Report of Inquest Act Respecting the Determination of the Causes and Circumstances of Death
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Premières Nations Et Inuits Du Québec 84 ° 82° 80° 78° 76° 74° 72° 70° 68° 66° 64° 62° 60° 58° 56° 54° 52° 62°
PREMIÈRES NATIONS ET INUITS DU QUÉBEC 84 ° 82° 80° 78° 76° 74° 72° 70° 68° 66° 64° 62° 60° 58° 56° 54° 52° 62° Ivujivik nations Salluit Détroit d’Hudson Abénaquis Kangiqsujuaq les 11 Algonquins Akulivik Attikameks 60° Quaqtaq Cris Mer du Labrador Hurons-Wendats Puvirnituq Kangirsuk Innus (Montagnais) Baie d’Ungava Malécites Micmacs Aupaluk Mohawks Inukjuak Naskapis 58 ° Kangiqsualujjuaq Tasiujaq Inuits T ra cé * Inuits de Chisasibi Kuujjuaq d e 1 9 2 7 d u C o n s Baie d’Hudson e i l p r Umiujaq i v 56 ° é ( n o n d é n i t 10 i f ) Kuujjuarapik Whapmagoostui Kawawachikamach Matimekosh • 54 ° Lac-John Chisasibi Schefferville * Radisson • Happy Valley-Goose Bay • Wemindji Baie James Fermont • 52 ° Eastmain Tracé de 1927 du Conseil privé (non dénitif) Lourdes-de-Blanc-Sablon• Waskaganish Nemaska Pakuashipi 09 Havre- La Romaine Uashat Saint-Pierre 50 ° Maliotenam Nutashkuan Natashquan Mistissini Mingan • Sept-Îles• • • Chibougamau Port-Cartier • Oujé-Bougoumou Waswanipi Île d'Anticosti Pikogan Baie-Comeau 02 • Pessamit Rouyn-Noranda Obedjiwan •Dolbeau-Mistassini Gespeg • • Gaspé 48 ° Val-d’Or Forestville Fleuve Saint-Laurent • Lac-Simon • • Gesgapegiag 11 Alma Essipit • Rimouski Golfe du Saint-Laurent Timiskaming Mashteuiatsh Saguenay• 08 01 Listuguj Kitcisakik Tadoussac• Cacouna Winneway Wemotaci • Whitworth Rivière- Lac-Rapide 04 •La Tuque du-Loup Hunter’s Point 03 Manawan Wendake Kebaowek Route 15 • Québec Voie ferrée 46 ° 07 14 Trois-Rivières Kitigan Zibi • Wôlinak 12 Région administrative Frontière internationale 17 Kanesatake Odanak -

North American Megadam Resistance Alliance
North American Megadam Resistance Alliance May 18, 2020 Christopher Lawrence U.S. Department of Energy Management and Program Analyst Transmission Permitting and Technical Assistance Office of Electricity Christopher.Lawrence.hq.doe.gov Re: Comments on DOE Docket No. PP-362-1: Champlain Hudson Power Express, Inc. and CHPE, LLC: Application to Rescind Presidential Permit and Application for Presidential Permit Dear Mr. Lawrence, The Sierra Club Atlantic Chapter and North American Megadam Resistance Alliance submit these comments on the above-referenced application of Champlain Hudson Power Express, Inc. (CHPEI) and CHPE, LLC (together, the Applicants) to transfer to CHPE, LLC ownership of the facilities owned by CHPEI and authorized for cross-border electric power transmission via a high voltage direct current line (the Project) by Presidential Permit No. PP- 362, dated October 6, 2014 (PP-362 or the Permit) .1 The Project is being developed by TDI, a Blackstone portfolio company. www.transmissiondevelopers.com Blackstone is a private investment firm with about $500 billion under management. www.blackstone.com The Sierra Club Atlantic Chapter, headquartered Albany New York, is responsible for the Sierra Club’s membership and activities in New York State and works on a variety of environmental issues. The Sierra Club is a national environmental organization founded in 1892. 1 On April 6, 2020, the Applicants requested that the Department of Energy (DOE) amend, or in the alternative, rescind and reissue PP-362 to enable the transfer of the Permit from CHPEI to its affiliate CHPE, LLC (the Application). On April 16, 2020, the Department of Energy (DOE) issued a Notice of “Application to Rescind Presidential Permit; Application for Presidential Permit; Champlain Hudson Power Express, Inc. -

