ICD-9 Diseases of the Ear and Mastoid Process 380-389
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
A Post-Tympanoplasty Evaluation of the Factors Affecting Development of Myringosclerosis in the Graft: a Clinical Study
Int Adv Otol 2014; 10(2): 102-6 • DOI: 10.5152/iao.2014.40 Original Article A Post-Tympanoplasty Evaluation of the Factors Affecting Development of Myringosclerosis in the Graft: A Clinical Study Can Özbay, Rıza Dündar, Erkan Kulduk, Kemal Fatih Soy, Mehmet Aslan, Hüseyin Katılmış Department of Otorhinolaryngology, Şifa University Faculty of Medicine, İzmir, Turkey (CÖ) Department of Otorhinolaryngology, Mardin State Hospital, Mardin, Turkey (RD, EK, KFS, MA) Department of Otorhinolaryngology, Katip Çelebi University Atatürk Training and Research Hospital, İzmir, Turkey (HK) OBJECTIVE: Myringosclerosis (MS) is a pathological condition characterized by hyaline degeneration and calcification of the collagenous structure of the fibrotic layer of the tympanic membrane, which may develop after trauma, infection, or inflammation as myringotomy, insertion of a ventila- tion tube, or myringoplasty. The aim of our study was to both reveal and evaluate the impact of the factors that might be effective on the post-tym- panoplasty development of myringosclerosis in the graft. MATERIALS and METHODS: In line with this objective, a total of 108 patients (44 males and 64 females) aged between 11 and 66 years (mean age, 29.5 years) who had undergone type 1 tympanoplasty (TP) with an intact canal wall technique and type 2 TP, followed up for an average of 38.8 months, were evaluated. In the presence of myringosclerosis, in consideration of the tympanic membrane (TM) quadrants involved, the influential factors were analyzed in our study, together with the development of myringosclerosis, including preoperative factors, such as the presence of myringosclerosis in the residual and also contralateral tympanic membrane, extent and location of the perforation, and perioperative factors, such as tympanosclerosis in the middle ear and mastoid cavity, cholesteatoma, granulation tissue, and type of the operation performed. -

Common Urgent ENT Problems APRIL 4, 2019 GERARD MACDONALD MD FRCS
3/21/2019 Common Urgent ENT Problems APRIL 4, 2019 GERARD MACDONALD MD FRCS 1 Course Objectives A review of common Urgent ENT problems presenting to office and ER Clinical Pearls to help you manage in a timely fashion Knowing when to refer 2 1 3/21/2019 I do not have any Conflicts of Interest 3 Top Ten List Of Urgent Calls 1.Acute Otitis Externa 2. Sudden Hearing Loss 3.Facial Palsy 4.Salivary Gland Stone /Infection 5.Peritonsillar Abscess 6.Neck Abscess 7.Nosebleeds 8.Hoarseness 9.Foreign Bodies Ear/Nose 10. Acute Vertigo 4 2 3/21/2019 Acute Otitis Externa Commonly associated with swimming ( swimmer’s ear) Common in diabetics and habitual Q-tip Users Usual presenting symptoms are itching, discharge, pain and swelling. More severe symptoms can include severe pain, parotid swelling,trismus and cellulitiis Most common organism is Pseudomonas Aeruginosa May go on to develop secondary otomycosis if frequent use of topical antibiotics. Malignant External Otitis rare but serious 5 Acute Otitis Externa 6 3 3/21/2019 Acute Otitis Externa - Treatment Debridement/Suctioning ? Culture Avoid syringing Ototopicals : Tobradex, Sofracort, Ciprodex Otowick if canal swollen shut Oral Antibiotic ( Cipro ) and single dose Steroid if severe When to refer : Unrelenting pain and swelling, facial nerve weakness,dysphagia , fever 7 Sudden hearing Loss UNEXPLAINED sudden sensorineural hearing loss occurring over 3 days Not AOM, trauma, acoustic trauma , ototoxicity Often confused with ETD , “fluid” Poorer outcome if not recognized -

