Summary Report of the SEARO/IAPB Meeting on Elimination Of
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Fire and Other Health and Safety Incidents in the Bangladesh Garment Sector November 2012-March 2018
Fire and Other Health and Safety Incidents in the Bangladesh Garment Sector November 2012-March 2018 5,178 worker injuries and deaths (3,875 injuries; 1,303 deaths) Safety Factory Incident Incidents Name Location Date Injuries Deaths Cause/Outcome Description 1 Tazreen 252, 253 & 258, 11/24/12 200 112 The fire, presumably caused by a short circuit, started on the ground floor of the nine-story factory, trapping the Fashions Ltd. Monoshontuspur, workers on the floors above. Because of the large amount of fabric and yarn in the factory, the fire was able to Nishenantopur, quickly spread to other floors, complicating the firefighting operations. The fire burned for more than seventeen Ashulia hours before the firefighters were successful in extinguishing it. http://www.shahidulnews.com/bangladesh-textile- factory-fire-leaves-more-than-100-dead 2 Swan Dakkin 11/26/12 0 1 The fire originated from the warehouse of Swan Garments Ltd on the 1st floor of Afnan Plaza at Mollartek around Garments Ltd Khan,Uttara, 9:30am. It was doused around 12:00 noon after hectic efforts by 13 firefighting units. Dhaka Except for the second floor, the blaze could not spread through the building. Some workers sustained minor injuries as they rushed to the main staircase to get out of the building. Bundles of threads and clothes kept in the warehouse were also gutted. 3 Al-Shahriar Palashbari, 11/27/12 0 0 Fire might have originated from an electrical short circuit at the warehouse. Fabrics was burnt. No Injury Fabric Ltd. Ashulia 4 Section Seven Chittagong EPZ 11/28/12 50 0 Power generator of the factory caught fire due to a mechanical glitch. -

INTEGRATING LAND with WATER ROUTES: Proposal for a Sustainable Spatial Network for Keraniganj in Dhaka
Proceedings of the Ninth International Space Syntax Symposium Edited by Y O Kim, H T Park and K W Seo, Seoul: Sejong University, 2013 INTEGRATING LAND WITH WATER ROUTES: Proposal for a sustainable spatial network for Keraniganj in Dhaka Farida Nilufar 031 Bangladesh University of Engineering & Technology e-mail : [email protected] Labib Hossain Bangladesh University of Engineering & Technology e-mail : [email protected] Mahbuba Afroz Jinia Stamford University Bangladesh e-mail : [email protected] Abstract Cities in the delta have unique spatial character being criss-crossed by rivers and canals. Keraniganj Upazila of Dhaka District is a settlement surrounded by two big rivers which are again connected by a canal network. The spatial network of Keraniganj, therefore, has got some significance due to its connectivity with the water-ways. However, as a result of many insentient manmade efforts, the water-ways of this settlement did not developed to any integrated system with the surface routes. Canals are being used as drainage channels or being filled up. Moreover, seasonal floods have detrimental effects on the land-use and infrastructure. As a result the potential development of Keraniganj is being hampered. A new land-use proposal under Detailed Area Plan (DAP) is in process of implementation. Besides, the inhabitants are trying to develop their own solution through a number of local roads. None of them, the professionals or the locals, ever takes the challenge to live negotiating with nature. It appears that the spatial characteristics of the existing and proposed network need to be explored in order to evolve a sustainable spatial network for Keraniganj. -