Rapport Rectoverso
HOWSE MINERALS LIMITED HOWSE PROJECT ENVIRONMENTAL IMPACT STATEMENT – (APRIL 2016) - SUBMITTED TO THE CEAA 11 LITERATURE CITED AND PERSONAL COMMUNICATIONS Personal Communications André, D., Environmental Coordinator, MLJ, September 24 2014 Bouchard, J., Sécurité du Québec Director, Schefferville, September 26 2014 Cloutier, P., physician in NNK, NIMLJ and Schefferville, September 24 2014 Coggan, C. Atmacinta, Economy and Employment – NNK, 2013 and 2014 (for validation) Corbeil, G., NNK Public Works, October 28 2014 Cordova, O., TSH Director, November 3 2014 Côté, S.D., Localization of George River Caribou Herd Radio-Collared Individuals, Map dating from 2014- 12-08 from Caribou Ungava Einish, L., Centre de la petite enfance Uatikuss, September 23 2015 Elders, NNK, September 26 2014 Elders, NIMLJ, September 25 2014 Fortin, C., Caribou data, December 15 2014 and January 22 2014 Gaudreault, D., Nurse at the CLSC Naskapi, September 25 2014 Guanish, G., NNK Environmental Coordinator, September 22 2014 ITUM, Louis (Sylvestre) Mackenzie family trapline holder, 207 ITUM, Jean-Marie Mackenzie family, trapline holder, 211 Jean-Hairet, T., Nurse at the dispensary of Matimekush, personal communication, September 26 2014 Jean-Pierre, D., School Principal, MLJ, September 24 2014 Joncas, P., Administrator, Schefferville, September 22 2014 Lalonde, D., AECOM Project Manager, Environment, Montreal, November 10 2015 Lévesque, S., Non-Aboriginal harvester, Schefferville, September 25 2014 Lavoie, V., Director, Société de développement économique montagnaise, November 3 2014 Mackenzie, M., Chief, ITUM, November 3 2014 MacKenzie, R., Chief, Matimekush Lac-John, September 23 and 24 2014 Malec, M., ITUM Police Force, November 5 2014 Martin, D., Naskapi Police Force Chief, September 25 2014 Michel, A. -
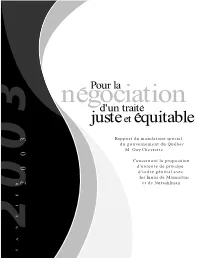
Justeet Equitable
Pour la negociationd'un traite juste et equitable Rapport du mandataire spécial du gouvernement du Québec M. Guy Chevrette Concernant la proposition d'entente de principe d'ordre général avec les Innus de Mamuitun 2003 et de Nutashkuan JANVIER Pour la négociation d'un traité juste et équitable Table des matières 1. PRÉAMBULE. 5 2. LES GRANDS CONSTATS . 7 3. LES TERRITOIRES EN CAUSE ET LES PRINCIPES ET MODALITÉS QUI S’Y APPLIQUERAIENT. 11 3.1 Le Nitassinan. 11 3.1.1 La propriété . 11 3.1.2 L’étendue. 11 3.1.3 Les activités traditionnelles de chasse, de pêche, de trappe et de cueillette (Innu Aitun) . 12 3.1.4 La participation au développement. 14 a) Forêt, mines et pourvoiries. 14 b) Parcs, réserve faunique et aires d’aménagement et de développement. 15 3.1.5 La participation aux processus gouvernementaux de la gestion du territoire . 16 3.1.6 Les redevances. 16 3.2 L’Innu Assi . 16 3.2.1 L’autonomie gouvernementale. 17 3.2.2 L’autonomie financière. 17 3.2.3 Les droits des tiers sur l’Innu Assi . 18 3.2.4 Les cas particuliers de Nutashkuan et d’Essipit . 19 4. LE PROCESSUS DE NÉGOCIATION ET AUTRES CONSIDÉRATIONS . 21 4.1 La participation au processus de négociation et d’information. 21 4.2 La participation aux processus postnégociation . 22 4.3 Le cas de Sept-Îles et de Uashat-Maliotenam . 22 4.4 La clause concernant la Constitution de 1982 . 22 4.5 Référendum ou consultation . 23 CONCLUSION . 25 RECOMMANDATIONS . 27 ANNEXES A. -

Tipatshimun 2E Trimestre 2008 .Pdf
