Neuroglial Choristoma of the Middle Ear with Massive Tympanosclerosis: a Case Report and Literature Review
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
A Post-Tympanoplasty Evaluation of the Factors Affecting Development of Myringosclerosis in the Graft: a Clinical Study
Int Adv Otol 2014; 10(2): 102-6 • DOI: 10.5152/iao.2014.40 Original Article A Post-Tympanoplasty Evaluation of the Factors Affecting Development of Myringosclerosis in the Graft: A Clinical Study Can Özbay, Rıza Dündar, Erkan Kulduk, Kemal Fatih Soy, Mehmet Aslan, Hüseyin Katılmış Department of Otorhinolaryngology, Şifa University Faculty of Medicine, İzmir, Turkey (CÖ) Department of Otorhinolaryngology, Mardin State Hospital, Mardin, Turkey (RD, EK, KFS, MA) Department of Otorhinolaryngology, Katip Çelebi University Atatürk Training and Research Hospital, İzmir, Turkey (HK) OBJECTIVE: Myringosclerosis (MS) is a pathological condition characterized by hyaline degeneration and calcification of the collagenous structure of the fibrotic layer of the tympanic membrane, which may develop after trauma, infection, or inflammation as myringotomy, insertion of a ventila- tion tube, or myringoplasty. The aim of our study was to both reveal and evaluate the impact of the factors that might be effective on the post-tym- panoplasty development of myringosclerosis in the graft. MATERIALS and METHODS: In line with this objective, a total of 108 patients (44 males and 64 females) aged between 11 and 66 years (mean age, 29.5 years) who had undergone type 1 tympanoplasty (TP) with an intact canal wall technique and type 2 TP, followed up for an average of 38.8 months, were evaluated. In the presence of myringosclerosis, in consideration of the tympanic membrane (TM) quadrants involved, the influential factors were analyzed in our study, together with the development of myringosclerosis, including preoperative factors, such as the presence of myringosclerosis in the residual and also contralateral tympanic membrane, extent and location of the perforation, and perioperative factors, such as tympanosclerosis in the middle ear and mastoid cavity, cholesteatoma, granulation tissue, and type of the operation performed. -

Hearing Loss in Patients with Extracranial Complications of Chronic Otitis Media
ORIGINAL ARTICLE Hearing loss in patients with extracranial complications of chronic otitis media Authors’ Contribution: BCDE AF A – Study Design Tomasz Przewoźny , Jerzy Kuczkowski B – Data Collection C – Statistical Analysis D – Data Interpretation Department of Otolaryngology, Medical University of Gdańsk, Gdańsk, Poland E – Manuscript Preparation F – Literature Search G – Funds Collection Article history: Received: 13.04.2017 Accepted: 10.04.2017 Published: 15.06.2017 ABSTRACT: Objective: A pure tone audiomety analysis of patients with extracranial complications of chronic suppurative otitis media (ECCSOM). Material and methods: We retrospectively analyzed audiometric data performed before treatment from 63 pa- tients with ECCSOM (56 single, 7 multiple complications) including groups of frequencies. Results: The greatest levels of hearing loss were noted for 6 and 8 kHz (79.0 and 75.7 dBHL) and for the frequency groups high tone average (76.1 dBHL). As regards the severity of hearing impairment in pure tone average the prev- alence of complications was as follows: labyrinthitis (77.8±33.6 dBHL), facial palsy (57.1±14.3 dBHL), perilymphatic fistula (53.9±19.9 dBHL) and mastoiditis (42.2±9.5 dBHL) (p=0.023). Conclusions: Hearing loss in ECCSOM is dominated by mixed, high-tone, moderate type of hearing loss, most pro- found in labyrinthitis. In 11% of patients the complication causes total deafness. KEYWORDS: chronic suppurative otitis media, complications extracranial, hearing loss INTRODUCTION ing discharge from the ear and mixed or conductive hearing loss can be observed [4-5]. Labyrinthitis is associated with Chronic suppurative otitis media (CSOM) is a destructive slowly progressive high-frequency sensorineural hearing loss disease of the ear. -
Tympanic Membrane Perforations: the Safe Versus the Unsafe
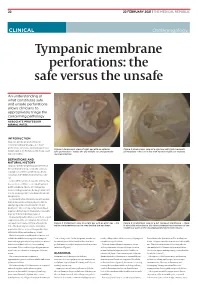
TMR_210222_22 2021-02-12T14:56:54+11:00 22 22 FEBRUARY 2021 | THE MEDICAL REPUBLIC CLINICAL Otolaryngology Tympanic membrane perforations: the safe versus the unsafe An understanding of what constitutes safe and unsafe perforations allows clinicians to appropriately triage the concerning pathology ASSOCIATE PROFESSOR NIRMAL PATEL INTRODUCTION Tympanic membrane perforations are seen frequently in general practice. Some perforations can be associated with significant Figure 1: Endoscopic view of right ear with an anterior Figure 2: Endoscopic view of a right ear with twin traumatic disease, such as cholesteatoma which may cause safe perforation – notice the dry middle ear and posterior perforations – the ear is dry with normal middle ear mucosa. major morbidity. myringosclerosis DEFINITIONS AND NATURAL HISTORY Tympanic membrane perforations are holes in the ear drum that most commonly occur as a consequence of either ear infections, chronic eustachian tube dysfunction or trauma to the ear. Acute middle ear infection (acute otitis media) is a common condition occurring at least once in 80% of children. Most acute otitis media resolves with spontaneous discharge of infected secretions through the eustachian tube into the nasopharynx. Occasionally when the infections are frequent, there is extensive scarring (tympanosclerosis and myringosclerosis) of the ear drum and middle ear . This scarring compromises blood supply to the healing ear drum and occasionally stops the hole from healing. (Figure 1) Traumatically induced holes occur from a rapid compression of the air column in the external ear canal, most commonly from a blow to the Figure 3: Endoscopic view of a right ear with an attic wax – the Figure 4: Endoscopic view of a left tympanic membrane – there white cholesteatoma can be seen behind the ear drum. -

