Radiation Therapy
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

*Revelle, Roger Baltimore 18, Maryland
NATIONAL ACADEMY OF SCIENCES July 1, 1962 OFFICERS Term expires President-Frederick Seitz June 30, 1966 Vice President-J. A. Stratton June 30, 1965 Home Secretary-Hugh L. Dryden June 30, 1963 Foreign Secretary-Harrison Brown June 30, 1966 Treasurer-L. V. Berkner June 30, 1964 Executive Officer Business Manager S. D. Cornell G. D. Meid COUNCIL *Berkner L. V. (1964) *Revelle, Roger (1965) *Brown, Harrison (1966) *Seitz, Frederick (1966) *Dryden, Hugh L. (1963) *Stratton, J. A. (1965) Hutchinson, G. Evelyn (1963) Williams, Robley C. (1963) *Kistiakowsky, G. B. (1964) Wood, W. Barry, Jr. (1965) Raper, Kenneth B. (1964) MEMBERS The number in parentheses, following year of election, indicates the Section to which the member belongs, as follows: (1) Mathematics (8) Zoology and Anatomy (2) Astronomy (9) Physiology (3) Physics (10) Pathology and Microbiology (4) Engineering (11) Anthropology (5) Chemistry (12) Psychology (6) Geology (13) Geophysics (7) Botany (14) Biochemistry Abbot, Charles Greeley, 1915 (2), Smithsonian Institution, Washington 25, D. C. Abelson, Philip Hauge, 1959 (6), Geophysical Laboratory, Carnegie Institution of Washington, 2801 Upton Street, N. W., Washington 8, D. C. Adams, Leason Heberling, 1943 (13), Institute of Geophysics, University of Cali- fornia, Los Angeles 24, California Adams, Roger, 1929 (5), Department of Chemistry and Chemical Engineering, University of Illinois, Urbana, Illinois Ahlfors, Lars Valerian, 1953 (1), Department of Mathematics, Harvard University, 2 Divinity Avenue, Cambridge 38, Massachusetts Albert, Abraham Adrian, 1943 (1), 111 Eckhart Hall, University of Chicago, 1118 East 58th Street, Chicago 37, Illinois Albright, William Foxwell, 1955 (11), Oriental Seminary, Johns Hopkins University, Baltimore 18, Maryland * Members of the Executive Committee of the Council of the Academy. -

Sterns Lebensdaten Und Chronologie Seines Wirkens
Sterns Lebensdaten und Chronologie seines Wirkens Diese Chronologie von Otto Sterns Wirken basiert auf folgenden Quellen: 1. Otto Sterns selbst verfassten Lebensläufen, 2. Sterns Briefen und Sterns Publikationen, 3. Sterns Reisepässen 4. Sterns Züricher Interview 1961 5. Dokumenten der Hochschularchive (17.2.1888 bis 17.8.1969) 1888 Geb. 17.2.1888 als Otto Stern in Sohrau/Oberschlesien In allen Lebensläufen und Dokumenten findet man immer nur den VornamenOt- to. Im polizeilichen Führungszeugnis ausgestellt am 12.7.1912 vom königlichen Polizeipräsidium Abt. IV in Breslau wird bei Stern ebenfalls nur der Vorname Otto erwähnt. Nur im Emeritierungsdokument des Carnegie Institutes of Tech- nology wird ein zweiter Vorname Otto M. Stern erwähnt. Vater: Mühlenbesitzer Oskar Stern (*1850–1919) und Mutter Eugenie Stern geb. Rosenthal (*1863–1907) Nach Angabe von Diana Templeton-Killan, der Enkeltochter von Berta Kamm und somit Großnichte von Otto Stern (E-Mail vom 3.12.2015 an Horst Schmidt- Böcking) war Ottos Großvater Abraham Stern. Abraham hatte 5 Kinder mit seiner ersten Frau Nanni Freund. Nanni starb kurz nach der Geburt des fünften Kindes. Bald danach heiratete Abraham Berta Ben- der, mit der er 6 weitere Kinder hatte. Ottos Vater Oskar war das dritte Kind von Berta. Abraham und Nannis erstes Kind war Heinrich Stern (1833–1908). Heinrich hatte 4 Kinder. Das erste Kind war Richard Stern (1865–1911), der Toni Asch © Springer-Verlag GmbH Deutschland 2018 325 H. Schmidt-Böcking, A. Templeton, W. Trageser (Hrsg.), Otto Sterns gesammelte Briefe – Band 1, https://doi.org/10.1007/978-3-662-55735-8 326 Sterns Lebensdaten und Chronologie seines Wirkens heiratete. -