Zila Report : Narayanganj
POPULATION & HOUSING CENSUS 2011 ZILA REPORT : NARAYANGANJ Bangladesh Bureau of Statistics Statistics and Informatics Division Ministry of Planning BANGLADESH POPULATION AND HOUSING CENSUS 2011 Zila Report: NARAYANGANJ October 2015 BANGLADESH BUREAU OF STATISTICS (BBS) STATISTICS AND INFORMATICS DIVISION (SID) MINISTRY OF PLANNING GOVERNMENT OF THE PEOPLE’S REPUBLIC OF BANGLADESH ISBN-978-984-33-8615-1 COMPLIMENTARY Published by Bangladesh Bureau of Statistics (BBS) Statistics and Informatics Division (SID) Ministry of Planning Website: www.bbs.gov.bd This book or any portion thereof cannot be copied, microfilmed or reproduced for any commercial purpose. Data therein can, however, be used and published with acknowledgement of their sources. Contents Page Message of Honorable Minister, Ministry of Planning …………………………………………….. vii Message of Honorable State Minister, Ministry of Finance and Ministry of Planning …………. ix Foreword ……………………………………………………………………………………………….. xi Preface …………………………………………………………………………………………………. xiii Zila at a Glance ………………………………………………………………………………………... xv Physical Features ……………………………………………………………………………………... xix Zila Map ………………………………………………………………………………………………… xxi Geo-code ………………………………………………………………………………………………. xxii Chapter-1: Introductory Notes on Census ………………………………………………………….. 1 1.1 Introduction ………………………………………………………………………………… 1 1.2 Census and its periodicity ………………………………………………………………... 1 1.3 Objectives ………………………………………………………………………………….. 1 1.4 Census Phases …………………………………………………………………………… 2 1.5 Census Planning …………………………………………………………………………. -

Bangladesh Rice Journal Bangladesh Rice Journal
ISSN 1025-7330 BANGLADESH RICE JOURNAL BANGLADESH RICE JOURNAL BANGLADESH RICE JOURNAL VOL. 21 NO. 2 (SPECIAL ISSUE) DECEMBER 2017 The Bangladesh Rice Journal is published in June and December by the Bangladesh Rice Research Institute (BRRI). The journal is a peer reviewed one based on original Theme : Cropping Patterns of Bangladesh research related to rice science. The manuscript should be less than eight printed journal pages or about 12 type written pages. An article submitted to the Bangladesh Rice Journal must not have been published in or accepted for publication by any other journal. DECEMBER 2017 ISSUE) NO. 2 (SPECIAL VOL. 21 Changes of address should be informed immediately. Claims for copies, which failed to reach the paid subscribers must be informed to the Chief Editor within three months of the publication date. Authors will be asked to modify the manuscripts according to the comments of the reviewers and send back two corrected copies and the original copy together to the Chief Editor within the specified time, failing of which the paper may not be printed in the current issue of the journal. BRJ: Publication no.: 263; 2000 copies BANGLADESH RICE RESEARCH INSTITUTE Published by the Director General, Bangladesh Rice Research Institute, Gazipur 1701, Bangladesh GAZIPUR 1701, BANGLADESH Printed by Swasti Printers, 25/1, Nilkhet, Babupura, Dhaka 1205 ISSN 1025-7330 BANGLADESH RICE JOURNAL VOL. 21 NO. 2 (SPECIAL ISSUE) DECEMBER 2017 Editorial Board Chief Editor Dr Md Shahjahan Kabir Executive Editors Dr Md Ansar Ali Dr Tamal Lata Aditya Associate Editors Dr Krishna Pada Halder Dr Md Abdul Latif Dr Abhijit Shaha Dr Munnujan Khanam Dr AKM Saiful Islam M A Kashem PREFACE Bangladesh Rice Journal acts as an official focal point for the delivery of scientific findings related to rice research. -