Hearing Loss in Patients with Extracranial Complications of Chronic Otitis Media
ORIGINAL ARTICLE Hearing loss in patients with extracranial complications of chronic otitis media Authors’ Contribution: BCDE AF A – Study Design Tomasz Przewoźny , Jerzy Kuczkowski B – Data Collection C – Statistical Analysis D – Data Interpretation Department of Otolaryngology, Medical University of Gdańsk, Gdańsk, Poland E – Manuscript Preparation F – Literature Search G – Funds Collection Article history: Received: 13.04.2017 Accepted: 10.04.2017 Published: 15.06.2017 ABSTRACT: Objective: A pure tone audiomety analysis of patients with extracranial complications of chronic suppurative otitis media (ECCSOM). Material and methods: We retrospectively analyzed audiometric data performed before treatment from 63 pa- tients with ECCSOM (56 single, 7 multiple complications) including groups of frequencies. Results: The greatest levels of hearing loss were noted for 6 and 8 kHz (79.0 and 75.7 dBHL) and for the frequency groups high tone average (76.1 dBHL). As regards the severity of hearing impairment in pure tone average the prev- alence of complications was as follows: labyrinthitis (77.8±33.6 dBHL), facial palsy (57.1±14.3 dBHL), perilymphatic fistula (53.9±19.9 dBHL) and mastoiditis (42.2±9.5 dBHL) (p=0.023). Conclusions: Hearing loss in ECCSOM is dominated by mixed, high-tone, moderate type of hearing loss, most pro- found in labyrinthitis. In 11% of patients the complication causes total deafness. KEYWORDS: chronic suppurative otitis media, complications extracranial, hearing loss INTRODUCTION ing discharge from the ear and mixed or conductive hearing loss can be observed [4-5]. Labyrinthitis is associated with Chronic suppurative otitis media (CSOM) is a destructive slowly progressive high-frequency sensorineural hearing loss disease of the ear. -

Definitions and Background
1 Definitions and Background Tinnitus is a surprisingly complex subject. Numer- ears.” And, in fact, the word “tinnitus” is derived ous books would be required to adequately cover the from the Latin word tinniere, which means “to current body of knowledge. The present handbook ring.” Patients report many different sounds—not focuses on describing procedures for providing just ringing—when describing the sound of their clinical services for tinnitus using the methodology tinnitus, as we discuss later in this chapter. of progressive tinnitus management (PTM). In this opening chapter we establish common ground with respect to terminology and contextual Transient Ear Noise information. Relevant definitions are provided, many of which are operational due to lack of consensus It seems that almost everyone experiences “tran- in the field. Additional background information sient ear noise,” which typically is described as a includes brief descriptions of epidemiologic data, sudden whistling sound accompanied by the per- patient data, and conditions related to reduced tol- ception of hearing loss (Kiang, Moxon, & Levine, erance (hypersensitivity) to sound. 1970). No systematic studies have been published to date describing the prevalence and properties of transient ear noise; thus, anything known about Basic Concepts and Terminology this phenomenon is anecdotal. The transient auditory event is unilateral and seems to occur completely at random without any- Tinnitus is the experience of perceiving sound that thing precipitating the sudden onset of symptoms. is not produced by a source outside of the body. The Often the ear feels blocked during the episode. The “phantom” auditory perception is generated some- symptoms generally dissipate within a period of where in the auditory pathways or in the head or about a minute. -
Tympanic Membrane Perforations: the Safe Versus the Unsafe
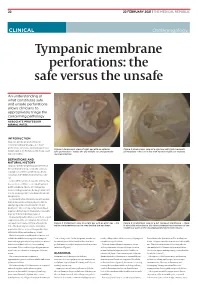
TMR_210222_22 2021-02-12T14:56:54+11:00 22 22 FEBRUARY 2021 | THE MEDICAL REPUBLIC CLINICAL Otolaryngology Tympanic membrane perforations: the safe versus the unsafe An understanding of what constitutes safe and unsafe perforations allows clinicians to appropriately triage the concerning pathology ASSOCIATE PROFESSOR NIRMAL PATEL INTRODUCTION Tympanic membrane perforations are seen frequently in general practice. Some perforations can be associated with significant Figure 1: Endoscopic view of right ear with an anterior Figure 2: Endoscopic view of a right ear with twin traumatic disease, such as cholesteatoma which may cause safe perforation – notice the dry middle ear and posterior perforations – the ear is dry with normal middle ear mucosa. major morbidity. myringosclerosis DEFINITIONS AND NATURAL HISTORY Tympanic membrane perforations are holes in the ear drum that most commonly occur as a consequence of either ear infections, chronic eustachian tube dysfunction or trauma to the ear. Acute middle ear infection (acute otitis media) is a common condition occurring at least once in 80% of children. Most acute otitis media resolves with spontaneous discharge of infected secretions through the eustachian tube into the nasopharynx. Occasionally when the infections are frequent, there is extensive scarring (tympanosclerosis and myringosclerosis) of the ear drum and middle ear . This scarring compromises blood supply to the healing ear drum and occasionally stops the hole from healing. (Figure 1) Traumatically induced holes occur from a rapid compression of the air column in the external ear canal, most commonly from a blow to the Figure 3: Endoscopic view of a right ear with an attic wax – the Figure 4: Endoscopic view of a left tympanic membrane – there white cholesteatoma can be seen behind the ear drum. -

