Gluten Food Frequency Questionnaire
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Autumn Conference Proceedings 2015 British Society of Baking
2FWREHU $XWXPQ&RQIHUHQFH 3URFHHGLQJV %ULWLVK6RFLHW\RI%DNLQJ $IILOLDWHGWRWKH$PHULFDQ6RFLHW\RI%DNLQJ %ULWLVK6RFLHW\RI%DNLQJ $XWXPQ&RQIHUHQFH %LFHVWHU+RWHO*ROIDQG6SD2[IRUGVKLUH 7XHVGD\WKDQG:HGQHVGD\WK2FWREHU 3DSHU 6SHDNHU 3DJH 7KH%6%²3DVW3UHVHQWDQG)XWXUH -LP%URZQ 3DXO7XUQHU 3 0LNH%DJVKDZ 0D[LPLVLQJ%XVLQHVVDQG+XPDQ3RWHQWLDO 'DYLG6PDUW 8 :DVWH0DQDJHPHQWLQ)RRG0DQXIDFWXUH &DPSEHOO0XUUD\ 13 7KH&XUUHQW8.(FRQRPLF&OLPDWHIRU%XVLQHVV 'DQLHO/HH 19 7KH%,$5LVLQJ6WDU$ZDUG 1DWKDQ*LOHV 23 )UHHIURP'HYHORSPHQW %DNHU\3URGXFW,QQRYDWLRQ&KULV%URFNPDQ 27 7KH9LOODJH%DNHU\·V7UDLQLQJDQG,QQRYDWLRQ$FDGHP\5RELQ-RQHV 32 7KH6HFUHWDU\ %ULWLVK6RFLHW\RI%DNLQJ 9LQH&RWWDJH7RPSNLQV/DQH0DUVK*LEERQ %LFHVWHU2[RQ2;(; 7HO)D[(PDLOEVE#IUHHXNFRP 1 7+(%5,7,6+62&,(7<2)%$.,1* $IILOLDWHGWRWKH$PHULFDQ6RFLHW\RI%DNLQJ ([HFXWLYH&RPPLWWHH 0LNH%DJVKDZ &KDLUPDQ %ULDQ&ODUNH 3DXO7XUQHU 9LFH&KDLUPDQ 5LFKDUG+D]HOGLQH -LP%URZQ +RQ7UHDVXUHU 6\OYLD0DFGRQDOG &RQIHUHQFH&RRUGLQDWRU *RUGRQ3ROVRQ 6KDURQ%\UQH 6HFUHWDU\ -DQH7\OHU 6DUD$XWWRQ ,PPHGLDWH3DVW&KDLUPDQ 3DXO:HVWRQ 6DUD3ULHVWOH\ 6WXGHQW/LDLVRQ 0DLO&KLPS 0DUN<RXQJ 3DVW&KDLUPHQ -7KRPVRQ $%XFKDQDQ 5)HUJXVRQ +&ROERXUQH )(OOLV 3+H\JDWH )%DWHV *3ULQFH 6&DXYDLQ $+DOO 32UW 10HDGRZV -6WHYHQV '5REHUWV &/RPD[ 36KHQWRQ 51HZVWHDG 1-DFNVRQ *+XPSKUH\ 70RVV $03ROODUG :*XQVWRQH 'U3:RRG .+RXOLVWRQ '.LQJ 30DVVH\ 6$XWWRQ 5+DUH $:DWHUILHOG 7%HDOH $+RGJHV 5+XPSKUH\ -%URZQ -5LWFKLH 3:DUG 5+RUQVE\ -53DUNLQVRQ -$QWKRQ\ ,0HOOLQJ *9HUH .6KDZ '*DUUDWW 56LPPV )6D\HU *&ULWLFRV )(OOLV 30RUURZ 5)OLQW 5.LUN .6\GQH\ -*ULHYHV 3DVWQG9LFH&KDLUPHQ EHIRUHWKHQG9LFH&KDLUPDQGLGQRWSURFHHGWR VW9LFH&KDLUPDQDQG&KDLUPDQEHFDXVHKHGLGQRWZRUNIRUDEDNHU\FRPSDQ\ 36DYRU\ 57XUQHU *%UXFH .0RUJDQ -0DKOLFK .&ROOLQJH **LOEHUW 1'RXJODV 7&ROOLQV -3ULFH 6/DPEHUW -%URZQ 1%HVVDQW -+X[WDEOH ::DOODFH 56DQGHUVRQ :3ULQJOH *6FKLQGOHU -3HONPDQ '(OLDV &&XUWLV ,.LQJ .:LOOLDPVRQ -3ULQJOH &%UDFHZHOO -*UHHQILHOG 2 Paul Turner; and to then look to the future with Chairman Mike 2015 DIAMOND JUBILEE AUTUMN Bagshaw. -

Food First Advice for Adults with a Small Appetite 2021
Food first Advice for adults with a small appetite Why have I received this handout? You may have a poor appetite or have been eating less due to feeling unwell. If you are not getting enough nutrition to meet your body’s needs you will lose weight and could be at risk of malnutrition. Malnutrition makes it more difficult for the body to fight illness and infection. It can make us feel weak, tired and low in mood. To treat malnutrition we need to increase the energy or calories, protein and overall nutrients that we eat and drink. This handout provides advice on increasing your intake using ordinary foods and by making simple changes to your meals, snacks and drinks. Although some of the foods and drinks in this leaflet may usually be considered unhealthy, they are recommended until your appetite and weight improve. These foods are energy-dense and can help to reduce your risk of malnutrition. If you have diabetes, it is preferable to fortify your food with protein and fats rather adding extra sugar or including more sugary foods. This will help to minimise the impact on your blood glucose levels. If you normally check your blood glucose levels and further to making these dietary changes find that they are higher than your target range, please contact your GP or diabetes nurse for advice regarding your diabetes management. Please read our food first diabetes leaflet for more information. Helpful tips 1 Try eating little and often. 2 Aim for 3 small meals and 2 to 3 snacks between meals. -
