tortillas. Fish or shrimp………………………..…………………….$10.75 2. Huevos ala Mexicana……...…….…$7.50 Quesadillas Two eggs scrambled with sautéed onions, tomatoes and jalepeno Served with guacamole and sour cream peppers (optional). Served with rice, beans and your choice of Chesse………………………………...……………………..$5.99 Authentic Mexican food II Chicken, ground beef, carnitas or al pastor……..$7.99 corn or flour tortillas Carne asada, shredded beef or lengua………...…$8.25 3. Chilaquiles…….…………………….$7.99 Fish or shrimp……………………………………...………$8.50 Corn tortillas fried with chili sauce and scrambled with two eggs. 333 dairy road Sincronizada with ham & avocado.$6.99 Served with rice and beans kahului, Maui, Hawaii 96732 Ham, mozzarella cheese, avocado & sour cream Add carne asada or chincken……………...…………………..$3.50 Taquitos Located behind 76 gas station Four taquitos served with lettuce, cheese, pico de gallo 4. Breakfast Burrito…………………$4.99 Sour cream and guacamole Scrambled eggs, cheese and beans. Chicken….$7.99 Shredded beef……$8.99 With Chorizo or machaca……………….…..………$6.99 Take out Shrimp ceviche bowl Chopped shrimp, onions, tomatoes, cilantro, and cucumber 5. Amigo’s Burrito…………………....$5.99 PH: (808) 872-9525 Cooked with lime juice, and served with avocado slices Scrambled eggs, potatoes, cheese and your choice of ham, bacon Fax: 872-9527 Small……….$6.99 Large………….$10.99 or sausage. -

Breakfast Burritos Nutrition Information Breakfast Plates Famous Burritos
Nutrition Information Sat Trans Fat Chol Sod Carbs Fiber Sugar Protein Menu Items Cal Fat Fat (g) (mg) (mg) (g) (g) (g) (g) (g) (g) Breakfast Burritos Chorizo Breakfast Burrito 990 55 20 1 395 2490 81 9 7 40 Machaca Burrito - Shredded Chicken 990 48 16 0 445 3360 88 13 9 49 Machaca Burrito - Shredded Beef 950 45 15 0 475 2390 78 10 9 58 Green Pig Burrito 880 41 16 0 470 2900 77 6 7 48 Sunrise Burrito 860 42 16 1 395 3090 77 6 7 40 Spud Burrito 660 26 11 0 395 2480 75 6 6 29 BRC con Huevos Burrito 1090 49 20 0 415 2030 120 13 6 40 Carne Asada Breakfast Burrito 980 41 15 1 425 3750 94 13 7 56 Add Cheese 110 9 5 0 30 190 1 0 0 6 Breakfast Plates Americano Plate - Bacon w/ Flour Tortilla 1070 54 20 0 425 2950 100 15 6 45 Americano Plate - Bacon w/ Corn Tortillas 910 48 16 0 425 2110 83 17 6 40 Americano Plate - Carne Asada w/ Corn Tortillas 970 43 15 0 470 2820 89 20 6 56 Americano Plate - Carne Asada w/ Flour Tortilla 1130 49 19 0 470 3650 106 18 6 61 Americano Plate - Chile Colorado w/ Corn Tortillas 880 42 14 0 430 1870 87 18 8 41 Americano Plate - Chile Colorado w/ Flour Tortillas 1040 48 18 0 430 2710 105 16 8 46 Americano Plate - Chile Verde Pork w/ Corn Tortillas 970 50 18 0 470 1950 85 17 7 47 Americano Plate - Chile Verde Pork w/ Flour Tortilla 1140 57 21 0 470 2790 102 15 7 52 Machaca Plate - Shredded Beef w/ Corn Tortillas 1210 55 18 0 490 2580 120 18 10 63 Machaca Plate - Shredded Beef w/ Flour Tortillas 1370 61 21 0 490 3420 137 16 10 68 Machaca Plate - Shredded Chicken w/ Corn Tortillas 1130 50 16 0 450 3480 120 18 11 51 Machaca -

Menu If You Would Like Slowly Braised and Simmered in Red Wine Shallot Gravy
Your Mimi’s favorites are back! We’ve brought back some of the classic dishes you’ve been asking for and added cravable new items to try. For breakfast, lunch or dinner, relax and enjoy a meal at our table. GRAND BREAKFAST MIMOSAS BEVERAGES Served with two eggs* (160 Cal) any style and your choice of Enjoy $5 Mimosas every pork sausage (530 Cal), turkey sausage (300 Cal), COFFEE DRINKS hickory-smoked bacon (370 Cal), or hickory-smoked ham Saturday and Sunday until 2:00PM! FRENCH ROAST COFFEE (910 Cal). Substitute your protein choice with slow-cooked $5 Mimosas do not include a champagne split. (0 Cal) corned beef hash. (420 Cal) Available where applicable by law. CAFÉ LATTE (150 Cal) (380 Cal) PAIN PERDU WITH MIXED BERRIES MOCHA LATTE MIMI-MOSA CAFÉ AU LAIT (80 Cal) Stuffed brioche french toast filled with orange marmalade A champagne split and orange juice with a ESPRESSO (0 Cal) tangerine burst. (220 Cal) and cream cheese blend topped with fresh berries and strawberry purée. (1150 Cal) CAPPUCCINO (130 Cal) ICED CAPPUCCINO MANGO MIMOSA (130 Cal) A champagne split and orange juice MALTED WAFFLES (380 Cal) with mango. (270 Cal) Buttermilk-malt waffles with whipped margarine ICED MOCHA and maple syrup. (420 Cal) Add mixed berries WHITE PEACH MIMOSA HOT TEA & HOT CHOCOLATE A champagne split and orange juice with the GREEN TEA (0 Cal) BRIOCHE FRENCH TOAST classic Bellini flavor of white peach. EARL GREY TEA (0 Cal) (270 Cal) French toast dusted with powdered sugar with whipped margarine and maple syrup. (590 Cal) CHAMOMILE TEA (0 Cal) HOT CHOCOLATE (180 Cal) TRIPLE BERRY MIMOSA A champagne split and orange juice with CINNAMON ROLL FRENCH TOAST strawberry, raspberry, blueberry and Cinnamon roll french toast with powdered sugar, cinnamon ICED TEA (720 Cal) blackberry. -