ICD-9 Diseases of the Ear and Mastoid Process 380-389
DISEASES OF THE EAR AND MASTOID PROCESS (380-389) 380 Disorders of external ear 380.0 Perichondritis of pinna Perichondritis of auricle 380.00 Perichondritis of pinna, unspecified 380.01 Acute perichondritis of pinna 380.02 Chronic perichondritis of pinna 380.1 Infective otitis externa 380.10 Infective otitis externa, unspecified Otitis externa (acute): NOS circumscribed diffuse hemorrhagica infective NOS 380.11 Acute infection of pinna Excludes: furuncular otitis externa (680.0) 380.12 Acute swimmers' ear Beach ear Tank ear 380.13 Other acute infections of external ear Code first underlying disease, as: erysipelas (035) impetigo (684) seborrheic dermatitis (690.10-690.18) Excludes: herpes simplex (054.73) herpes zoster (053.71) 380.14 Malignant otitis externa 380.15 Chronic mycotic otitis externa Code first underlying disease, as: aspergillosis (117.3) otomycosis NOS (111.9) Excludes: candidal otitis externa (112.82) 380.16 Other chronic infective otitis externa Chronic infective otitis externa NOS 380.2 Other otitis externa 380.21 Cholesteatoma of external ear Keratosis obturans of external ear (canal) Excludes: cholesteatoma NOS (385.30-385.35) postmastoidectomy (383.32) 380.22 Other acute otitis externa Excerpted from “Dtab04.RTF” downloaded from website regarding ICD-9-CM 1 of 11 Acute otitis externa: actinic chemical contact eczematoid reactive 380.23 Other chronic otitis externa Chronic otitis externa NOS 380.3 Noninfectious disorders of pinna 380.30 Disorder of pinna, unspecified 380.31 Hematoma of auricle or pinna 380.32 Acquired -