Floristic Diversity of Dhamrai Upazila of Dhaka with Emphasis on Medicinal Plants
Bangladesh J. Bot. 41(1): 71-85, 2012 (June) FLORISTIC DIVERSITY OF DHAMRAI UPAZILA OF DHAKA WITH EMPHASIS ON MEDICINAL PLANTS M OLIUR RAHMAN*, RUMANA TANJIN ANTARA, MOMTAZ BEGUM AND MD ABUL HASSAN Department of Botany, University of Dhaka, Dhaka 1000, Bangladesh Key words: Angiosperm diversity, Dhamrai, Medicinal plants, Bangladesh Abstract A total of 263 angiosperm species under 210 genera and 79 families have been recorded from Dhamrai Upazila of Dhaka district. Of these, Magnoliopsida is represented by 200 species under 154 genera and 62 families while Liliopsida is represented by 63 species under 56 genera and 17 families. Asteraceae is the largest family in Magnoliopsida represented by 17 species, and Poaceae is the largest family in Liliopsida represented by 20 species. Habit analysis shows that herbs, shrubs and trees are represented by 166, 23 and 74 species, respectively. Sixty two medicinal plants have been documented with their uses for the cure of more than 30 diseases, and some of these are diabetes, jaundice, diarrhoea, dysentery, spleen and liver complaints, chronic ulcers, bronchitis, rheumatism, irregular menstruation, piles, urinary problems and heart diseases. Threats to the species have also been assessed and appropriate conservation measures suggested. Introduction Dhamrai is one of the five Upazilas of Dhaka district with an area of 307.4 km2 and is situated about 38 km north-west of Dhaka metropolis. It is located at 23º55΄ N and 90º14΄E. Dhamrai represents an undulating area with conspicuous crests and troughs. The soil is a heterogenous assortment of dry, moist and clay material. The crest soils are represented by three different types, namely brownish grey fine sandy loam, dark grey fine sandy loam and grey fine sandy loam. -

Study of Circulation Spaces in the Schools of Dhaka in Terms of Safety
STUDY OF CIRCULATION SPACES IN THE SCHOOLS OF DHAKA IN TERMS OF SAFETY SADIA BINTE AMIN A thesis submitted in partial fulfilment of the requirement for the degree of MASTER OF ARCHITECTURE March, 2019 Department of Architecture BANGLADESH UNIVERSITY OF ENGINEERING & TECHNOLOGY Dhaka, Bangladesh. ii CANDIDATE’S DECLARATION It is declared that this thesis or any part of it has not been submitted elsewhere for the award of degree or diploma. Signature: ------------------------------------------ Name iii TO MY PARENTS iv ACpKNOWLEDGEMENT Foremost, I would like to express my deep gratitude to Almighty Allah for being able to complete my task successfully. I am also very grateful to my supervisor Mohammed Tarek Haider, Assistant Professor, Department of Architecture, BUET, for his valuable guidance, untiring support and continuous supervision throughout my research work. My sincere gratitude is also extended Professor Dr. Nasreen Hossain, Head of the Department of Architecture, BUET, Professor Dr. Md. Ashikur Rahman Joarder, Department of Architecture, BUET , Dr. Nayma Khan, Associate Professor, Department of Architecture, BUET and Professor Dr. Nizamuddin Ahmed for their valuable suggestions and kind advice. I am extremely thankful to Moushumi Ahmed, Assistant Professor, Department of Architecture, Bangladesh University (BU) for her guidance and encouragement to my work. I would like to thank all the Principals of relevant School of Dhaka City for allowing me to carry out survey in their schools and rendering their valuable support. I feel extremely honoured to receive the accurate requisite data and information from concerned students & staff of the above institutions mentioned on time as and when sought. I would also like to mention the support of Emdad Hossain Riyad and Sakib Abdullah Khan, student of the Department of Architecture, AUST and Architect Rafi for helping me in conducting survey and gathering information. -