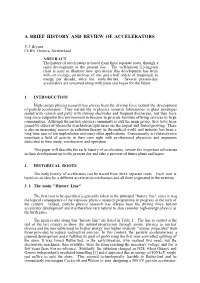
A Brief History and Review of Accelerators
A BRIEF HISTORY AND REVIEW OF ACCELERATORS P.J. Bryant CERN, Geneva, Switzerland ABSTRACT The history of accelerators is traced from three separate roots, through a rapid development to the present day. The well-known Livingston chart is used to illustrate how spectacular this development has been with, on average, an increase of one and a half orders of magnitude in energy per decade, since the early thirties. Several present-day accelerators are reviewed along with plans and hopes for the future. 1 . INTRODUCTION High-energy physics research has always been the driving force behind the development of particle accelerators. They started life in physics research laboratories in glass envelopes sealed with varnish and putty with shining electrodes and frequent discharges, but they have long since outgrown this environment to become large-scale facilities offering services to large communities. Although the particle physics community is still the main group, they have been joined by others of whom the synchrotron light users are the largest and fastest growing. There is also an increasing interest in radiation therapy in the medical world and industry has been a long-time user of ion implantation and many other applications. Consequently accelerators now constitute a field of activity in their own right with professional physicists and engineers dedicated to their study, construction and operation. This paper will describe the early history of accelerators, review the important milestones in their development up to the present day and take a preview of future plans and hopes. 2 . HISTORICAL ROOTS The early history of accelerators can be traced from three separate roots. -

Physiker-Entdeckungen Und Erdzeiten Hans Ulrich Stalder 31.1.2019
Physiker-Entdeckungen und Erdzeiten Hans Ulrich Stalder 31.1.2019 Haftungsausschluss / Disclaimer / Hyperlinks Für fehlerhafte Angaben und deren Folgen kann weder eine juristische Verantwortung noch irgendeine Haftung übernommen werden. Änderungen vorbehalten. Ich distanziere mich hiermit ausdrücklich von allen Inhalten aller verlinkten Seiten und mache mir diese Inhalte nicht zu eigen. Erdzeiten Erdzeit beginnt vor x-Millionen Jahren Quartär 2,588 Neogen 23,03 (erste Menschen vor zirka 4 Millionen Jahren) Paläogen 66 Kreide 145 (Dinosaurier) Jura 201,3 Trias 252,2 Perm 298,9 Karbon 358,9 Devon 419,2 Silur 443,4 Ordovizium 485,4 Kambrium 541 Ediacarium 635 Cryogenium 850 Tonium 1000 Stenium 1200 Ectasium 1400 Calymmium 1600 Statherium 1800 Orosirium 2050 Rhyacium 2300 Siderium 2500 Physiker Entdeckungen Jahr 0800 v. Chr.: Den Babyloniern sind Sonnenfinsterniszyklen mit der Sarosperiode (rund 18 Jahre) bekannt. Jahr 0580 v. Chr.: Die Erde wird nach einer Theorie von Anaximander als Kugel beschrieben. Jahr 0550 v. Chr.: Die Entdeckung von ganzzahligen Frequenzverhältnissen bei konsonanten Klängen (Pythagoras in der Schmiede) führt zur ersten überlieferten und zutreffenden quantitativen Beschreibung eines physikalischen Sachverhalts. © Hans Ulrich Stalder, Switzerland Jahr 0500 v. Chr.: Demokrit postuliert, dass die Natur aus Atomen zusammengesetzt sei. Jahr 0450 v. Chr.: Vier-Elemente-Lehre von Empedokles. Jahr 0300 v. Chr.: Euklid begründet anhand der Reflexion die geometrische Optik. Jahr 0265 v. Chr.: Zum ersten Mal wird die Theorie des Heliozentrischen Weltbildes mit geometrischen Berechnungen von Aristarchos von Samos belegt. Jahr 0250 v. Chr.: Archimedes entdeckt das Hebelgesetz und die statische Auftriebskraft in Flüssigkeiten, Archimedisches Prinzip. Jahr 0240 v. Chr.: Eratosthenes bestimmt den Erdumfang mit einer Gradmessung zwischen Alexandria und Syene. -