Instruction Sheet: Otitis Externa
University of North Carolina Wilmington Abrons Student Health Center INSTRUCTION SHEET: OTITIS EXTERNA The Student Health Provider has diagnosed otitis externa, also known as external ear infection, or swimmer's ear. Otitis externa is a bacterial/fungal infection in the ear canal (the ear canal goes from the outside opening of the ear to the eardrum). Water in the ear, from swimming or bathing, makes the ear canal prone to infection. Hot and humid weather also predisposes to infection. Symptoms of otitis externa include: ear pain, fullness or itching in the ear, ear drainage, and temporary loss of hearing. These symptoms are similar to those caused by otitis media (middle ear infection). To differentiate between external ear infection and middle ear infection, the provider looks in the ear with an instrument called an otoscope. It is important to distinguish between the two infections, as they are treated differently: External otitis is treated with drops in the ear canal, while middle ear infection is sometimes treated with an antibiotic by mouth. MEASURES YOU SHOULD TAKE TO HELP TREAT EXTERNAL EAR INFECTION: 1. Use the ear drops regularly, as directed on the prescription. 2. The key to treatment is getting the drops down into the canal and keeping the medicine there. To accomplish this: Lie on your side, with the unaffected ear down. Put three to four drops in the infected ear canal, then gently pull the outer ear back and forth several times, working the medicine deeper into the ear canal. Remain still, good-ear-side-down for about 15 minutes. -

Noise-Induced Cochlear Neuronal Degeneration and Its Role in Hyperacusis- and Tinnitus-Like Behavior
Noise-Induced Cochlear Neuronal Degeneration and Its Role in Hyperacusis- and Tinnitus-Like Behavior by Ann E. Hickox B.A. French Arizona State University, 2006 MSc Speech and Hearing Sciences University College London, 2007 SUBMITTED TO THE HARVARD-MIT DIVISION OF HEALTH SCIENCES AND TECHNOLOGY IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF DOCTOR OF PHILOSOPHY IN SPEECH AND HEARING BIOSCIENCE AND TECHNOLOGY AT THE MASSACHUSETTS INSTITUTE OF TECHNOLOGY FEBRUARY 2013 @2013 Ann E. Hickox. All rights reserved The author hereby grants to MIT permission to reproduce and to distribute publicly paper and electronic copies of this thesis document in whole or in part in any medium now known or hereafter created. Signature of Author: Ann E. Hickox Harvard-MIT Division of e lthSciences and Technology f/ / I / January 2, 2013 Certified by: M. Charles Liberman, Ph.D. Thesis Supervisor Director, Eaton-Peabody Laboratory, Massachusetts Eye & Ear Infirmary Harold F. Schuknecht Professor of Otology and Laryngology, Harvard Medical School Accepted by Emery Brown, MD, PhD Director, Harvard-MIT Division of Health Sciences and Technology Professor of Computational Neuroscience and Health Sciences and Technology 1 2 Noise-Induced Cochlear Neuronal Degeneration and Its Role in Hyperacusis- and Tinnitus-Like Behavior by Ann E. Hickox Submitted to the Harvard-MIT Division of Health Sciences and Technology on January 2, 2013 in partial fulfillment of the requirements for the Degree of Doctor of Philosophy in Speech and Hearing Bioscience and Technology Abstract Perceptual abnormalities such as hyperacusis and tinnitus often occur following acoustic overexposure. Although such exposure can also result in permanent threshold elevation, some individuals with noise-induced hyperacusis or tinnitus show clinically normal thresholds. -

