FORDS for 2011
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Endocrine Surgery Goals and Objectives
Lenox Hill Hospital Department of Surgery Endocrine Surgery Goals and Objectives Medical Knowledge and Patient Care: Residents must demonstrate knowledge and application of the pathophysiology and epidemiology of the diseases listed below for this rotation, with the pertinent clinical and laboratory findings, differential diagnosis and therapeutic options including preventive measures, and procedural knowledge. They must show that they are able to gather accurate and relevant information using medical interviewing, physical examination, appropriate diagnostic workup, and use of information technology. They must be able to synthesize and apply information in the clinical setting to make informed recommendations about preventive, diagnostic and therapeutic options, based on clinical judgement, scientific evidence, and patient preferences. They should be able to prescribe, perform, and interpret surgical procedures listed below for this rotation. All Residents are expected to understand: 1. Normal physiology and anatomy of the thyroid glands. 2. Normal physiology and anatomy of the parathyroid glands. 3. Normal physiology and anatomy of the adrenal glands 4. Normal physiology of the pancreatic neuroendocrine cells. 5. Normal physiology of the pituitary gland. Disease-Based Learning Objectives: Hyperfunctioning Thyroid and Hypothyroid State: 1. Physiology of Grave’s disease and toxic goiter. 2. Management of a patient in hyperthyroid storm. 3. Medical and surgical treatment options for hyperthyroidism. 4. Physiology of Hashimoto’s thyroiditis and hypothyroidism. Thyroid Neoplasm: 1. Workup of a cold thyroid nodule. 2. Surgical management of papillary, follicular, medullary, and anaplastic thyroid carcinoma. 3. Adjuvant therapy for thyroid neoplasms. 4. Postoperative medical management and long-term follow-up of thyroid cancer. Hyperparathyroidism: 1. Diagnosis and work-up of hypercalcemia and primary, secondary, and tertiary hyperparathyroidism. -

Human Anatomy As Related to Tumor Formation Book Four
SEER Program Self Instructional Manual for Cancer Registrars Human Anatomy as Related to Tumor Formation Book Four Second Edition U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutesof Health SEER PROGRAM SELF-INSTRUCTIONAL MANUAL FOR CANCER REGISTRARS Book 4 - Human Anatomy as Related to Tumor Formation Second Edition Prepared by: SEER Program Cancer Statistics Branch National Cancer Institute Editor in Chief: Evelyn M. Shambaugh, M.A., CTR Cancer Statistics Branch National Cancer Institute Assisted by Self-Instructional Manual Committee: Dr. Robert F. Ryan, Emeritus Professor of Surgery Tulane University School of Medicine New Orleans, Louisiana Mildred A. Weiss Los Angeles, California Mary A. Kruse Bethesda, Maryland Jean Cicero, ART, CTR Health Data Systems Professional Services Riverdale, Maryland Pat Kenny Medical Illustrator for Division of Research Services National Institutes of Health CONTENTS BOOK 4: HUMAN ANATOMY AS RELATED TO TUMOR FORMATION Page Section A--Objectives and Content of Book 4 ............................... 1 Section B--Terms Used to Indicate Body Location and Position .................. 5 Section C--The Integumentary System ..................................... 19 Section D--The Lymphatic System ....................................... 51 Section E--The Cardiovascular System ..................................... 97 Section F--The Respiratory System ....................................... 129 Section G--The Digestive System ......................................... 163 Section -