MAI-JUIN 2008 VOLUME 5 NUMÉRO 2 P. 8 L’aire de répartition du caribou des bois ne cesse de reculer vers le nord, à tel point que cette espèce n’existe pratiquement plus au sud du St-Laurent, si ce n’est dans le Parc de la Gaspésie. Mais le caribou ne s’en va pas : il meurt! P. 10 Benjamin Ross, Pierre Ross-Fortin et Pierre-Marc Gravel représentaient Essipit à la quatrième Le Centre d’information et de réservations édition de la Dictée innu / Pakunu e mashinaitshenanut qui, comme chaque année, avait lieu à des Entreprises Essipit a remporté l’or, soit un Uashat. Pierre-Marc et Benjamin ont décroché respectivement la première et deuxième place premier prix national dans la catégorie dans la catégorie innue langue seconde. Une fierté qui rejaillit sur toute la Première Nation « services touristiques », à l’occasion des plus récents Grands Prix du tourisme québécois d’Essipit. P. 5 tenus au Palais des congrès de Montréal. Tipatshimun ENSEMBLE VERS UN TRAITÉ Une obligation de résultat serait appelé à trancher à titre C’est à l’occasion de propriétaire foncier. « de rencontres d’échange et d’informa- Autre question : où les tion tenues les 4 et 5 mai municipalités trouveront-elles derniers, que les mem- de meilleurs alliés pour les bres, membres apparen- aider à mettre en place leur tés et employés d’Essipit, propre plan d’aménagement, ont posé une foule de tel que stipulé dans le Livre questions et formulé vert? Essipit y travaille pour leurs commentaires en sa part depuis plus de cinq regard de la conduite ans! Au lieu de s’affronter sur des négociations et plus un sujet aussi vital pour notre particulièrement en ce région, c’est ensemble, Innus qui a trait au régime et Québécois réunis, que nous territorial. -

Community Development in English-Speaking Communities in Québec: Lessons Learned from a Participatory Action Research Project
Community development in English-speaking communities in Québec: lessons learned from a participatory action research project INSTITUT NATIONAL DE SANTÉ PUBLIQUE DU QUÉBEC Community development in English-speaking communities in Québec: lessons learned from a participatory action research project Développement des individus et des communautés January 2014 AUTHORS Mary Richardson, PhD, Anthropologist Institut national de santé publique du Québec Shirley Jobson, research professional Institut national de santé publique du Québec Joëlle Gauvin-Racine, research professional Institut national de santé publique du Québec REVIEW COMMITTEE Cheryl Gosselin, Professor Bishop’s University Jennifer Johnson, Executive Director Community Health and Social Services Network Kit Malo Centre for Community Organizations Lorraine O’Donnell Québec English-Speaking Communities Research Network (Concordia University and Canadian Institute for Research on Linguistic Minorities) Louis Poirier, Chef d’unité Institut national de santé publique du Québec Paule Simard, Chercheure Institut national de santé publique du Québec Normand Trempe, Project coordinator Institut national de santé publique du Québec ACKNOWLEDGEMENTS This project was instigated by the Community Health and Social Services Network (CHSSN) and received financial support from Health Canada. We also wish to acknowledge the valuable comments and suggestions made by the review committee. Ce document est disponible intégralement en format électronique (PDF) sur le site Web de l’Institut national de santé publique du Québec au : http://www.inspq.qc.ca. Les reproductions à des fins d’étude privée ou de recherche sont autorisées en vertu de l’article 29 de la Loi sur le droit d’auteur. Toute autre utilisation doit faire l’objet d’une autorisation du gouvernement du Québec qui détient les droits exclusifs de propriété intellectuelle sur ce document. -