Sustainable Solid Waste Management Through 3R Strategy in Gazipur City Corporation
Sustainable Solid Waste Management Through 3R Strategy in Gazipur City Corporation By ABDULLAH RUMI SHISHIR PROMI ISLAM ISLAMIC UNIVERSITY OF TECHNOLOGY (IUT) 2016 i Sustainable Solid Waste Management Through 3R Strategy in Gazipur City Corporation By Abdullah Rumi Shishir (Student id 125423) Promi Islam (Student id 125447) A THESIS SUBMITTED FOR THE DEGREE OF BACHELOR OF SCIENCE IN CIVIL ENGINEERING DEPARTMENT OF CIVIL AND ENVIRONMENTAL ENGINEERING ISLAMIC UNIVERSITY OF TECHNOLOGY NOVEMBER, 2015 iii iv APPROVAL The thesis titled ―Sustainable solid waste management through 3R strategy in Gazipur city corporation‖ submitted by Abdullah Rumi Shishir (Student ID 125423), Promi Islam (Student ID 125447) of Academic Year 2012-16 has been found as satisfactory and accepted as partial fulfillment of the requirement for the degree of Bachelor of Science in Civil Engineering. SUPERVISOR DR. MD. REZAUL KARIM Professor Department of Civil and Environmental Engineering (CEE) Islamic University of Technology (IUT) v DECLARATION We hereby declare that the undergraduate project work reported in this thesis has been performed by us and this work has not been submitted elsewhere for the award of any degree or diploma. November 2016 Abdullah Rumi Shishir (125423) Promi Islam (125447) vi DEDICATED TO OUR BELOVED PARENTS vii ACKNOWLEDGEMENTS In the name of Allah, Most Gracious, Most Merciful All praises belongs to the almighty Allah for giving us the strength and courage to successfully complete our B.Sc. thesis. We would like to express our sincere appreciation to our Supervisor Dr. Md. Rezaul Karim, Professor, Department of Civil and Environmental Engineering, Islamic University of Technology (IUT), for his generous guidance, advice and encouragement in supervising us. -

Ashuganj 400 MW Combined Cycle Power Plant (East)
Environmental Impact Assessment (Annex 16-Part 2) May 2016 Bangladesh: Power System Expansion and Efficiency Improvement Investment Program (Tranche 3) Ashuganj 400 MW Combined Cycle Power Plant (East) Prepared by Ashuganj Power Station Company Limited (APSCL) for the Asian Development Bank. This is an updated version of the draft EIA posted in October 2015 available on http://www.adb.org/projects/documents/ashuganj-400mw-ccpp-east-updated-eia This environmental impact assessment is a document of the borrower. The views expressed herein do not necessarily represent those of ADB's Board of Directors, Management, or staff, and may be preliminary in nature. Your attention is directed to the “terms of use” section on ADB’s website. In preparing any country program or strategy, financing any project, or by making any designation of or reference to a particular territory or geographic area in this document, the Asian Development Bank does not intend to make any judgments as to the legal or other status of any territory or area. Erosion The Meghna river banks suffer from erosion problems annually, mostly in the monsoon and post monsoon periods. As the transmission line will not have any impact on erosion, a further detailed analysis of erosion was not required for the project. Flooding Flooding situation of the study area is very nominal. The local people informed that, only the historical flash flood occurred in the year of 1988, 1998 and 2004. Flooding of 1988 and 1998 severely affected almost the entire study area. The duration of 1988 and 1998 flood was around 1-1.5 months with flood level of 6-7 ft. -