Of 4 07/12/2015
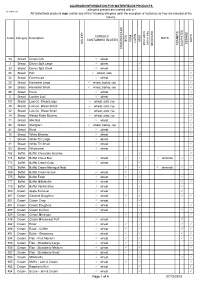
ALLERGEN INFORMATION FOR WATERFIELDS PRODUCTS - allergens present are marked with a NETHERTON All Waterfields products may contain any of the following allergens (with the exception of molluscs) as they are handled at the bakery. CEREALS Code Category Description NUTS CONTAINING GLUTEN EGG FISH MILK SOYA LUPIN CELERY SESAME (not on site) PEANUTS MOLLUSCS MUSTARD SULPHITES CRUSTACEANS 34 Bread Crown Cob wheat 3 Bread Devon Split Large wheat 33 Bread Devon Split Small wheat 85 Bread Farl wheat, oats 32 Bread Farmhouse wheat 20 Bread Harvester Large wheat, barley, rye 84 Bread Harvester Small wheat, barley, rye 86 Bread Hovis wheat 2 Bread London Loaf wheat 107 Bread Low G.I. Bread Large wheat, oats, rye 48 Bread Low G.I. Bread Sliced wheat, oats, rye 42 Bread Low G.I. Bread Small wheat, oats, rye 14 Bread Malted Flake Bloomer wheat, oats, rye 71 Bread Milk Roll wheat 88 Bread Multigrain wheat, barley, rye 41 Bread Rural wheat 16 Bread White Bloomer wheat 1 Bread White Tin Large wheat 31 Bread White Tin Small wheat 53 Bread Wholemeal wheat 782 Buffet Buffet Chocolate Surprise 774 Buffet Buffet Choux Bun wheat almonds 773 Buffet Buffet Cream Crisp wheat 778 Buffet Buffet Cream Meringue Nest almonds 786 Buffet Buffet Cream Scone wheat 775 Buffet Buffet Éclair wheat 777 Buffet Buffet Millefeuille wheat 776 Buffet Buffet Vanilla Slice wheat 500 Cream Apple Turnover wheat 467 Cream Caramel Doughnut wheat 501 Cream Cream Crisp wheat 481 Cream Cream Doughnut -

William Schwenck Gilbert - Poems
Classic Poetry Series William Schwenck Gilbert - poems - Publication Date: 2004 Publisher: Poemhunter.com - The World's Poetry Archive William Schwenck Gilbert(1836 - 1911) William Schwenck Gilbert, born in London in 1836, was the son of a retired naval surgeon. Except for a kidnapping by Italian brigands in Italy at age two, and a ransomed release, he appears to have had a very normal upbringing. Beyond ordinary schooling, he took training as an artillery officer and was tutored in military science with hopes of participating in the Crimean War. Unfortunately for him, but not for us, he did not graduate until after the War was over. Gilbert subsequently joined the militia and was a member for 20 years. After finishing his military training Gilbert worked in a government bureau job which he hated. Upon receiving a nice inheritance from an aunt, Gilbert indulged his fancy and became a barrister. Called to the bar at age 28, Gilbert's law career, with no "rich attorney's elderly, ugly daughter" to help him escape mediocrity, lasted just a few years. Before leaving his law practice, however, he married the daughter of an army officer. Gilbert had shown a proclivity for caustic wit and sarcasm from an early age and it was this talent that put him on the path to greatness. Beginning in 1861, Gilbert contributed dramatic criticism and humorous verse (unsigned) to the popular British magazine FUN. Some of his work was accompanied by cartoons and sketches which were signed "Bab." Many of the characters in the G&S operas were modelled after some of Gilbert's "Bab" characters. -