Collaborative Stage Manual Part II
SEER Program Coding and Staging Manual 2004, Revision 1 Collaborative Staging Codes Nasal Cavity C30.0 C30.0 Nasal cavity (excludes nose, NOS C76.0) Note: Laterality must be coded for this site, except subsites Nasal cartilage and Nasal septum, for which laterality is coded 0. CS Tumor Size CS Site-Specific Factor 1 - Size of The following tables are available CS Extension Lymph Nodes at the collaborative staging CS TS/Ext-Eval CS Site-Specific Factor 2 - website: CS Lymph Nodes Extracapsular Extension, Lymph Nodes Histology Exclusion Table CS Reg Nodes Eval for Head and Neck AJCC Stage Reg LN Pos CS Site-Specific Factor 3 - Levels I- Lymph Nodes Size Table Reg LN Exam III, Lymph Nodes for Head and Neck CS Mets at DX CS Site-Specific Factor 4 - Levels IV- CS Mets Eval V and Retropharyngeal Lymph Nodes for Head and Neck CS Site-Specific Factor 5 - Levels VI- VII and Facial Lymph Nodes for Head and Neck CS Site-Specific Factor 6 - Parapharyngeal, Parotid, Preauricular, and Sub-Occipital Lymph Nodes, Lymph Nodes for Head and Neck Nasal Cavity CS Tumor Size SEE STANDARD TABLE Nasal Cavity CS Extension Code Description TNM SS77 SS2000 00 In situ; non-invasive Tis IS IS 10 Invasive tumor confined to site of origin T1 L L Meatus (superior, middle, inferior) Nasal chonchae (superior, middle, inferior) Septum Tympanic membrane 30 Localized, NOS T1 L L 40 Extending to adjacent connective tissue within the nasoethomoidal T2 RE RE complex Nasolacrimal duct 60 Adjacent organs/structures including: T3 RE RE Bone of skull Choana Frontal sinus Hard palate -

Delayed Multiple Port Sites Metastases After Laparoscopic Radical Prostatectomy
CASE REPORT Delayed Multiple Port Sites Metastases After Laparoscopic Radical Prostatectomy Brusabhanu Nayak, MS, MCH, Prem Nath Dogra, MS, MCH, Vaibhav Saxena, MS, MCH, Ashis Saini, MS, MCH Department of Urology, All India Institute of Medical Sciences, New Delhi, India (all authors). ABSTRACT Introduction: Laparoscopic port site metastases are recurrent nodular lesions developing locally in the abdominal wall within the scar tissue of one or more trocar sites. We are reporting an extremely rare case of delayed multiple port site metastases 3 years after laparoscopic radical prostatectomy. In this case, 3 port site metastases appeared 3 years after laparoscopic radical prostatectomy. Case Description: A 65-year-old man was evaluated for lower urinary tract symptoms and found to have raised serum prostate-specific antigen of 9.06 ng/mL. Transrectal ultrasonography-guided biopsy of the prostate revealed an adeno- carcinoma of the prostate (Gleason score 3 ϩ 4 ϭ 7), with 5 of 12 cores positive for tumor. Contrast-enhanced computed tomography showed localized disease with no involvement of seminal vesicle or lymph nodes. The bone scan was normal. He underwent laparoscopic radical prostatectomy for localized carcinoma of the prostate. He developed 3 port site metastases 3 years after surgery. In view of multiple port site metastatic disease, bilateral orchiectomy was done. The patient is doing well after 1 year of follow-up. Conclusion: We report an occurrence of delayed multiple port site metastases after laparoscopic radical prostatectomy. The 3 sites of metastases in our case included the extraction site, the most active instrument site, and the drain placement site. -

Gender Dysphoria Treatment – Commercial Medical Policy
UnitedHealthcare® Commercial Medical Policy Gender Dysphoria Treatment Policy Number: 2021T0580J Effective Date: April 1, 2021 Instructions for Use Table of Contents Page Related Commercial Policies Coverage Rationale ....................................................................... 1 • Blepharoplasty, Blepharoptosis and Brow Ptosis Documentation Requirements ...................................................... 3 Repair Definitions ...................................................................................... 4 • Botulinum Toxins A and B Applicable Codes .......................................................................... 5 • Cosmetic and Reconstructive Procedures Description of Services ................................................................. 9 • Gonadotropin Releasing Hormone Analogs Benefit Considerations .................................................................. 9 Clinical Evidence ......................................................................... 10 • Habilitative Services and Outpatient Rehabilitation U.S. Food and Drug Administration ........................................... 15 Therapy References ................................................................................... 15 • Panniculectomy and Body Contouring Procedures Policy History/Revision Information ........................................... 16 • Rhinoplasty and Other Nasal Surgeries Instructions for Use ..................................................................... 17 Community Plan Policy • Gender Dysphoria -