Invitation for E-Tender (LTM)-Furniture-1St
GOVERNMENT OF THE PEOPLE’S REPUBLIC OF BANGLADESH OFFICE OF THE EXECUTIVE ENGINEER EDUCATION ENGINEERING DEPARTMENT, NARAYANGANJ ZONE SHIKKHA BHABAN, MASDAIR, NARAYANGANJ [email protected] Memo No: 13/EED/NZ/2019-20/1666 Date: 25/07/2019 Invitation for e-Tender (LTM)-Furniture-1st SL Last Selling Last Closing Tender ID No. Name of Works no Date & Time Date & Time Manufacturing and Supplying of furniture for Academic building to 19-Aug-2019 20-Aug-2019 1 345932 Selected Firoza Khatun Adarsha Mohila Dakhil Madrasha, Sadar 17:00 16:00 Upazila, Narayanganj District. Manufacturing and Supplying of furniture for Academic building to 19-Aug-2019 20-Aug-2019 2 345930 Selected Darussunnah Kamil Madrasha, Fatullah, Sadar Upazila, 17:00 16:00 Narayanganj District. Manufacturing and Supplying of furniture for Academic building to 19-Aug-2019 20-Aug-2019 3 345929 Selected Shadipur Islamia Senior Alim Madrasha, Sonargano Upazila, 17:00 16:00 Narayanganj District. Manufacturing and Supplying of furniture for Academic building to 19-Aug-2019 20-Aug-2019 4 345928 Selected Beldi Darul Hadis Fazil Madrasha, Rupganj Upazila, 17:00 16:00 Narayanganj District. Manufacturing and Supplying of furniture for Academic building to 19-Aug-2019 20-Aug-2019 5 345927 Selected Narayanganj High School, Sadar Upazila, Narayanganj 17:00 16:00 District. Manufacturing and Supplying of furniture for Academic building to 19-Aug-2019 20-Aug-2019 6 345926 Selected Hazi Pande Ali High School, Fatullah, Sadar Upazila, 17:00 16:00 Narayanganj District. Manufacturing and Supplying of furniture for Academic building to 19-Aug-2019 20-Aug-2019 7 345925 Selected Godnail High School, Shiddirganj, Sadar Upazila, Narayanganj 17:00 16:00 District. -
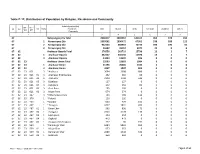
Table C-13: Distribution of Population by Religion, Residence and Community
Table C-13: Distribution of Population by Religion, Residence and Community Administrative Unit UN / MZ / ZL UZ Vill RMO Residence Total Muslim Hindu Christian Buddhist Others WA MH Community 1 2 3 4 5 6 7 8 67 Narayanganj Zila Total 2948217 2802567 144105 963 378 204 67 1 Narayanganj Zila 1959261 1890472 67951 538 188 112 67 2 Narayanganj Zila 942354 868943 72733 396 190 92 67 3 Narayanganj Zila 46602 43152 3421 29 0 0 67 02 Araihazar Upazila Total 376550 363733 12796 13 1 7 67 02 1 Araihazar Upazila 362127 350136 11970 13 1 7 67 02 3 Araihazar Upazila 14423 13597 826 0 0 0 67 02 23 Araihazar Union Total 25593 23603 1984 6 0 0 67 02 23 1 Araihazar Union 21196 20006 1184 6 0 0 67 02 23 3 Araihazar Union 4397 3597 800 0 0 0 67 02 23 021 3 *Araihazar 3694 3008 686 0 0 0 67 02 23 021 01 3 Araihazar Krishnapura 262 202 60 0 0 0 67 02 23 021 02 3 Araihazar 2294 1748 546 0 0 0 67 02 23 021 03 3 Dighirpar 127 127 0 0 0 0 67 02 23 021 04 3 Debipura 242 162 80 0 0 0 67 02 23 021 05 3 Goal Para 195 195 0 0 0 0 67 02 23 021 06 3 Nagar Para 574 574 0 0 0 0 67 02 23 247 3 *Chhota Barai Para 703 589 114 0 0 0 67 02 23 376 1 *Faitadi 126 126 0 0 0 0 67 02 23 403 1 *Gazipur 693 494 199 0 0 0 67 02 23 467 1 *Jhaugara 4237 3831 400 6 0 0 67 02 23 467 01 1 Binar Char 963 890 73 0 0 0 67 02 23 467 02 1 Jhaugara 2320 2178 136 6 0 0 67 02 23 467 03 1 Lakhupura 254 254 0 0 0 0 67 02 23 467 04 1 Dighaldi 473 473 0 0 0 0 67 02 23 467 05 1 Jhaugara Krishnapura 227 36 191 0 0 0 67 02 23 559 1 *Kamrangir Char 6384 5833 551 0 0 0 67 02 23 559 01 1 Majar Char 553 -