Unit: 01 Basic Ingredients
Bakery Management BHM –704DT UNIT: 01 BASIC INGREDIENTS STRUCTURE 1.1 Introduction 1.2 Objectives 1.3 Sugar 1.4 Shortenings 1.5 Eggs 1.6 Wheat and flours 1.7 Milk and milk products 1.8 Yeast 1.9 Chemical leavening agents 1.10 Salt 1.11 Spices 1.12 Flavorings 1.13 Cocoa and Chocolate 1.14 Fruits and Nuts 1.15 Professional bakery equipment and tools 1.16 Production Factors 1.17 Staling and Spoilage 1.18 Summary 1.19 Glossary 1.20 Reference/Bibliography 1.21 Suggested Readings 1.22 Terminal Questions 1.1 INTRODUCTION Bakery ingredients have been used since ancient times and are of utmost importance these days as perhaps nothing can be baked without them. They are available in wide varieties and their preferences may vary according to the regional demands. Easy access of global information and exposure of various bakery products has increased the demand for bakery ingredients. Baking ingredients offer several advantages such as reduced costs, volume enhancement, better texture, colour, and flavour enhancement. For example, ingredients such enzymes improve protein solubility and reduce bitterness in end products, making enzymes one of the most preferred ingredients in the baking industry. Every ingredient in a recipe has a specific purpose. It's also important to know how to mix or combine the ingredients properly, which is why baking is sometimes referred to as a science. There are reactions in baking that are critical to a recipe turning out correctly. Even some small amount of variation can dramatically change the result. Whether its breads or cake, each ingredient plays a part. -

Raisins & Dried Fruits
Sun-Maid Raisins & Dried Fruits One hundred years in the making, Sun-Maid’s century of experience answers all your questions on raisins and dried fruits—their unique characteristics, their history, and how they are grown, processed, Raisins & Dried Fruits marketed, and enjoyed throughout the world. Serving American Families & the World Since 1912 & the World Since 1912 Serving American Families $35.00 USA Printed in U.S.A Raisins & Dried Fruits Serving American Families & the World Since 1912 Sun-Maid growers Of California Sun-Maid creative teaM Anna L. Palecek • gary H. Marshburn • Barry f. Kriebel 13525 South Bethel avenue Kingsburg, Ca 93631-9232 Tel: 1-559-896-8000 Email: [email protected] Website: www.sunmaid.com Special thanks to Jerry Winters, cover design Copyright © 2011 Sun-Maid Growers of California Raisins & Dried Fruits Serving American Families & the World Since 1912 LONDON, NEW YORK, MUNICH, MELBOURNE, DELHI FOR DORLING KINDERSLEY: Managing Art Editor RichaRd czapnik Senior Editors Michele Wells, ROs WALFORd • DTP Designers david McDonald, kavita VARMa • Senior Production Controller saRah hughes Associate Publisher nigel duffield FirstFOR published DORLING in the United KINDERSLEY States in December 2011 by DK Publishing, 375 Hudson Street, New York, New York 10014 Managing Art10 Editor 9 8 7 6 5 4 Richard 3 2 1 Czapnik Senior Editors Michele001-182142-Dec/11 Wells, ROS WALFORD Copyright Page Layout and Design © 2011 Dorling Kindersley Limited DTP Designers David McDonald, Kavita VARMA All rights reserved under International and Pan-American Copyright Conventions. No part of Seniorthis publication Production may be reproduced, Controller stored in a retrieval Sarah system, HughEs or transmitted in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise,Associate without the priorPublisher written permission Nigel of Duffield the copyright owner. -