Download Menu
TACOS Sour Cream ½ pint --- $2.39 Guacamole ½ pint --- MARKET 3 Rolled tacos & cheese --- $3.49 PRICE Shredded beef rolled tacos, topped w/cheddar & jack cheese. Tamales per Dozen --- $16.00 3 Rolled tacos & guacamole -- $4.79 ½ Dozen Tamales --- $9.00 Shredded beef rolled tacos, topped w/guacamole, cheddar & jack cheese. EXTRAS Taco salad --- $4.99 MENU Tortilla shell w/bed of lettuce, beans, Cheese --- 89¢ pico de gallo, your choice of red chilli chicken or shredded beef, topped Guacamole --- 89¢ w/cheddar & sour cream. Sour Cream --- 89¢ BREAKFAST BURRITO $5.39 ea ENCHILADAS Tortilla --- 89¢ A- Bean, Cheese & Eggs. $4.99 Beef --- $5.99 Shredded beef wrapped w/ two corn DESSERTS B- Bacon, Cheese, Potatoes & Eggs. tortillas, topped w/enchiladas sauce, C- Chorizo, Potatoes, Cheese & Eggs. cheddar, jack cheese & lettuce. Churros --- $2.09 Plain, Cajeta, Cream. D- Ham, Potatoes, Cheese & Eggs. Chicken --- $5.99 E- Sausage, Potatoes, Cheese & Eggs. Red chilli chicken wrapped w/ two Churros --- $2.19 F- Mexican omelet ham, Cheese, Salsa & Eggs. corn tortillas, topped w/enchiladas Strawberry. sauce, cheddar, jack cheese & lettuce. G- Machaca, Cheese, Potatoes & Eggs. Xangos --- $4.69 H- Steak, Cheese, Potatoes, Salsa & Eggs. Cheese --- $5.99 Cheese cake chimichanga dessert. Plenty of cheese w/two corn tortillas, I- Potatoes, Cheese & Eggs. $4.99 topped w/enchiladas sauce, cheddar, jack cheese & lettuce. KIDS COMBOS Viva Burrito Colorado KIDS 1 6990 Leetsdale Dr. 7550 Pecos St. 6796 W. Colfax Ave. 5165 Federal Blvd. SIDE ORDERS Denver, CO. 80224 Denver, CO. 80221 Lakewood, CO. 80214 Denver, CO. 80221 One Quesadilla --- $3.99 (303) 320 4753 (303) 412 7391 (303) 274 0754 (303) 455 1384 Quesadillas --- $4.59 OPEN 24HRS Sun-Thu 6am-10pm Every day 6am-10pm Every day 6am-10pm Your choice of Carne Asada or Pollo Fri & Sat 6am-2pm Tortilla filled w/ Cheddar cheese. -
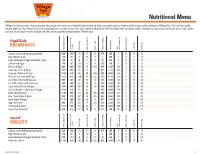
Nutritional Menu
VillageInn.com Nutritional Menu Village Inn Restaurants has provided this guide for menu nutritional information to help you make better informed decisions when dining at Village Inn. To use this guide, simply look for the menu item in the appropriate section to see the nutritional information. Please note that we often make changes to our menu to better serve you, so be sure to check back to the website for the most updated information. Thank you! brightside BREAKFASTS Total calories (cal) Total fat Calories from cal) (fat (g) Fat Total (g) Fat Saturated (g) Fat Trans (mg) Cholesterol (mg) Sodium Total (g) carbohydrate (g) Fiber Dietary (g) Sugars (g) Protein 2 Eggs, any style except poached 220 160 18 5 0 475 150 1 0 0 13 Egg Whites (4 oz) 120 60 7 1.5 0 0 190 1 0 1 12 Low-Cholesterol Egg Substitute (4 oz) 140 80 9 2 0 95 320 1 0 1 13 2 Poached Eggs 140 90 10 3 0 370 140 1 0 0 13 Bacon & Eggs 860 490 55 15 0.5 565 1840 59 2 9 31 Sausage Links & Eggs 1060 650 73 21 1 625 2220 60 2 10 41 Sausage Patties & Eggs 1240 820 92 30 0.5 655 2560 61 2 10 38 Biscuits & Gravy with Eggs 1580 970 109 41 0.5 600 4130 100 4 6 45 2-2-2 Breakfast with Bacon 600 340 38 11 0 555 1030 38 1 9 24 2-2-2 Breakfast with Sausage 700 420 47 14 0 585 1220 39 1 9 29 Corned Beef Hash & Eggs 1000 500 56 15 1.5 605 2650 76 5 11 43 1/2 lb Chicken-Fried Steak & Eggs 1480 810 91 23 1 630 3560 110 3 9 54 Ultimate Breakfast 1190 740 83 24 0.5 665 3310 62 2 12 52 6 oz.