Surgical Indications and Techniques for Adrenalectomy Review
THE MEDICAL BULLETIN OF SISLI ETFAL HOSPITAL DOI: 10.14744/SEMB.2019.05578 Med Bull Sisli Etfal Hosp 2020;54(1):8–22 Review Surgical Indications and Techniques for Adrenalectomy Mehmet Uludağ,1 Nurcihan Aygün,1 Adnan İşgör2 1Department of General Surgery, Sisli Hamidiye Etfal Training and Research Hospital, Istanbul, Turkey 2Department of General Surgery, Bahcesehir University Faculty of Medicine, Istanbul, Turkey Abstract Indications for adrenalectomy are malignancy suspicion or malignant tumors, non-functional tumors with the risk of malignancy and functional adrenal tumors. Regardless of the size of functional tumors, they have surgical indications. The hormone-secreting adrenal tumors in which adrenalectomy is indicated are as follows: Cushing’s syndrome, arises from hypersecretion of glucocorticoids produced in fasciculata adrenal cortex, Conn’s syndrome, arises from an hypersecretion of aldosterone produced by glomerulosa adrenal cortex, and Pheochromocytomas that arise from adrenal medulla and produce catecholamines. Sometimes, bilateral adre- nalectomy may be required in Cushing's disease due to pituitary or ectopic ACTH secretion. Adenomas arise from the reticularis layer of the adrenal cortex, which rarely releases too much adrenal androgen and estrogen, may also develop and have an indication for adrenalectomy. Adrenal surgery can be performed by laparoscopic or open technique. Today, laparoscopic adrenalectomy is the gold standard treatment in selected patients. Laparoscopic adrenalectomy can be performed transperitoneally or retroperitoneoscopi- cally. Both approaches have their advantages and disadvantages. In the selection of the surgery type, the experience and habits of the surgeon are also important, along with the patient’s characteristics. The most common type of surgery performed in the world is laparoscopic transabdominal lateral adrenalectomy, which most surgeons are more familiar with. -

Ministry of Education and Science of Ukraine Sumy State University 0
Ministry of Education and Science of Ukraine Sumy State University 0 Ministry of Education and Science of Ukraine Sumy State University SPLANCHNOLOGY, CARDIOVASCULAR AND IMMUNE SYSTEMS STUDY GUIDE Recommended by the Academic Council of Sumy State University Sumy Sumy State University 2016 1 УДК 611.1/.6+612.1+612.017.1](072) ББК 28.863.5я73 С72 Composite authors: V. I. Bumeister, Doctor of Biological Sciences, Professor; L. G. Sulim, Senior Lecturer; O. O. Prykhodko, Candidate of Medical Sciences, Assistant; O. S. Yarmolenko, Candidate of Medical Sciences, Assistant Reviewers: I. L. Kolisnyk – Associate Professor Ph. D., Kharkiv National Medical University; M. V. Pogorelov – Doctor of Medical Sciences, Sumy State University Recommended for publication by Academic Council of Sumy State University as а study guide (minutes № 5 of 10.11.2016) Splanchnology Cardiovascular and Immune Systems : study guide / С72 V. I. Bumeister, L. G. Sulim, O. O. Prykhodko, O. S. Yarmolenko. – Sumy : Sumy State University, 2016. – 253 p. This manual is intended for the students of medical higher educational institutions of IV accreditation level who study Human Anatomy in the English language. Посібник рекомендований для студентів вищих медичних навчальних закладів IV рівня акредитації, які вивчають анатомію людини англійською мовою. УДК 611.1/.6+612.1+612.017.1](072) ББК 28.863.5я73 © Bumeister V. I., Sulim L G., Prykhodko О. O., Yarmolenko O. S., 2016 © Sumy State University, 2016 2 Hippocratic Oath «Ὄμνυμι Ἀπόλλωνα ἰητρὸν, καὶ Ἀσκληπιὸν, καὶ Ὑγείαν, καὶ Πανάκειαν, καὶ θεοὺς πάντας τε καὶ πάσας, ἵστορας ποιεύμενος, ἐπιτελέα ποιήσειν κατὰ δύναμιν καὶ κρίσιν ἐμὴν ὅρκον τόνδε καὶ ξυγγραφὴν τήνδε. -

Gender Dysphoria Treatment – Community Plan Medical Policy
UnitedHealthcare® Community Plan Medical Policy Gender Dysphoria Treatment Policy Number: CS145.I Effective Date: March 1, 2021 Instructions for Use Table of Contents Page Related Community Plan Policies Application ..................................................................................... 1 • Blepharoplasty, Blepharoptosis, and Brow Ptosis Coverage Rationale ....................................................................... 1 Repair Definitions ...................................................................................... 3 • Botulinum Toxins A and B Applicable Codes .......................................................................... 4 • Cosmetic and Reconstructive Procedures Description of Services ................................................................. 8 • Gonadotropin Releasing Hormone Analogs Benefit Considerations .................................................................. 9 Clinical Evidence ........................................................................... 9 • Panniculectomy and Body Contouring Procedures U.S. Food and Drug Administration ........................................... 14 • Rhinoplasty and Other Nasal Surgeries References ................................................................................... 14 • Speech Language Pathology Services Policy History/Revision Information ........................................... 16 Commercial Policy Instructions for Use ..................................................................... 16 • Gender Dysphoria Treatment -