Project No: V5va 1040
PROJECT NO: V5VA 1040 Steviol Glycosides Exposure Assessment Author: Phil Northing The Food and Environment Research Agency Sand Hutton York YO41 1LZ Sponsor: Coca-Cola Europe Start Date: June 2010 End Date: September 2010 Report Issue Date: September 2010 Pages in Report: 91 Final Report: 29th September 2010 Contents 1. Assessment Objectives ..................................................................................................................... 3 2. Model Specification ......................................................................................................................... 3 3. Food Baskets .................................................................................................................................... 3 4. Maximum Level data ....................................................................................................................... 5 5. Associations ..................................................................................................................................... 5 6. Modelling Approach ........................................................................................................................ 7 7. Exposure Results .............................................................................................................................. 8 8. Conclusions .................................................................................................................................... 12 9. References ..................................................................................................................................... -
Carbohydrate Counting – Food Reference Lists
Carbohydrate counting – food reference lists UHB is a no smoking Trust Please note This list has been compiled using a sample of foods and is not as accurate as the information detailed on the packaging for specific foods. • Wt (g) refers to the the weight of food • CHO (g) refers to the carbohydrate content within the specified weight For ease of calculation, carbohydrate contents have been listed to the nearest 5g. This information is intended only for those people with diabetes on a basal bolus, multiple daily injection (MDI) or pump insulin regimes that are able to carbohydrate count and self-adjust insulin doses. If you have type 1 diabetes we recommend you book a place on either the Dose Adjustment For Normal Eating (DAFNE) or Heart of England Type 1 Education (HET1E) course. 2 | PI20_1167_03 Carbohydrate counting - Food reference lists Biscuits Food Quantity Wt (g) CHO (g) Blue Ribband 1 12.9g 10 Blue Ribband dark 1 11.8g 10 Bourbon cream 1 12g 10 Chocolate digestive 1 18g 10 Cream crackers 2 14g 10 Custard cream 1 11g 10 Digestive 1 13g 10 Digestive creams 1 8.3g 10 Digestive fingers 2 10.2g 10 Fig roll 1 12g 10 Flapjack 1 large 90g 55 Fox’s Classics 1 15.7g 15 Fox’s Creams (vanilla cream) 2 15.2g 10 Frusli Bar 1 30g 20 Giant chocolate chip cookie 1 large cookie 65g 65 Ginger snap 1 10g 10 HobNobs 1 13g 10 Jaffa cake 1 10g 10 Kit Kat (2 finger) 1 22g 15 Malted Milk 2 18g 10 Mini Cheddars 1 mini pack 25g 15 Nutrigrain Bar 1 37g 25 Oatcake 1 12g 10 Penguin 1 14g 15 Rich Tea 2 12g 10 Ritz (plain) 5 15g 10 Rocky 1 12.7g 15 PI20_1167_03 -