Acoustic Trauma and Hyperbaric Oxygen Treatment
Acoustic Trauma and Hyperbaric Oxygen Treatment Mesut MUTLUOGLU Department of Underwater and Hyperbaric Medicine Gulhane Military Medical Academy Haydarpasa Teaching Hospital 34668, Uskudar, Istanbul TURKEY [email protected] ABSTRACT As stated in the conclusions of the HFM-192 report on hyperbaric oxygen therapy (HBOT) in military medical setting, acoustic trauma is a frequent consequence of military activity in operation. Acoustic trauma refers to an acute hearing loss following a single sudden and very intense noise exposure. It differs from chronic noise induced hearing (NIHL) loss in that it is usually unilateral and causes sudden profound hearing loss. Acoustic trauma is a type of sensorineural hearing loss affecting inner ear structures; particularly the inner and outer hair cells of the organ of Corti within the cochlea. Exposure to noise levels above 85 decibel (dB) may cause hearing loss. While long-term exposure to repetitive or continuous noise above 85 dB may cause chronic NIHL, a single exposure above 130-140 dB, as observed in acoustic trauma, may cause acute NIHL. The loudest sound a human ear may tolerate without pain varies individually, but is usually around 120dB. Military personnel are especially at increased risk for acoustic trauma due to fire arm use in the battle zone. While a machine gun generates around 145dB sound, a rifle generates 157- 163dB, a 105 mm towed howitzer 183dB and an improvised explosive device around 180dB sound. Acoustic trauma displays a gradually down-slopping pattern in the audiogram, particularly after 3000Hz and is therefore described as high-frequency hearing loss. Tinnitus is almost always associated with acoustic trauma. -

Hearing Loss, Vertigo and Tinnitus
HEARING LOSS, VERTIGO AND TINNITUS Jonathan Lara, DO April 29, 2012 Hearing Loss Facts S Men are more likely to experience hearing loss than women. S Approximately 17 percent (36 million) of American adults report some degree of hearing loss. S About 2 to 3 out of every 1,000 children in the United States are born deaf or hard-of-hearing. S Nine out of every 10 children who are born deaf are born to parents who can hear. Hearing Loss Facts S The NIDCD estimates that approximately 15 percent (26 million) of Americans between the ages of 20 and 69 have high frequency hearing loss due to exposure to loud sounds or noise at work or in leisure activities. S Only 1 out of 5 people who could benefit from a hearing aid actually wears one. S Three out of 4 children experience ear infection (otitis media) by the time they are 3 years old. Hearing Loss Facts S There is a strong relationship between age and reported hearing loss: 18 percent of American adults 45-64 years old, 30 percent of adults 65-74 years old, and 47 percent of adults 75 years old or older have a hearing impairment. S Roughly 25 million Americans have experienced tinnitus. S Approximately 4,000 new cases of sudden deafness occur each year in the United States. Hearing Loss Facts S Approximately 615,000 individuals have been diagnosed with Ménière's disease in the United States. Another 45,500 are newly diagnosed each year. S One out of every 100,000 individuals per year develops an acoustic neurinoma (vestibular schwannoma). -

Tinnitus & Hyperacusis
REFERENCE Tinnitus & Hyperacusis GlossarY The American Tinnitus Association (ATA) is pleased to provide our readers with a glossary of terms pertaining to tinnitus and hyperacusis. It has been adapted with permission from a document published with the Progressive Tinnitus Management program developed by researchers and clinicians at the Veterans Health Administration. The ATA Tinnitus & Hyperacusis Glossary was edited by members of the Tinnitus Today Editorial Advisory Panel. The terminology used to describe any condition is of vital importance to diagnosis and treatment of the condition. Without a commonly understood set of terms, we could not effectively communicate a diagnosis, direct treatment for conditions, or expect patients to understand and follow those treatments accurately. www.ATA.org TINNITUS TODay WIntER 2017 33 REFERENCE Acceptance and Commitment aminoglycoside antibiotics: Any by neural networks that respond to Therapy (ACT): A psychotherapeutic of a group of antibiotics derived from different levels of sound. approach similar to Cognitive Behav- various species of Streptomyces that auditory hallucinations: Usually ioral Therapy (CBT), and sometimes is inhibit bacterial protein synthesis and perceived as voices or music (and referenced as part of the third wave of are active against gram-negative bac- sometimes as environmental sounds, CBT approaches. ACT involves mind- teria, in particular. Aminoglycosides e.g., a barking dog), and have been fulness, which is aimed at reducing include streptomycin, gentamicin, studied primarily in the context of psychological distress, depressive amikacin, kanamycin, tobramycin, and mental health. Some individuals who symptoms, and anxiety by focusing on neomycin, among others. All can be experience auditory hallucinations do the present moment. -