Robotic Surgery for Male Infertility
Robotic Surgery for Male Infertility Annie Darves-Bornoz, MD, Evan Panken, BS, Robert E. Brannigan, MD, Joshua A. Halpern, MD, MS* KEYWORDS Robotic surgical procedures Infertility Male Vasovasostomy Varicocele KEY POINTS Robotic-assisted approaches to male infertility microsurgery have potential practical benefits including reduction of tremor, 3-dimensional visualization, and decreased need for skilled surgical assistance. Several small, retrospective studies have described robotic-assisted vasectomy reversal with com- parable clinical outcomes to the traditional microsurgical approach. Few studies have described application of the robot to varicocelectomy, testicular sperm extrac- tion, and spermatic cord denervation. The use of robotic-assistance for male infertility procedures is evolving, and adoption has been limited. Rigorous studies are needed to evaluate outcomes and cost-effectiveness. INTRODUCTION with intraperitoneal and pelvic surgery. On the other hand, many of the theoretic and practical ad- Up to 15% of couples have infertility, with approx- 1,2 vantages offered by the robotic approach are imately 50% of cases involving a male factor. A highly transferrable to surgery for male infertility: substantial proportion of men with subfertility have surgically treatable and even reversible etiologies, High quality, 3-dimensional visualization is such as a varicocele or vasal obstruction. The essential for any microsurgical procedure. introduction of the operating microscope revolu- Improved surgeon ergonomics are always desir- tionized the field of male infertility, dramatically able, particularly given the surgeon morbidity improving visualization of small, complex associated with microsurgery.3 anatomic structures. The technical precision Filtering of physiologic tremor can improve pre- afforded has improved operative outcomes across cision during technically demanding micro- the board. -
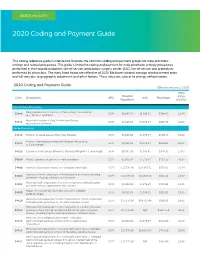
2020 Coding and Payment Guide
MEN’S HEALTH 2020 Coding and Payment Guide This coding reference guide is intended to illustrate the common coding and payment groups for male prosthetic urology and related procedures. This guide is limited to coding and payment for male prosthetic urology procedures performed in the hospital outpatient site-of-service, ambulatory surgery center (ASC) site-of-service and procedures performed by physicians. The rates listed below are reflective of 2020 Medicare national average reimbursement rates and will vary due to geographic adjustment and other factors. These rates are subject to change without notice. 2020 Coding and Payment Guide Effective January 1, 2020 Total Hospital Code Description APC ASC Physicians RVUs Outpatient (Facility) Urinary Sling Procedures Sling operation for correction of male urinary incontinence 53440 5376 $8,067.93 $6.546.11 $784.59 21.74 (e.g., fascia or synthetic) Removal or revision of sling for male incontinence 53442 5375 $4,231.62 $1,976.27 $816.35 22.62 (e.g., fascia or synthetic) Penile Procedures 54110 Excision of penile plaque (Peyronie’s Disease) 5374 $3,018.54 $1,376.97 $650.33 18.02 Excision of penile plaque (Peyronie’s Disease); with graft up 54111 5375 $4,231.62 $1,976.27 $834.03 23.11 to 5 cm in length 54112 Excision of penile plaque (Peyronie’s Disease); with graft > 5 cm in length 5376 $8,067.93 $3,995.65 $976.95 27.07 54360 Plastic operation on penis to correct angulation 5374 $3,018.54 $1,376.97 $751.39 20.82 54400 Insertion of penile prosthesis; non-inflatable (semi-rigid) 5377 $17,573.96 -