National Academy of Sciences July 1, 1973
NATIONAL ACADEMY OF SCIENCES JULY 1, 1973 OFFICERS Term expires President-PHILIP HANDLER June 30, 1975 Vice-President-SAUNDERS MAC LANE June 30, 1977 Home Secretary-ALLEN V. ASTIN June 30, 1975 Foreign Secretary-HARRISON BROWN June 30, 1974 Treasurer- E. R. PIORE June 30, 1976 Executive Officer Comptroller John S. Coleman Aaron Rosenthal Buiness Manager Bernard L. Kropp COUNCIL *Astin, Allen V. (1975) Marshak, Robert E. (1974) Babcock, Horace W. (1976) McCarty, Maclyn (1976) Bloch, Konrad E. (1974) Pierce, John R. (1974) Branscomb, Lewis M. (1975) *Piore, E. R. (1976) *Brown, Harrison (1974) Pitzer, Kenneth S. (1976) *Cloud, Preston (1975) *Shull, Harrison (1974) Eagle, Harry (1975) Westheimer, Frank H. (1975) *Handler, Philip (1975) Williams, Carroll M. (1976) *Mac Lane, Saunders (1977) * Members of the Executive Committee of the Council of the Academy. SECTIONS The Academy is divided into the following Sections, to which members are assigned at their own choice: (1) Mathematics (10) Microbiology (2) Astronomy (11) Anthropology (3) Physics (12) Psychology (4) Engineering (13) Geophysics (5) Chemistry (14) Biochemistry (6) Geology (15) Applied Biology (7) Botany (16) Applied Physical and Mathematical Sciences (8) Zoology (17) Medical Sciences (9) Physiology (18) Genetics (19) Social, Economic, and Political Sciences In the alphabetical list of members, the number in parentheses, following year of election, indicates the Section to WCiph the member belongs. 3009 Downloaded by guest on September 25, 2021 3010 Members N.A.S. Organization CLASSES Ames, Bruce Nathan, 1972 (14), Department of Biochem- istry, University of California, Berkeley, California The members of Sections are grouped in the following Classes: 94720 Anderson, Carl David, 1938 (3), California Institute of I. -
Radioactivity and X-Rays
Radioactivity and X-rays Applications and health effects by Thormod Henriksen Preface The present book is an update and extension of three previous books from groups of scientists at the University of Oslo. The books are: I. Radioaktivitet – Stråling – Helse Written by; Thormod Henriksen, Finn Ingebretsen, Anders Storruste and Erling Stranden. Universitetsforlaget AS 1987 ISBN 82-00-03339-2 I would like to thank my coauthors for all discussions and for all the data used in this book. The book was released only a few months after the Chernobyl accident. II. Stråling og Helse Written by Thormod Henriksen, Finn Ingebretsen, Anders Storruste, Terje Strand, Tove Svendby and Per Wethe. Institute of Physics, University of Oslo 1993 and 1995 ISBN 82-992073-2-0 This book was an update of the book above. It has been used in several courses at The University of Oslo. Furthermore, the book was again up- dated in 1998 and published on the Internet. The address is: www.afl.hitos.no/mfysikk/rad/straling_innh.htm III. Radiation and Health Written by Thormod Henriksen and H. David Maillie Taylor & Francis 2003 ISBN 0-415-27162-2 This English written book was mainly a translation from the books above. I would like to take this opportunity to thank David for all help with the translation. The three books concentrated to a large extent on the basic properties of ionizing radiation. Efforts were made to describe the background ra- diation as well as the release of radioactivity from reactor accidents and fallout from nuclear explosions in the atmosphere. These subjects were of high interest in the aftermath of the Chernobyl accident. -