Duplessis Manicouagan
renseignements utiles SYMBOLES ET PICTOGRAMMES CARTE DE LA RÉGION TOURISTIQUE CÔTE-NORD Légende Matimekosh – Schefferville Kawawachikamach Lac-John (accessible par train à partir de Sept-Îles) Municipalité SYMBOLES Réserve autochtone Happy Valley- Route Goose Bay ET PICTOGRAMMES Chemin de fer Churchill Falls Route des Baleines Æ Abri pour Circuit gourmand ? Lieux d’accueil ¶ Restauration Village-relais pique-nique à Chasse saisonnier Route verte Traversier h Aire de ö Location U Chute ¶! Petit-déjeuner Trajet du N/M Bella-Desgagnés Labrador City Km 362 pique-nique d’équipement Emeril Junction LABRADOR ¢ Cuisinette ¶@ Dîner Aéroport Wabush Accès Internet w Location de chalet c Cuisine commune ¶# Souper Lieu d’accueil saisonnier sans fil gratuit L Location de vélo Fermont s Électricité , Salle de bains Lieu d’accueil permanent < Aéroport - Hôpital t Ornithologie privée M Agréé Bienvenue 30 ampères F Minifrigo b Parc et réserve naturelle Km 473 Procurez-vous la Carte touristique cyclistes u 50 ampères Salle de bains Fire Lake Blanc-Sablon p.82 n Motoneige partagée Parc marin du Saguenay – de la Côte-Nord dans nos bureaux R i v Bonne-Espérance v Saint-Laurent Fermont et i D Air climatisé Entrée directe d’information touristique (p. 218 à 220). è p.50 r e Blanc- la Route 389 S Brador @ Pêche º Salle de gym a i n Middle Bay Sablon t -  A Animaux admis Entrée gratuite u Rivière-Saint-Paul g u C s t Î a h Pêche blanche Ski alpin i n e m Lourdes-de- i Apportez votre vin $ Entrée payante n Vieux-Fort Blanc-Sablon d St. -

Testimony of Chief Rene Simon Pessamit Lnnu First Nation Pessamit, Canada July 20, 2017 Ladies and Gentlemen of the State Of
Testimony of Chief Rene Simon Pessamit lnnu First Nation Pessamit, Canada July 20, 2017 Ladies and gentlemen of the State of New Hampshire Site Evaluation Committee, my name is Paul Pouliot. I am the Sag8mo of the Cowasuck Band of the Pennacook Abenaki People, based in Alton, NH. Chief Rene Simon and the elected officials of Pessamit have asked me to deliver this message and thank you for the opportunity to speak at the Northern Pass public hearings. It is with confidence in a better future that the "Pessamit lnnu First Nation" is addressing you today. It is not Pessamit's intention to take a position on the impacts of the Northern Pass Project in New Hampshire. However, we want to share our experience with regard to the source of electricity and its environmental and social legitimacy. In 1973, the Supreme Court of Canada confirmed our Ancestral Rights, territories and the value of the Indigenous treaties with France and England . However, the Quebec Government challenged the Supreme Court's decision until1996 when the Supreme Court ruled against Quebec's position. ,.. ,~. 1 N~'TP(;5E. rvniV The Government of Quebec strategically allowed enough time fo completion of Hydro-Quebec, a government owned entity, to invade our Nitassina our homelands. As such, thirteen hydroelectric plants and eleven re~ were implanted on our homelands without impact studies, without our consent and without compensation. This state-run fraud now makes 29% of Hydro-Quebec's installed capacity which is illegally acquired at the expense of Pessamit. The Government of Quebec, which is Hydro-Quebec's sole shareholder, has become one of the largest and most profitable energy companies in the West. -