Evsjv‡`K †M‡RU
†iwR÷vW© bs wW G-1 ÒRvwZi wcZv e½eÜz †kL gywReyi ingv ‡bi Rb¥kZevwl©Kx D`&hvcb mdj †nvKÓ evsjv ‡`k †M‡RU AwZwi³ msL¨v KZ…©cÿ KZ…©K cÖKvwkZ iweevi, †deªæqvwi 14, 2021 ! " : $% &'( )$)% )$.$+.$$$$.,$).%-.$+..)$ -)- 0 -0 1 2( 3 %) , )$$+ 0 %- , )$$+ ! 35( 67 7 ! 1 89 : 1 :1; 1 < (1) ;? 0 @( :1; @( ;? (0 A) 1 @( B (0: ) 67 C DE F 1 (-(G ;H7 I ; <J7 (5 <) KL4 8M N( O P, 0 @ (G; 9 @ OQ 0M DE 99 R( : 5 P S ( 9 T 6G 0U VJW U X :Y। 1 , 0 A 1 0: ’ :1; \7 ] O^, 8 ,7 _ J R( 3; Q O F 1 $, 3( )$)% " T G 89, , (-(G ;7 1 `^ <J7 KL QJ X VJW U 3B (। a S 1 5<5< 6Q7 3` \a ] O^, 8 7 1 _ ^ba7 J c< 7 dH;7 : ( 5063 ) g~j¨ : UvKv 168.00 5064 0 A 1 0: 0 :1( _ ba 9 O F ()ef- U ) : g h _ -' ' (ijJ 7 ).$ HH 0 kl7) Name of Road Road Length Proposed SL No. Road ID Road Name Upazila Classification (Km) Ownership a, _, 1 2 3 4 5 6 7 Keraniganj 1 326385774 VR-B Agrokhola Noya Bari - Noyagaon Road 2.00 LGED Bottoli Natunhati Culvert - Aman Shaheb Bari via Uttar Baher 2 326385775 VR-B 2.80 Char Connectivity Road 3 326385776 VR-B Uttor Baherchar Mokkanagar Road 2.00 4 326385777 VR-B Chunkutia Aminpara Kanapotty - Mirerbag Road 2.00 &'( %- &'( 5 326385778 VR-B Ruhitpur RHD - Sonakanda Pucca Road via Katbagan 2.00 6 326385779 VR-B Lakhirchar Dayna Mill Ghat - Mugharchar Road 2.00 Pucca Road 2.00 ,)$)% 7 326385780 VR-B Shahpur Jilani Mia House - Bottola Chatircha Bazar UZR - Char Ruhitpur UNR via Shoburnasur 8 326385781 VR-B 2.00 Road 9 326385782 VR-B Belna Khaskandi(RHD) - Joinpur UZR Road 2.00 10 326385783 VR-B Kuraisnagar Main Road - Adu Pagla House Road 2.00 11 326385784 VR-B Bounakandi Madrasha - Ring Road. -

Environmental Assessment Report
Environmental Assessment Report Union Road (UNR) Name of the Sub-project : Nekrozbag R&H to Dhaka Mawa Road at Abdullahpur via Muktirbag & Firm Ratan Road. Slice No. : UNR-12 (III) Upazila : Keraniganj District : Dhaka Second Rural Transport Improvement Project Local Government Engineering Department Environmental Assessment Report Contents 1. Sub Project Description ............................................................................................................................3 2. Detail Environmental Features .................................................................................................................5 3. Baseline Data: Physical Environment ......................................................................................................6 4. Screening Format ......................................................................................................................................9 5. Specific Impact and Mitigation ............................................................................................................. 13 6. Environmental Management Plan ......................................................................................................... 15 7. EMP in Bidding Document ................................................................................................................... 20 Annex-1: Public Consultation ....................................................................................................................... 21 Second Rural Transport Improvement