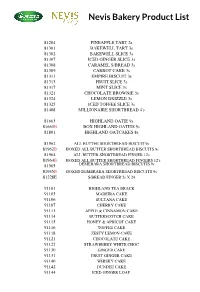
Bakery-Product-List-EDITED.Pdf
Nevis Bakery Product List 81204 PINEAPPLE TART 2s 81301 BAKEWELL TART 3s 81302 BAKEWELL SLICE 3s 81307 ICED GINGER SLICE 3s 81308 CARAMEL S/BREAD 3s 81309 CARROT CAKE 3s 81311 EMPIRE BISCUIT 3s 81313 FRUIT SLICE 3s 81317 MINT SLICE 3s 81321 CHOCOLATE BROWNIE 3s 81324 LEMON DRIZZLE 3s 81325 ICED TOFFEE SLICE 3s 81408 MILLIONAIRE SHORTBREAD 4's 81663 HIGHLAND OATIE 9s 81663B BOX HIGHLAND OATIES 9s 81801 HIGHLAND OATCAKES 8s 81962 ALL BUTTER SHORTBREAD BISCUIT 9s 81962B BOXED ALL BUTTER SHORTBREAD BISCUITS 9s 81964 ALL BUTTER SHORTBREAD FINGER 12s 81964B BOXED ALL BUTTER SHORTBREAD FINGERS 12's 81965 DEMERARA SHORTBREAD BISCUITS 9s 81965B BOXED DEMERARA SHORTBREAD BISCUITS 9s 81228E S/BREAD FINGER 2s X 24 91101 HIGHLAND TEA BRACK 91105 MADEIRA CAKE 91106 SULTANA CAKE 91107 CHERRY CAKE 91113 APPLE & CINNAMON CAKE 91114 BUTTERSCOTCH CAKE 91115 HONEY & APRICOT CAKE 91116 TOFFEE CAKE 91118 ZESTY LEMON CAKE 91121 CHOCOLATE CAKE 91122 STRAWBERRY WHITE CHOC 91130 GINGER CAKE 91131 FRUIT GINGER CAKE 91140 WHISKY CAKE 91142 DUNDEE CAKE 91144 ICED GINGER LOAF Macleans Bakery Product List TUES THUR FRI CODE DESCRIPTION MON ____ WED ____ SAT ____ ____ ____ ____ 1026 GI BREAD 400G SLICED 1027 GI FLAT TOP 800G SLICED 1035 WHITE BREAD 800G SLICED 1038 BROWN BREAD 800G SLICED 1109 WASTLE WHITE 1116 WASTLE BROWN 1118 WASTLE GI 1194 WHITE ROLLS LOOSE 1224 WHITE ROLLS X4 1202 SOFTIES LOOSE 1232 SOFTIES X4 1135 GI ROLLS LOOSE 1235 GI ROLLS X4 1219 BROWN ROLL LOOSE 1229 BROWN ROLLS X4 1203 BUTTERIES LOOSE 1230 BUTTERIES X4 1320 PANCAKES X4 1319 MUFFINS X4 1295 -

Allergen Information for Waterfields Products
ALLERGEN INFORMATION FOR WATERFIELDS PRODUCTS - allergens present are marked with a All Waterfields products may contain any of the following allergens (with the exception of molluscs) as they are handled at the bakery. Code Category Description EGG FISH MILK NUTS SOYA LUPIN CELERY SESAME CEREALS PEANUTS MUSTARD SULPHITES CRUSTACEANS CONTAINING GLUTEN MOLLUSCS (not on site) MOLLUSCS (not on 34 Bread Crown Cob Small wheat 3 Bread Devon Split Large wheat 33 Bread Devon Split Small wheat 85 Bread Farl (4) wheat, oats 32 Bread Farmhouse Small wheat 57 Bread Flatbread - Tomato & Mozzarella wheat, rye, barley 23 Bread Focaccia - Lancashire Cheese & Red Onion wheat, rye, barley 58 Bread Focaccia - Mature Cheddar & Red Onion wheat, rye, barley 22 Bread Focaccia - Rosemary wheat, rye, barley 20 Bread Harvester Large wheat, rye, barley 84 Bread Harvester Small wheat, barley, rye 79 Bread Hot Cross Bun Loaf wheat 86 Bread Hovis wheat 107 Bread Large G.I Loaf wheat, oats, rye 1 Bread Large White Tin wheat 2 Bread London Loaf Large wheat 42 Bread Low G.I. Bread wheat, rye, oats 14 Bread Malted Flake Bloomer Bread wheat, rye, oats 30 Bread Malted Wholegrain Thicker Sliced wheat, rye 71 Bread Milk Roll wheat 88 Bread Multigrain wheat, barley, rye 1878 Bread Paninni Part Baked (20) wheat, rye, barley 41 Bread Rural Small wheat 74 Bread Sandwich Bread - Fruited wheat 24 Bread Sandwich Bread - G.I wheat, rye 27 Bread Sandwich Bread - Harvester wheat, rye, barley 19 Bread Sandwich Bread - Multigrain Thicker Sliced wheat, rye, barley 26 Bread Sandwich Bread - Multigrain Thicker Sliced wheat, rye, barley 25 Bread Sandwich Bread White wheat 53 Bread Stoneground Small wheat Page 1 18/03/2015 ALLERGEN INFORMATION FOR WATERFIELDS PRODUCTS - allergens present are marked with a All Waterfields products may contain any of the following allergens (with the exception of molluscs) as they are handled at the bakery. -