Lawrence Berkeley National Laboratory Recent Work
Lawrence Berkeley National Laboratory Recent Work Title BIBLIOGRAPHY OF PARTICLE ACCELERATORS - JULY 1948 to DEC. 1950 Permalink https://escholarship.org/uc/item/0m72734s Author Cushman, Bonnie E. Publication Date 1951-03-01 eScholarship.org Powered by the California Digital Library University of California UCRL 1238 cy 2 r UNIVERSITY OF CALIFORNIA TWO-WEEK LOAN COpy This is a Library Circulating Copy which may be borrowed for two weeks. For a personal retention copy, call Tech. Info. Division, Ext. 5545 . BERKELEY, CALIFORNIA DISCLAIMER This document was prepared as an account of work sponsored by the United States Government. While this document is believed to contain correct information, neither the United States Government nor any agency thereof, nor the Regents of the University of California, nor any of their employees, makes any warranty, express or implied, or assumes any legal responsibility for the accuracy, completeness, or usefulness of any information, apparatus, product, or process disclosed, or represents that its use would not infringe privately owned rights. Reference herein to any specific commercial product, process, or service by its trade name, trademark, manufacturer, or otherwise, does not necessarily constitute or imply its endorsement, recommendation, or favoring by the United States Government or any agency thereof, or the Regents of the University of California. The views and opinions of authors expressed herein do not necessarily state or reflect those of the United States Government or any agency thereof or the Regents of the University of California. l1JNClASSIFHEJ" UCRL-1238 Unclassified - Physics Distribution UNIVERSITY OF CALIFORNIA . , Radiation laboratory Contract No o ~v-7405-eng-48 BIBLIOGRAPHY OF PARTICLE ACGELERATORS JULY 1948 TO DECEMBER 1950 Bonnie E. -

*Revelle, Roger
NATIONAL ACADEMY OF SCIENCES July 1, 1964 OFFICERS Term expires President-Frederick Seitz June 30, 1966 Vice President-J. A. Stratton June 30, 1965 Home Secretary-Hugh L. Dryden June 30, 1967 Foreign Secretary-Harrison Brown June 30, 1966 Treasurer-L. V. Berkner June 30, 1968 Executive Officer Business Manager S. D. Cornell G. D. Meid COUNCIL *Berkner, L. V. (1968) *Seitz, Frederick (1966) *Brown, Harrison (1966) Sonneborn, T. M. (1966) *Dryden, Hugh L. (1967) *Stratton, J. A. (1965) Kornberg, Arthur (1966) Weiss, Paul (1967) *Pitzer, K. S. (1967) Wood, W. Barry, Jr. (1965) *Revelle, Roger (1965) MEMBERS The number in parentheses, following year of election, indicates the Section to which the member belongs, as follows: (1) Mathematics (8) Zoology and Anatomy (2) Astronomy (9) Physiology (3) Physics (10) Pathology and Microbiology (4) Engineering (11) Anthropology (5) Chemistry (12) Psychology (6) Geology (13) Geophysics (7) Botany (14) Biochemistry Abbot, Charles Greeley, 1915 (2), Smithsonian Institution, Washington, D. C. 20560 Abelson, Philip Hauge, 1959 (6), Geophysical Laboratory, Carnegie Institution of Washington, 2801 Upton Street, N. W., Washington, D. C. 20008 Adams, Leason Heberling, 1943 (13), Institute of Geophysics, University of Cali- fornia, Los Angeles, California 90024 Adams, Roger, 1929 (5), Department of Chemistry and Chemical Engineering, University of Illinois, Urbana, Illinois 61803 AhIfors, Lars Valerian, 1953 (1), Department of Mathematics, Harvard University, 2 Divinity Avenue, Cambridge, Massachusetts 02138 Albert, Abraham Adrian, 1943 (1), 111 Eckhart Hall, University of Chicago, 1118 East 58th Street, Chicago, Illinois 60637 Albright, William Foxwell, 1955 (11), Oriental Seminary, Johns Hopkins University, Baltimore, Maryland 21218 * Members of the Executive Committee of the Council of the Academy. -

