The Utility and Limitations of the Transfibular Approach in Ankle Trauma Surgery
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Anatomy: Lower Leg, Knee, & Patella Positioning
Reading assignment: Lower Leg Anatomy: lower leg, knee, & Merrils, Vol. 1: Chapter 6 Film Critique #3 patella Lab demonstration Positioning: lower leg Positioning: knee Reading assignment: Knee Merrils, Vol. 1: Chapter 6 Film Critique #4 & Lab demonstration Positioning: intercondylar fossa Reading assignment: Intercondylar fossa and patella & patella Merrils, Vol. 1: Chapter 6 Lab demonstration Anatomy: Femur Reading assignment: Femur Positioning: Femur Merrils, Vol. 1: Chapters 6 & 7 Film Critique #5 Lab demonstration Leg…… The leg is composed of two long bones: Tibia – medial bone; second largest bone in the body Fibula – lateral bone The tibia has several anatomical features of note. See whether you can locate each on the diagram. Proximal end: Medial condyle Lateral condyle Tibial plateaus Intercondylar eminence Tibial tuberosity Body – features anterior crest Distal end: Medial malleolus Fibular notch The head of the fibula is located at its proximal end and has a pointed apex laterally. Distally, the fibular features the lateral malleolus. The articulations between the two leg bones are discussed on Screen 1.13. Knee….. The knee joint is the articulation between the femoral condyles and the tibial plateaus. Numerous soft tissues support and reinforce the knee, including the: Menisci Cruciate ligaments Collateral ligaments These supporting soft tissue structures are enclosed in a common joint capsule. The knee joint is of the hinge type, capable of flexion and extension only. The anterior knee joint is protected by the patella and patellofemoral joint. The patella is the largest and most constant sesamoid bone. It develops in the quadriceps femoris tendon between the ages of 3 and 5 years. -

Anatomy, Bony Pelvis and Lower Limb, Leg Bones
NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Anatomy, Bony Pelvis and Lower Limb, Leg Bones Authors Austin J. Cantrell1; Matthew Varacallo2. Affiliations 1 University of Oklahoma College of Med. 2 Department of Orthopaedic Surgery, University of Kentucky School of Medicine Last Update: January 17, 2019. Introduction The leg is the region of the lower limb between the knee and the foot. It comprises two bones: the tibia and the fibula. The role of these two bones is to provide stability and support to the rest of the body, and through articulations with the femur and foot/ankle and the muscles attached to these bones, provide mobility and the ability to ambulate in an upright position. The tibia articulates with the femur at the knee joint. The knee joint consists of three compartments [1][2] medial tibiofemoral compartment lateral tibiofemoral compartment patellofemoral compartment At the ankle, the tibia and fibula create the articular surface for the talus. The ankle mortise is a specialized articulation providing support and optimizing motion and function through the ankle joint. A normal ankle joint ultimately optimizes and allows for physiologic mobility of the foot and its associated joints and articulations. The bones and fascia also divide the lower leg into four compartments [3][4] anterior compartment lateral compartment posterior compartment, superficial posterior compartment, deep Structure and Function The tibia is the second largest bone in the body and provides support for a significant portion of the weight-bearing forces transmitted from the rest of the body. -
Bones of the Lower Limb Doctors Notes Notes/Extra Explanation Editing File Objectives
Color Code Important Bones of the Lower Limb Doctors Notes Notes/Extra explanation Editing File Objectives Classify the bones of the three regions of the lower limb (thigh, leg and foot). Memorize the main features of the – Bones of the thigh (femur & patella) – Bones of the leg (tibia & Fibula) – Bones of the foot (tarsals, metatarsals and phalanges) Recognize the side of the bone. ﻻ تنصدمون من عدد ال رشائح نصها رشح زائد وملخصات واسئلة Some pictures in the original slides have been replaced with other pictures which are more clear BUT they have the same information and labels. Terminology (Team 434) شيء مرتفع /Eminence a small projection or bump Terminology (Team 434) Bones