Hearing Loss, Vertigo and Tinnitus
HEARING LOSS, VERTIGO AND TINNITUS Jonathan Lara, DO April 29, 2012 Hearing Loss Facts S Men are more likely to experience hearing loss than women. S Approximately 17 percent (36 million) of American adults report some degree of hearing loss. S About 2 to 3 out of every 1,000 children in the United States are born deaf or hard-of-hearing. S Nine out of every 10 children who are born deaf are born to parents who can hear. Hearing Loss Facts S The NIDCD estimates that approximately 15 percent (26 million) of Americans between the ages of 20 and 69 have high frequency hearing loss due to exposure to loud sounds or noise at work or in leisure activities. S Only 1 out of 5 people who could benefit from a hearing aid actually wears one. S Three out of 4 children experience ear infection (otitis media) by the time they are 3 years old. Hearing Loss Facts S There is a strong relationship between age and reported hearing loss: 18 percent of American adults 45-64 years old, 30 percent of adults 65-74 years old, and 47 percent of adults 75 years old or older have a hearing impairment. S Roughly 25 million Americans have experienced tinnitus. S Approximately 4,000 new cases of sudden deafness occur each year in the United States. Hearing Loss Facts S Approximately 615,000 individuals have been diagnosed with Ménière's disease in the United States. Another 45,500 are newly diagnosed each year. S One out of every 100,000 individuals per year develops an acoustic neurinoma (vestibular schwannoma). -

Intratympanic Membrane Cholesteotoma: an Unusual Rare Case
Central Journal of Ear, Nose and Throat Disorders Bringing Excellence in Open Access Case Report *Corresponding author Mohamad Ali El Natout, Department of Otolaryngology Head & Neck Surgery, American University of Beirut Intratympanic Membrane Medical Center, P.O.Box: 11-0236, Riad El-Solh, Beirut 1107 2020, Beirut-Lebanon, USA, Tel: 96-133-449-66; Email: Cholesteotoma: An Unusual Submitted: 11 July 2016 Accepted: 23 July 2016 Rare Case Published: 01 August 2016 Copyright 1 2 1 Hayat Adib , Tamer El Natout , and Mohamad Ali El Natout * © 2016 El Natout et al. 1Department of Otolaryngology Head & Neck Surgery, American University of Beirut Medical Center, USA OPEN ACCESS 2Faculty of Medicine, American University of Beirut, USA Keywords • Intratympanic membrane Abstract • Cholesteatoma • Acquired Intraympanic membrane cholesteotoma without a preceding ear trauma or surgery is a rare entity. Only few cases have been documented in the literature. The exact etiology of this lesion is still unclear. We report an unusual case of an intratympaniccholesteatoma in an adult patient. He is a 45-year-old male who presented with ear fullness and hearing loss six months following an acute otitis media without otorrhea or a tympanic membrane perforation. Physical exam showed a central whitish area on the tympanic membrane. CT scan demonstrated thickening of the tympanic membrane. On the audiogram, he had a 20-dB air-bone gap; tympanogram showed a B-curve. We surgically explored his middle ear and encountered a central tympanic membrane 5X3 mm cholesteatoma with intact middle ear cavity. Accordingly we performed a tympanoplasty. The gold standard for diagnosis of tympanic membrane cholesteotoma is oto-microscopy. -

Tinnitus What Is Tinnitus? Tinnitus Is Defined As the Perception of Sound When No External Sound Is Present
Tinnitus What is tinnitus? Tinnitus is defined as the perception of sound when no external sound is present. The common vernacular is "ringing in the ears"; however, the quality of the tinnitus can range from roaring to hissing and chirping to clicking. Tinnitus can pulsate or be constant. It can be a single tone or multiple tones, and it's amplitude can vary from background noise to an excruciating experience. What causes tinnitus? Tinnitus has a variety of causes. The most common causes include wax in the ear canal, noise trauma or temporomandibular joint (TMJ) dysfunction. It can also be caused by Meniere's disease, endolymphatic hydrops, allergies, destruction of the middle ear bones, infection, nutritional deficiency, cardiovascular disease, thyroid disorders, certain medications, head injury and cervical disorders. Recently, migraine disorders have also been listed as a culprit. Regardless of the inciting etiology, it has been shown that the it is within the brain that the sound resides, persists, evolves and propagates. Tinnitus may begin with damage to the peripheral auditory system (the cochlea and auditory nerve), but its persistence is a function of the attention that it receives parietal cortex and frontal cortex), the importance that it is given (cingulate cortex, anterior insula) and it maintaining residence in the limbic system (the amygdala, hippocampus and thalamus). Ongoing research is being aggressively pursued to stop this feed-forward cycle in its tracks. Medications that may exacerbate tinnitus (adapted from Bailey's Otolaryngology - Head and Neck Surgery 4th ed.) include aspirin and aspirin-containing compounds, aminoglycoside antibiotics, nonsteroidal antiinflammatory drugs and heterocycline antidepressants. -