The Betatron and Its Applications
THE BETATRON AND ITS APPLICATIONS A THESIS Presented to the Faculty of the Division of Graduate Studies Georgia Institute of Technology In Partial Fulfillment of the Requirements for the Degree Master of Science in Physics by Walter Wilkinson Atkins June 1951 Original Page Numbering Retained. THE BETATRON AND ITS APPLICATIONS Approved: / Date Approved by Chairman ) o / ACKNOWLEDGMENTS I should like to express my sincere appreciation to Dr. J. E. Boyd, my advisor, for his aid and guidance during the course of this work. Also, I should like to thank Dr. V. D. Crawford for his assist- ance in the preparation of specific sections, and to Dr. L. D. Wyly and Dr. W. M. Spicer for their constructive suggestions. I should like to thank the staff of the library of the Georgia Institute of Technology, especially Miss Harris and Mrs. Jackson, for their co—operation and help in the location of reference material. Without the assistance of Miss Mildred Jordan of the Emory University Medical Library, sections of this thesis could not have been written. iv TABLE OF CONTENTS CHAPTER PAGE I. INTRODUCTION 1 II. ELECTRON ACCELERATION 10 III.MECHANICS OF THE BETATRON 29 IV. BETATRON INSTALLATION 70 V. PHYSICAL APPLICATIONS 81 VI. RADIOGRAPHY IVITH THE BETATRON 116 VII.MEDICAL APPLICATIONS 123 BIBLIOGRAPHY 138 APPENDIX I: VECTOR NOTATION IN CYLINDRICAL COORDINATES 149 APPENDIX II: DERIVATION OF RELATION BETMEN 150 Br AND Bz APPENDIX III : DERIVATION OF EQUATION /7/ 151 APPENDIX IV: PROOF OF EQUATION /8B/ 152 APPENDIX V: DETERMINATION OF THE RELATIVISTIC MASS EQUATION 153 APPENDIX VI: SIMPLIFICATION OF THE KINETIC ENERGY EQUATION 154 LIST OF FIGURES FIGURES PAGE 1. -
Man-Made Accelerators (Earth-Based)
Man-Made Accelerators (Earth-Based) Ron Ruth SLAC Outline of Talk • Introduction • History of Particle Acceleration • Basic Principles – What are the forces? – Acceleration and radiation – Synchronism – Basic device ideas, linear circular – Beams and physics – Storage ring colliders – Electron Linear Accelerators – The next window: linear colliders • The present generation – Storage Ring Factories –LHC – Linear colliders: ILC • The next generations – Two beam colliders – Laser acceleration – Plasma acceleration – Muon colliders Cosmic Ray Spectrum • OK, OK, so our beam so our energy is a bit lower than yours. • Only TeV scale now. • But we have got you with flux, if not energy. • More on that later. From ‘The Evolution of Particle Accelerators and Colliders’ by Wolfgang K. H. Panofsky “WHEN J. J. THOMSON discovered the electron, he did not call the instrument the was using an accelerator, but an accelerator it certainly was. He accelerated particles between two electrodes to which he had applied a difference in electric potential. He manipulated the resulting beam with electric and magnetic fields to determine the charge-to-mass ratio of cathode rays. Thomson achieved his discovery by studying the properties of the beam itself—not its impact on a target or another beam, as we do today. Accelerators have since become indispensable in the quest to understand Nature at smaller and smaller scales. And although they are much bigger and far more complex, they still operate on much the same physical principles as Thomson’s device.” [1897] Livingston Chart • Graph of concepts • Points are devices • Energy is plotted in terms of the laboratory energy when colliding with a proton at rest to reach the same center of mass energy. -