of thigh (Femur and Patella) Femur o Articulates (joins): (1) above with Acetabulum of hip bone to form the hip joint, (2) below with tibia and patella to form the knee joint. Body of femur (shaft) o Femur consists of: I. Upper end. II. Shaft. III. Lower end. Note: All long bones consist of three things: 1- upper/proximal end posterior 2- shaft anterior 3- lower/distal end I. Upper End of Femur The upper end contains: A. Head B. Neck C. Greater trochanter & D. Lesser trochanter A. Head: o Articulates (joins) with acetabulum of hip bone to form the hip joint. o Has a depression in the center called Fovea Capitis. o The fovea capitis is for the attachment of ligament of the head of Femur. o An artery called Obturator Artery passes along this ligament to supply head of Femur. B. Neck: o Connects head to the shaft. -

Bones of Lower Limb
BONES OF LOWER LIMB ANATOMY DEPARTMENT Dr. Sanaa Alshaarawi OBJECTIVES • At the end of the lecture the students should be able to: • Classify the bones of the three regions of the lower limb (thigh, leg and foot). • Memorize the main features of the – Bones of the thigh (femur & patella) – Bones of the leg (tibia & Fibula). – Bones of the foot (tarsals, metatarsals and phalanges) • Recognize the side of the bone BONES OF THIGH (Femur and Patella) Femur: . Articulates above with acetabulum of hip bone to form the hip joint. Articulates below with tibia and patella to form the knee joint. BONES OF THIGH (Femur and Patella) • Femur : Consists of : • Upper end • Shaft • Lower end Posterior view Anterior View UPPER END OF FEMUR • Head : • It articulates with acetabulum of hip bone to form hip joint. • Has a depression in the center (fovea capitis), for the attachment of ligament NECK of the head of femur. • Obturator artery passes along this ligament to supply head of femur. • Neck : • It connects head to the shaft. UPPER END OF FEMUR • Greater & lesser trochanters : • Anteriorly, connecting the 2 trochanters, the inter-trochanteric line, where the iliofemoral ligament is attached. • Posteriorly, the inter- trochanteric crest, on which is the quadrate tubercle (Qudratus femoris muscle). SHAFT OF FEMUR It has 3 surfaces Anterior Medial Lateral It has 3 borders Two rounded medial and lateral One thick posterior border or ridge called Anterior view Posterior view linea aspera SHAFT OF FEMUR • Anteriorly : is smooth and rounded. • Posteriorly : has a ridge, the linea aspera. • Posteriorly : below the greater trochanter is the gluteal tuberosity for attachment of gluteus M maximus muscle. -

A Fibular Notch Approach for the Treatment of Ankle Fractures Involving the Distal Tibial Plafond
A Fibular Notch Approach for the Treatment of Ankle Fractures Involving the Distal Tibial Plafond Tong Liu Department of Orthopaedics, Yantaishan Hospital Yiheng Cheng Department of Orthopaedics, Yantaishan Hospital Wenqing Qu ( [email protected] ) Department of Orthopaedics, Qilu Hospital(Qingdao) , Shandong University; 2 Department of Orthopedics,Yantaishan Hospital https://orcid.org/0000-0002-0099-1858 Research article Keywords: Ankle fractures, Pilon fractures, Distal tibial plafond fractures, Surgical approach, Fibular notch Posted Date: December 21st, 2020 DOI: https://doi.org/10.21203/rs.3.rs-129852/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Version of Record: A version of this preprint was published on February 8th, 2021. See the published version at https://doi.org/10.1186/s13018-021-02270-3. Page 1/12 Abstract BACKGROUND: Although several approaches have been used for the treatment of complex ankle fractures, there are still some ankle fractures which can not obtain ideal intraoperative exposure with these traditional approaches. The purpose of this study was to present an innovative bular notch approach in detail for the treatment of ankle fractures involving the distal tibial plafond and to present a series of patients with either functional or radiographic outcomes. METHODS: Between March 2015 and October 2018, 22 patients with distal tibial plafond fractures with concomitant bular and distal tibiobular syndesmosis injuries were treated through a bular notch approach. The details of the surgical technique were reviewed from the operative notes. Relevant data were reviewed from the medical records. The quality of fractures and syndesmosis reduction was examined using CT scans, and lateral stability of the ankle was assessed by physical examination and stress radiographs. -