Continuation of the Negotiations with the Innu
QUEBECERS and the INNU CONTINUATION OF THE NEGOTIATIONS WITH THE INNU AGREEMENT-IN-PRINCIPLE WORKING TOGETHER TO ACHIEVE A TREATY Québec Secrétariat aux affaires autochtones Québec HOW TO PARTICIPATE IN THE NEGOTIATIONS The Government of Québec has put in place a participation mechanism that allows the populations of the Saguenay–Lac-Saint-Jean and Côte-Nord regions to make known their opinion at the negotiating table. Québec’s negotiations team includes a representative of the regions who attends all of the negotiation sessions. He is the regions’ spokesperson at the negotiating table. The representative of the regions can count on the assistance of one delegate in each of the regions in question. W HAT IS THE RO L E OF THE REP RES ENTATIV E O F THE REGIO NS AND THE DELEGATES? 1 To keep you informed of the progress made in the work of the negotiating table. 2 To consult you and obtain your comments. 3 To convey your proposals and concerns to the Minister for Aboriginal Affairs and to the special negotiator for the Government of Québec. WHAT IS THE AGREEM ENT-IN-P RINCIPLE? The agreement-in-principle reached by the Government of Québec, the Government of Canada and the First Nations of Betsiamites, Essipit, Mashteuiatsh and Nutashkuan will serve as a basis for negotiating a final agreement that will compromise a treaty and complementary agreements. In other words, it is a framework that will orient the pursuit of negotiations towards a treaty over the next two years. WHY NEGOTIATE? Quebecers and the Innu have lived together on the same territory for 400 years without ever deciding on the aboriginal rights of the Innu. -

Schéma De Couverture De Risque En Sécurité Incendie
Schéma de couverture de risques en sécurité incendie Municipalité régionale de comté de Sept-Rivières DÉCEMBRE 2009 MRC de Sept-Rivières Schéma de couverture de risques en sécurité incendie Préparé par : Marie-Claude Dubé Sarah Daragon Chargées de projet en sécurité incendie Dépôt du projet pour consultation le 16 octobre 2007 Dépôt du projet pour approbation du ministre le 15 janvier 2008 Adoption du schéma le 15 décembre 2009 Entrée en vigueur du schéma le 4 janvier 2010 Collaborateurs Conseil de la MRC : o Laurence Méthot, préfet et mairesse de la Ville de Port-Cartier o Henriette Lapierre, représentante de la Ville de Port-Cartier o Serge Lévesque, maire de la Ville de Sept-Îles Comité de Sécurité Incendie : o Guy Bonin, représentant du Service incendie de Port-Cartier o Gervais Gagné, conseiller de la Ville de Sept-Îles o Gaby Gauthier, conseiller de la Ville de Sept-Îles o Denis Jutras, représentant du service incendie de Sept-Îles o Alain Lapierre, directeur général de la MRC o Henriette Lapierre, conseillère de la Ville de Port-Cartier Comité technique du schéma de couverture de risques : o Guy Bonin, représentant du service incendie de Port-Cartier o Andrée Bouffard, directrice générale de la Ville de Port-Cartier o Claude Bureau, directeur général de la Ville de Sept-Îles o Patrick Gagnon, représentant du service incendie de Sept-Îles Ministère de la Sécurité publique : o Claude Labrie, conseiller en sécurité incendie Chargée de projet : o Marie-Claude Dubé, inspectrice régionale, MRC de Sept-Rivières Anciens collaborateurs -

Principaux Dossiers Et Décisions