Allergen Main List1
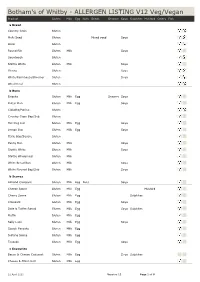
Botham's of Whitby - ALLERGEN LISTING V12 Veg/Vegan Product Gluten Milk Egg Nuts Seeds Sesame Soya Sulphites Mustard Celery Fish a Bread Country Grain Gluten Multi Seed Gluten Mixed seed Soya Oatie Gluten Round Rib Gluten Milk Soya Sourdough Gluten Stottie White Gluten Milk Soya Vienna Gluten Soya White/Farmhouse/Bloomer Gluten Soya Wholemeal Gluten b Buns Brioche Gluten Milk Egg SesameSoya Butter Bun Gluten MilkEgg Soya Ciabatta/Panino Gluten Country Grain Bap/Sub Gluten Hot Dog Roll Gluten MilkEgg Soya Lemon Bun Gluten MilkEgg Soya Oatie Bap/Square Gluten Penny Bun Gluten Milk Soya Stottie White Gluten Milk Soya Stottie Wholemeal Gluten Milk White Bread Bun Gluten Milk Soya White Floured Bap/Sub Gluten Milk Soya b Scones Almond Croissant Gluten Milk Egg Nuts Soya Cheese Scone Gluten MilkEgg Mustard Cherry Scone Gluten Milk Egg Sulphites Croissant Gluten MilkEgg Soya Date & Toffee Rascal Gluten Milk Egg Soya Sulphites Muffin Gluten Milk Egg Sally Lunn Gluten MilkEgg Soya Scotch Pancake Gluten Milk Egg Sultana Scone Gluten Milk Egg Teacake Gluten MilkEgg Soya c Savouries Bacon & Cheese Croissant Gluten Milk Egg Soya Sulphites Cheese & Onion Roll Gluten Milk Egg 22 April 2021 Version 12 Page 1 of 9 Product Gluten Milk Egg Nuts Seeds Sesame Soya Sulphites Mustard Celery Fish Chicken & Ham Pie Gluten Milk Egg Soya Celery Chicken & Leek Pie Gluten Milk Egg Soya Celery Minced Steak & Onion Pie Gluten Milk Egg Soya Sulphites Celery Pizza Cheese & Tomato Gluten Milk Pizza Ham & Pineapple Gluten Milk Pork Pie Gluten Milk Egg Quiche Cheese & Onion -

Price List Bread Plate Pies
PRICE LIST BREAD PLATE PIES Medium White Barm…………..……..…………..……....48p Chicken & Mushroom Pie 9”……………..……..….£6.90 Medium Harvester Barm....………………..…..……....48p Potato & Meat Pie 9”……………..…………….………£6.90 White Bloomer 400g……………………………...…….£1.95 Steak Pie Large 9"…………………….………………….£6.90 Harvester Bloomer 400g………….……………..……£2.05 THICK & THIN SLICING AVAILABLE. QUICHE Hot Cross bun…………………………………………………...50p Flavours, Mushroom, Ham & Tomato or Goats Cheese and Spinach. Croissant…………………………………………………………£1.05 Quiche Large 9"……………………….....................£20.70 Danish Pastry…………………………………………………£1.55 Quiche Small 6"……………………………………….....£8.40 SAVOURIES Quiche Individual………………………………..…....….£2.60 Beef Pie……….………………………….………………..….£2.10 Pork Pie……………………………………………….………..£2.10 FAMILY MEALS Pork & Black pudding pie……………………………...£2.15 Cornish Roll…………………………………………...….....£3.20 Hot Pot (per Portion)…………………………….......£4.85* Sausage Roll…………………………………….……..…….£2.00 Meat Lasagne (per Portion)………………....…...£4.80* Pork & Apple Roll…………………………….……....…..£2.05 Veg Lasagne (per Portion)…………………...….....£4.70* Spiced Chutney Sausage Roll………………..……....£2.05 In Individual portions , 2 portions or 6 portions. Subject to availability. Cheese & Bacon T/over………………………...…..….£2.35 Cheese & Onion Pasty……………………..…….….....£2.20 Savoury items are all available to buy Pizza Slice………………………………………..……...…….£2.25 frozen to bake at home. Spinach & Cheese Roll………………….………....…...£2.00 Potato Cake…………………………..……………...…..….£1.05 SUNDRIES Potato Cake Large, Bacon, Cheese & Tomato…£2.60 Potato