Neurootological Evaluation of Tinnitus
International Tinnitus Journal 1, 93-97 (1995) Neurootological Evaluation of Tinnitus J. c. R. Seabra, M.D., H. Diamantino, M.D., J. Faria e Almeida, M.D. Ear, Nose and Throat Department, Vila Nova de Gaia, Portugal Abstract: We analyse the neurootological data of patients attended in the Ear, Nose and Throat (E.N.T.) department of the Centro Hospitalar de Vila Nova de Gaia for a tinnitus problem. We submitted these patients to our neurootological routine evaluation. This approach is justified in a tinnitus patient because the cochleovestibular system is a unit and acts as a whole. We characterise the population that came to us by sex and mean age. The profile of these patients is then analysed by our neurootological routine evaluation, which comprises the history taking and audiometric as well as equilibriometric investigations. The results of the audiovestibulometric examinations - pure tone audiometry, vocal audiometry, and Brain Evoked Response Audiometry (B.E.R.A.), Cranio-Corpo Graphy (C.C.G.), Electronystagmography (E.N.G.) - are discussed. We concluded that many tinnitus patients, even those who had no vestibular symptoms, showed some disturbances in the vestibular tests. This fact highlights the need for a complete cochleovestibular investigation in all patients complaining about tinnitus. INTRODUCTION middle ear disease, such as chronic otitis, tympanic perforations, or tympanosclerosis. innitus is a widespread symptom that mortifies We investigated 44 patients, 19 men and 25 women, with T patients and frustrates doctors. It may be the only a mean age of 48-years (standard deviation being 12). symptom complained by patients, but commonly The patients underwent our routine neurootological it is associated with neurosensory hearing loss and/or examination which comprises: vertigo. -

Lyric 24/7 Hearing: Could It Help Those with Tinnitus?
Lyric 24/7 hearing: could it help those with tinnitus? Jacob Johnson, Medical Director, Lyric, Phonak Silicone Valley; Associate Clinical About Lyric Hearing The tinnitus dilemma Professor, Department Since its launch in 2008, Lyric represents Subjective tinnitus, the phantom percep- of Otolaryngology, the first and only device of its kind estab- tion of sound with no identifiable sound Head & Neck Surgery, University of California – lishing a new category of hearing solution: source, significantly reduces an individual’s San Francisco; 24/7 extended wear. Lyric is placed several quality of life [1]. The tinnitus patient lives President, San Francisco millimetres within the ear canal, near the with a complex constellation of symptoms Audiology; Physician Partner tympanic membrane, so it is 100% invisible, including challenges to sleep, concentra- (Otolaryngologist), and worn 24 hours a day for months at a tion, and cognition that, over time, can San Francisco Otolaryngology Medical time. Lyric is worn during all daily activities include anxiety, anger, depression, and loss Group. including showering, sleeping and exer- of control [2]. Additionally, these patients cising. This frees the wearer from typical have well-characterised alterations in neur- Correspondence hassles presented by traditional hearing onal activity in auditory and non-auditory E: Jacob.Johnson@ phonak.com aids, including multiple daily device inser- pathways [3]. tions or removals, battery changes, and For the practitioner, evaluation and Declaration of cleaning. Moreover, the placement of care of tinnitus is complicated by the competing interests JJ is a Consultant with the device near the tympanic membrane diversity of clinical presentations, the lack Phonak. enables the anatomy of the ear to naturally of a single underlying cause (Table 1), transform sound before it enters the Lyric patient co-morbidities, wide promotion Article was first published in microphone for amplification (Figure 1). -