Numéro 1 14 matishu-pishimu | février 2014 Kuei! Pekuakamiulnuatsh Takuhikan instaure aujourd’hui une nouvelle action de communication importante destinée à informer rapidement la population des principales décisions et dossiers traités par les élus, et ce, conformément aux orientations et priorités du Conseil visant à rendre compte aux Pekuakamiulnuatsh des décisions et enjeux majeurs. Dorénavant, nous publierons de façon régulière le présent feuillet préparé par notre nouveau Secteur des communications. Nous souhaitons que cet outil vous permette de bien suivre les travaux et d’être impliqués dans la poursuite des objectifs et priorités de votre Conseil. Gilbert Dominique Pekuakamiu ilnutshimau | Chef des Pekuakamiulnuatsh Principaux dossiers et décisions Participation à la création d’un fonds pour soutenir la logement sur la rue Atshikash, dont la réalisation est mise en place d’une structure politique de la nation conditionnelle à l’obtention de la totalité du innue en y injectant un montant de 3 000 $. financement. Chaque communauté de la nation innue fournit le Résolution pour la poursuite du partenariat avec les même montant. MRC dans les activités de Forêt modèle du Lac- Choix du secteur Duteau pour la récolte de Saint-Jean, pour investir la somme de 60 000 $ 50 000 m3 de bois en 2014. annuellement jusqu’au 31 mars 2017 et pour désigner Suzanne Dupuis et Steve Morel à titre de Suspension temporaire du processus d’embauche représentants au conseil d’administration. des postes de directeur principal des affaires communautaires et de directeur principal de la Résolution pour proclamer officiellement la troisième culture et du développement durable afin de semaine de février comme Journées de la simplifier la mise en place de la nouvelle structure persévérance scolaire à Mashteuiatsh. -

Spring Survey of Caribou in the Vicinity of Schefferville May 2009
SPRING SURVEY OF CARIBOU IN THE VICINITY OF SCHEFFERVILLE MAY 2009 Prepared for: NEW MILLENNIUM CAPITAL CORP. AND LABRADOR IRON MINES LIMITED FINAL REPORT – WITHOUT PREJUDICE Natalie D’Astous, Groupe Hémisphères Perry Trimper, Jacques Whitford Stantec Limited November 2009 EXECUTIVE SUMMARY During May 2009, Labrador Iron Mines Limited and New Millennium Capital Corp. partnered to complete an aerial survey for caribou in consultation with the Newfoundland and Labrador Wildlife Division. Both companies are undergoing environmental reviews for mining projects located in the vicinity of Schefferville, Quebec. Working under the regulatory direction of the Provincial Wildlife Division in Newfoundland and Labrador and the ministère des Ressources naturelles et de la Faune du Quebec, consultants for these proponents (i.e., Jacques Whitford Stantec Limited (JWSL) and Groupe Hémisphères (GH), respectively) worked together to assess the presence/absence of sedentary caribou in the area surrounding these proposed iron ore developments. The survey was a requirement of the Newfoundland and Labrador environmental assessment process. Prior to field investigations, a literature search was conducted to identify a Study Area of 50 km in radius centred on each proposed development. Letters explaining the objectives and other aspects of the survey were sent to the leaders of the local First Nations concerned, namely the Innu Nation, Innu Takuaikan Uashat mak Mani-Utenam, the Naskapi Nation of Kawawachikamach and the Nation Innu Matimekush-Lac John. Given the presence of staging waterfowl, a portion of Attikamagen and Petitsikapau Lakes was avoided to reduce potential effects on the goose hunting activities being conducted at the time, at the request of these leaders.