Sports Injuries
Sports Injuries Of the Ear G.A.WAGNER,MD SUMMARY The author describes common sports injuries involving the ear. Such injuries include hematoma, lacerations, foreign bodies (tattoo), and thermal injuries. Ear canal injuries include swimmer's ear and penetrating injuries. Tympanum injuries include tympanic membrane perforations, ossicular discontinuity, eustachian tube dysfunction, temporal bone fractures and traumatic facial nerve palsy. Inner ear injuries include traumatic sensorineural deafness. The author emphasizes the management of these injuries. Dr. Wagner, an otolaryngologist, is on the active staff of three Calgary hospitals. SPORTS INJURIES to the ear are as variable as the frostbite. These are usually found in skiers, skaters, and activities which cause them - they may involve the mountain climbers. Severe, deep frostbite injuries of the auricle, external auditory canal, tympanum, and inner ear, auricle are best treated by rapid rewarming with water- but only rarely involve the eighth cranial nerve or central soaked pledgets maintained at between 38 and 42 degrees auditory pathways. centigrade. Freezing, thawing, and re-freezing must be avoided since this is extremely injurious to tissue.2 Surgical Auricle debridement may occasionally be required but is generally Auricle injuries are common, as there is a human reflex prohibited for several months as the auricle has an amazing tendency to turn the head to the side when expecting capacity for self repair. frontal head trauma. The auricle is thereby involved even though the impact may have been from a head-on External Auditory Canal direction.' Lacerations in the ear canal, if minor, may be treated The so-called 'cauliflower ear' often seen in retired with an antibiotic-steroid eardrop solution in order to boxers or wrestlers is caused by untreated - or repeated - minimize crusting, maximize clot dissolution and cleansing hematomas of the auricle. -

EXAMINATION of PATIENTS with ACUTE ACOUSTIC TRAUMA Umar B
EXAMINATION OF PATIENTS WITH ACUTE ACOUSTIC TRAUMA Umar B. Bobodzhanov, Jamol I. Kholmatov, Ravshan U. Bobodzhonov Department of Otorhinolaryngology of the Tajik Medical University of the name Abuali ibni Sino Corresponding author: Jamal I. Kholmatov, Department of Otorhinolaryngology of the Tajik Medical University of the name Abuali ibni Sino, e-mail: [email protected] Abstract The acute acoustic trauma leads to further injuries of various structures of the middle and inner ear. Complex audiological examination of hearing in order to reveal posttraumatic sensorineural hearing loss and timely rehabilitation is required to re- veal injuries. It is especially necessary in case of suspicion of integrity damage of labyrinthine windows. In order to evaluate posttraumatic hearing loss, we consider complete audiological examination, including audiomentry in the expanded range of frequencies of air-conduction and bone-conduction, and also urgent rehabilitation actions necessary. Background All patients with ear trauma reported decrease of hear- ing and tinnitus in the ears which was perceptible from According to different authors ear traumas make 32–70% the moment of trauma. The majority of patients suffered of all injuries both in war and a peace times. Decrease of from abrupt hearing loss. the tinnitus was of various in- their number is hard to estimate in the near future be- tensity and character. cause of constant development of manufacture, increase of speed, instability of living standards and growth of house- Other implications of diseases were noted, such as pain hold violence [1,3,6–8]. and feeling of heaviness in the injured ear. 98 (32.7%) pa- tients noted a short-term loss of consciousness immediate- Occurring diagnostic difficulties, especially in cases of ly after trauma, later on they experienced dizziness, nausea polytrauma of various ear structures and posttraumat- and vomiting.