Ese-Ensat-Acc-Guidelines-13-5-2018
European Society of Endocrinology Clinical Practice Guidelines on the Management of Adrenocortical Carcinoma in Adults, in collaboration with the European Network for the Study of Adrenal Tumors Martin Fassnacht1,2*, Olaf M. Dekkers3,4,5, Tobias Else5, Eric Baudin7,8, Alfredo Berruti9, Ronald R. de Krijger10, 11, 12, 13, Harm R. Haak14,15, 16, Radu Mihai17, Guillaume Assie19, 20, Massimo Terzolo20* 1 Dept. of Internal Medicine I, Div. of Endocrinology and Diabetes, University Hospital, University of Würzburg, Würzburg, Germany 2 Comprehensive Cancer Center Mainfranken, University of Würzburg, Würzburg, Germany 3 Department of Clinical Epidemiology, Leiden University Medical Centre, Leiden, the Netherlands 4 Department of Clinical Endocrinology and Metabolism, Leiden University Medical Centre, Leiden, the Netherlands 5 Department of Clinical Epidemiology, Aarhus University Hospital, Aarhus, Denmark 6 Department of Internal Medicine, Division of Metabolism, Endocrinology and Diabetes, University of Michigan, Ann Arbor, MI, USA 7 Endocrine Oncology and Nuclear Medicine, Institut Gustave Roussy, Villejuif, France 8 INSERM UMR 1185, Faculté de Médecine, Le Kremlin-Bicêtre, Université Paris Sud, Paris, France 9 Department of Medical and Surgical Specialties, Radiological Sciences, and Public Health, Medical Oncology, University of Brescia at ASST Spedali Civili, Brescia, Italy. 10 Dept. of Pathology, Erasmus MC University Medical Center, Rotterdam, The Netherlands 11 Dept. of Pathology, University Medical Center Utrecht, Utrecht, The Netherlands 12 Dept. of Pathology, Reinier de Graaf Hospital, Delft, The Netherlands 13 Princess Maxima Center for Pediatric Oncology, Utrecht, The Netherlands 14 Department of Internal Medicine, Máxima Medical Centre, Eindhoven/Veldhoven, the Netherlands 15 Maastricht University, CAPHRI School for Public Health and Primary Care, Ageing and Long-Term Care, Maastricht, the Netherlands 16 Department of Internal Medicine, Division of General Internal Medicine, Maastricht University Medical Centre+, Maastricht, the Netherlands. -

Download Download
ACTA Official Journal of the Italian Society Otorhinolaryngologica Italica, 38/2, Supplement 1, S1-S106, 2018 S1-S106, Supplement 1, 38/2, Otorhinolaryngologica Italica, of Otorhinolaryngology Head and Neck Surgery Organo Ufficiale della Società Italiana di Otorinolaringologia e Chirurgia Cervico-Facciale 105th Congress of the Italian Society of Otorhinolaryngology Head and Neck Surgery Official report Emerging and re-emerging infectious disease in otorhinolaryngology Patologia infettiva emergente e riemergente in otorinolaringoiatria F. Scasso, G. Ferrari, G.C. De Vincentiis, A. Arosio, S. Bottero, M. Carretti, A. Ciardo, S. Cocuzza, A. Colombo, B. Conti, A. Cordone, M. De Ciccio, E. Delehaye, L. Della Vecchia, I. De Macina, C. Dentone, P. Di Mauro, R. Dorati, R. Fazio, A. Ferrari, G. Ferrea, S. Giannantonio, I. Genta, M. Giuliani, D. Lucidi, L. Maiolino, G. Marini, P. Marsella, D. Meucci, T. Modena, B. Montemurri, A. Odone, S. Palma, M.L. Panatta, M. Piemonte, P. Pisani, S. Pisani, L. Prioglio, A. Scorpecci, L. Scotto di Santillo, A. Serra, C. Signorelli, E. Sitzia, M.L. Tropiano, M. Trozzi, F.M. Tucci, L. Vezzosi, B. Viaggi Volume 38 • Supplement 1 April 2018 POSTE ITALIANE SPA - Spedizione in Abbonamento Postale - D.L. 353/2003 conv. in L. 27/02/2004 n° 46 art. 1, comma 1, DCB PISA - Iscrizione al tribunale di Pisa al n. 10 del 30-07-93 - ISSN: 0392-100X (Print) - ISSN: 1827-675X (Online) 10 del 30-07-93 - ISSN: DCB PISA - Iscrizione al tribunale di Pisa n. comma 1, 1, 27/02/2004 n° 46 art. in L. 353/2003 conv. Abbonamento Postale - D.L.