Lab Activity 9
Lab Activity 9 Appendicular Skeleton Martini Chapter 8 Portland Community College BI 231 Appendicular Skeleton • Upper & Lower extremities • Shoulder Girdle • Pelvic Girdle 2 Humerus 3 Humerus: Proximal End Greater tubercle Lesser tubercle Head: Above the epiphyseal line Anatomical Neck Surgical neck Intertubercular groove Anterior Medial Posterior4 Deltoid Tuberosity 5 Radial Groove 6 Trochlea (Distal Humerus) Anterior Posterior Anterior Posterior 7 Capitulum (Distal Humerus) Anterior Posterior Anterior Posterior 8 Olecranon Fossa (Distal Humerus) Anterior Posterior Anterior Posterior 9 Medial Epicondyle (Distal Humerus) Anterior Posterior Anterior Posterior 10 Lateral Epicondyle (Distal Humerus) Anterior Posterior Anterior Posterior 11 Radial Fossa (Distal Humerus) Anterior Posterior Anterior Posterior 12 Coronoid Fossa (Distal Humerus) Anterior Posterior Anterior Posterior 13 Lateral Supracondylar Ridge (Distal Humerus) Anterior Posterior Anterior Posterior 14 Medial Supracondylar Ridge (Distal Humerus) Anterior Posterior Anterior Posterior 15 Humerus: Distal End/Anterior Medial Lateral Supracondylar Supracondylar Ridge Ridge Coronoid Fossa Radial fossa Lateral Medial Epicondyle Epicondyle Capitulum Trochlea 16 Humerus: Distal End/Posterior Olecranon Fossa Medial Epicondyle Lateral Epicondyle Trochlea 17 Radius • “Rotates” • On the thumb side of the forearm 18 Radius: Head 19 Radial Tuberosity 20 Ulnar Notch of the Radius 21 Ulnar Notch of the Radius 22 Radius: Interosseous Ridge 23 Styloid Process of the Radius 24 Radius Distal Anterior -
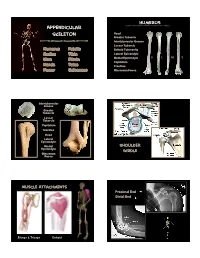
Appendicular Skeleton
Humerus Appendicular Skeleton Head Greater Tubercle Intertubercular Groove Lesser Tubercle Humerus Patella Deltoid Tuberosity Radius Tibia Lateral Epicondyle D L M V Ulna Fibula Medial Epicondyle Capitulum Hands Talus Trochlea Femur Calcaneus Olecrenon Fossa Intertubercular Groove Greater Tubercle Lesser Tubercle Capitulum Trochlea Head Lateral Epicondyle Medial Shoulder Epicondyle Girdle Olecrenon Fossa Muscle Attachments Proximal End Distal End Biceps & Triceps Deltoid 1 Radius Ulna Head Neck Radial Tuberosity Interosseous Crest Styloid Process Olecrenon Process Ulnar Notch Radial Notch Tuberosity L M D V Styloid Process D L M V Interosseous Crest Trochlea Radial Tuberosity Olecrenon Process Capitulum Head Medial Epicondyle Phalanges 1st 3rd Proximal Phalange 3rd Metacarpals 1st Proximal Phalange 2 Femur Head, medial Larger epicondyle, lateral Femur head Olecrenon fossa, distal Fovea capitus Olecrenon process, proximal Greater trochanter Radial notch, lateral Lesser trochanter Styloid process, towards ‘pinky’ Linea aspera Head, proximal Medial condyle Tuberosity, medial Lateral condyle Styloid towards thumb Intercondylar fossa V D L M Patellar articular surface Proximal Femur Fovea capitus Trochanteric Fossa Greater Trochanter Lesser femur humerus Trochanter Proximal Femur Medial condyle Lateral condyle Patella Patellar articular surface Intercondylar notch V D Apex Base Facet for lateral femoral condyle Distal Femur Facet for medial femoral condyle 3 Tibia Tibia Lateral condyle Lateral condyle Medial condyle Medial condyle Fibular -
Lab Manual Appendicular Skele
1 PRE-LAB EXERCISES When studying the skeletal system, the bones are often sorted into two broad categories: the axial skeleton and the appendicular skeleton. This lab focuses on the appendicular skeleton, which is formed from the pectoral and pelvic girdles and the upper and lower limbs. View Module 7.2 Axial and Appendicular Skeleton to highlight the bones of the appendicular skeleton and compare them to those of the axial skeleton. Examine Module 11.1 Appendicular Skeleton to view only the bones of the appendicular skeleton. In addition to learning about all the bones of the appendicular skeleton, it is also important to identify some significant bone markings. Bone markings can have many shapes, including holes, round or sharp projections, and shallow or deep valleys, among others. These markings on the bones serve many purposes, including forming attachments to other bones or muscles and allowing passage of a blood vessel or