A Bridge Between
A BRIDGE BETWEEN TWO EPOCHS 2 translation of calligraphy surah of qadr 97 VERILY WE REVEALED IT IN THE NIGHT OF QADR . AND WHAT MAKES YOU KNOW WHAT THE NIGHT OF QADR IS ? THE NIGHT OF QADR IS BETTER THAN A THOUSAND MONTHS . THE ANGELS AND THE SPIRIT DESCEND IN IT BY THE PERMISSION OF THEIR LORD , CONCERNING EVERY WORK . [ IT IS ] PEACE UNTIL THE BREAK OF DAWN . HIS HIGHNESS AGA KHAN III , MOSAIC PORTRAIT IN LAPIS LAZULI ismail gulgee reproduced by kind permission of amin gulgee 4 A BRIDGE BETWEEN TWO EPOCHS CREATIVE DIRECTOR rashida noormohamed-hunzai PHOTOGRAPHS RESEARCHERS nizar habib, yasmin p. karim DESIGNER yasmin p. karim 2 0 1 4 6 A BRIDGE BETWEEN TWO EPOCHS rashida noormohamed-hunzai 8 GLORIOUS LIFE OF HAZRAT MAWLANA SULTAN MUHAMMAD SHAH C - AL-HUSAYNI, ALAYHI’S-SALAM, HIS HIGHNESS AGA KHAN III 04 ABOUT THIS PUBLICATION 12 SAYINGS OF HAZRAT MAWLANA SHAH KARIM AL-HUSAYNI, HIS HIGHNESS AGA KHAN IV, RELATED TO HIS GRANDFATHER 14 HONOURS 26 SPECIAL EVENTS 54 INVENTIONS CONTENTS 70 SAYINGS RELATED TO WOMEN 102 MESSAGES TO THE ISMAILIS OF AFRICA 108 STATUS OF WOMEN 118 THE CONCEPT OF MONOREALITY 132 CORRESPONDENCE 136 PHOTO CREDITS 137 ACKNOWLEDGEMENTS bout his u b l i c a ti o n ABrave indeed wouldT be a person toP undertake a book on Hazrat Mawlana Sultan Muhammad Shah al-Husayni, calayhi’s-salÀm! It would take much more than an ordinary literary talent to do justice to a life crammed with so many unprecedented events and achievements, a life which he himself describes as being so full that he was never for an instant bored! This publication therefore has very different objectives. -
Os Cientistas E O Esforço De Guerra. É Bem Sabido Que, Por Ocasião Dos Conflitos Bélicos, Os Cientistas São Chamados Para O Esforço De Guerra
SEARA DA CIÊNCIA CURIOSIDADES DA FÍSICA José Maria Bassalo Os cientistas e o esforço de guerra. É bem sabido que, por ocasião dos conflitos bélicos, os cientistas são chamados para o esforço de guerra. Muito embora a maioria deles aceite (com o arrependimento de uns poucos), existiram cientistas (também poucos) que se recusaram a trabalhar para projetos bélicos. A seguir, vamos enumerar os principais cientistas que trabalharam nos famosos projetos bélicos criados no decorrer da Segunda Guerra Mundial (1939-1945), da Guerra Fria (intervalo crítico: 1949-1953) e da Guerra do Vietnã (1955-1973), assim como os que se recusaram. [Para detalhes sobre a participação desses cientistas e de outros não referidos, ver os livros (e referências bibliográficas neles anotadas): Danhoni Neves, M. C. 1999. Memórias do Invisível: Uma Reflexão sobre a História no Ensino de Física e a Ética da Ciência, Departamento de Física da Universidade Estadual de Maringá e LCV Edições; Farias, R. F. de, Bassalo, J. M. F. e Ferreira, J. E. Ética e Atividade Científica, a ser publicado pela Editora Átomo, em 2006.] Na Segunda Guerra Mundial, foram desenvolvidos três Projetos Atômicos: Americano, Alemão e Soviético. Vamos enumerar os mais importantes cientistas que trabalharam neles. No Projeto Atômico Americano, conhecido como Projeto Manhattan (PM), destacam-se os seguintes cientistas. Físicos norte- americanos: Luís Walter Alvarez (1911-1988; PNF, 1968), Robert Fox Bacher (1905-2004), Hans Albrecht Bethe (1906-2005; PNF, 1967) (de origem alemã), Felix Bloch (1905-1983;