Giant Congenital Cholesteatoma of the Temporal Bone
Global Journal of Otolaryngology ISSN 2474-7556 Case Report Glob J Otolaryngol Volume 18 Issue 5 - January 2019 Copyright © All rights are reserved by Cristina Laza DOI: 10.19080/GJO.2019.18.555998 Giant Congenital Cholesteatoma of the Temporal Bone Cristina Laza* and Eugenia Enciu Clinical county hospital for emergencies Constanta, Romania Submission: December 15, 2018; Published: January 03, 2019 *Corresponding author: Cristina Laza, Clinical county hospital for emergencies Constanta, Romania Abstract Congenital or primitive cholesteatoma is a benign disease with slow progressive growth that destroys neighboring structures. It is a rare disease considered an epidermal cyst originating from the remnants of squamous keratinized epithelium, in several regions of the temporal bone such as in the middle ear (most frequent) as well as in the petrous apex, cerebellopontine cistern, external acoustic meatus and mastoid process. In this case report, we present a giant congenital cholesteatoma, occupying a part of the petrous part of the temporal bone, including middle ear and mastoid process discovered at a 12-years-old girl as an acute right otomastoiditis complicated with retro auricular abscess. There were no history of ear infections, trauma or previous surgeries on this area, the eardrum was intact, all the accusing starts after an infection of the naos- pharynx –typical for congenital cholesteatoma. In emergency using a retro auricular approach we drain the abscess located sub-periosteal a minutia’s excision of the cholesteatoma and a permanent follow up recurrence was discovered after 4 years at 16 years old –without signs of infectionand finally but we with remove tinnitus the andcholesteatoma vertigo and usingwe explore a radical the mastoidectomycavity and remove with the canal new wallcholesteatoma. -

Differential Diagnosis and Treatment of Hearing Loss JON E
Differential Diagnosis and Treatment of Hearing Loss JON E. ISAACSON, M.D., and NEIL M. VORA, M.D., Milton S. Hershey Medical Center, Hershey, Pennsylvania Hearing loss is a common problem that can occur at any age and makes verbal communication difficult. The ear is divided anatomically into three sections (external, middle, and inner), and pathology contributing to hearing loss may strike one or more sections. Hearing loss can be cat- egorized as conductive, sensorineural, or both. Leading causes of conductive hearing loss include cerumen impaction, otitis media, and otosclerosis. Leading causes of sensorineural hear- ing loss include inherited disorders, noise exposure, and presbycusis. An understanding of the indications for medical management, surgical treatment, and amplification can help the family physician provide more effective care for these patients. (Am Fam Physician 2003;68:1125-32. Copyright© 2003 American Academy of Family Physicians) ore than 28 million Amer- tive, the sound will be heard best in the icans have some degree of affected ear. If the loss is sensorineural, the hearing impairment. The sound will be heard best in the normal ear. differential diagnosis of The sound remains midline in patients with hearing loss can be sim- normal hearing. Mplified by considering the three major cate- The Rinne test compares air conduction gories of loss. Conductive hearing loss occurs with bone conduction. The tuning fork is when sound conduction is impeded through struck softly and placed on the mastoid bone the external ear, the middle ear, or both. Sen- (bone conduction). When the patient no sorineural hearing loss occurs when there is a longer can hear the sound, the tuning fork is problem within the cochlea or the neural placed adjacent to the ear canal (air conduc- pathway to the auditory cortex. -

Life's Worth Hearing
Life’s worth hearing Exploring a Cochlear™ Bone Conduction Solution Opening up a new world of sound When you live with hearing loss, you’re not simply missing out on sounds, you could be missing out on life. It’s time to get back what you’ve been missing. If you struggle to hear because of conditions such as draining ears, chronic ear infections, acoustic neuroma or Microtia and Atresia, a bone conduction solution may be what you have been waiting for. 2 “ My hearing loss no longer slows me down. The Baha System keeps up with me and my active lifestyle.” Tiff any – Baha recipient 3 Hope when you need it most Every hearing loss is different and the causes vary from person to person. Your hearing loss may affect one ear or both ears and it may stem from a problem in the inner, middle or outer ear. Depending on the degree of hearing loss and which part of the ear is damaged, a bone conduction solution can help you regain access to the sounds you have been missing. Cochlear™ bone conduction solutions are clinically proven medical treatment options for those with single-sided deafness, conductive hearing loss or mixed hearing loss. Single-sided deafness Conductive hearing loss Mixed hearing loss Sensorineural hearing loss in one When your outer or middle ear is Refers to a combination of ear where you have little or no damaged and prevents sound from conductive and sensorineural hearing in that ear, but normal reaching your inner ear. hearing loss. This means there hearing in the other ear.