nerve. It is helpful to understand the meanings of some of the more common bone marking terms. Before we get started, look up the definitions of these common bone marking terms: Canal: Condyle: Facet: Fissure: Foramen: (see Module 10.18 Foramina of Skull) Fossa: Margin: Process: Proximal: Trochanter: Tubercle: Tuberosity: Throughout this exercise, you will notice bold terms. This is meant to focus your attention on these important words. Make sure you pay attention to any bold words and know how to explain their definitions and/or where they are located. Use the following modules to guide your exploration of the appendicular skeleton. As you explore these bones in Visible Body’s app, also locate the bones and bone markings on any available charts, models, or specimens. -

Study of Distal Dimensions of Tibia in Correlation with The
International Journal of Anatomy and Research, Int J Anat Res 2018, Vol 6(2.3):5354-59. ISSN 2321-4287 Original Research Article DOI: https://dx.doi.org/10.16965/ijar.2018.206 STUDY OF DISTAL DIMENSIONS OF TIBIA IN CORRELATION WITH THE LENGTH OF TIBIA Yogi Anupkumar Balakrishnan 1, S.Vikram *2, Chitra Prakash Rao 3, Sanjay Kumar B Revankar 4. 1 Assistant professor of Anatomy Malankara orthodox syrian church medical college, kolenchery Kerala, India. *2 Associate Professor of Anatomy A.J Institute of Medical Sciences and Research centre, Mangalore,India. 3 Professor and HOD of Anatomy A.J Institute of Medical Sciences and Research centre, Mangalore, India. 4 Assistant professor of Anatomy, A.J Institute of Medical Sciences and Research centre, Mangalore, India. ABSTRACT Background: In forensic analysis, the estimation of the stature is key in identification of an individual. The stature of an individual can be estimated from long bones especially the tibia and the femur as these have direct correlation to the height of an individual. The tibia is ideal in this application as it resists erosion and keeps its anatomical shape for long even after burial. Mechanical loading is especially high in the distal ends of long bones of the lower limb and as such they display significant inter-individual differences. The use of distal dimensions in estimation of the length of the tibia from skeletal remains has not been reported. Materials and methods: 150 dry and processed tibias irrespective of side, grossly normal and complete were randomly collected from a medical college of south India. -

Morphological and Morphometrical Analysis of Fibula in Relation to Fibular Facet P
Research Article Morphological and morphometrical analysis of fibula in relation to fibular facet P. Santhanam, Karthik Ganesh Mohanraj* ABSTRACT Introduction: The fibula bone is also known as the calf bone, which was introduced into anatomical nomenclature by Vesalius during the 16th century. Fibula is a slender lateral bone of the leg, the fibula is identified by a proximal head, with a twisted shaft and a distal lateral malleolus. The lower ends of the bone fibula and tibia form an anatomic and functional unit. In view of the widespread clinical relevance, the purpose of this study was to investigate the morphology and morphometric analysis of the human fibula bone in relation to fibular incisura within South Indian population group. Materials and Methods: In the present study, a total of 30 dry human fibula bones of unknown sex and without any gross abnormality will be collected from the Department of Anatomy, Saveetha Dental College, Chennai, for evaluation. With the help of Vernier caliper and ruler, the measurements such as the length, breadth, and diameter of the orbital cavity will be measured. The maximum orbital length and the maximal orbital breadth are measured to calculate the orbital index. The results obtained were analyzed, tabulated, and represented graphically. Results: After analyzing the data we come to know that diameter from upper and lower articulating facet seems to lie between 2 cm and 2.5 cm and height of lateral malleolus tend to be between 2.5 cm and 3 cm in the analyzed dry bone. About 50% of the bone sample contains nutrient foramen at inferior one-third, 40% contain at superior one-third, and only 10% contain nutrient foramen at the middle one-third. -

Anatomy Lab: the Skeletal System Part I: Vertebrae and Thoracic Cage
ANA Lab: Bone 1 Anatomy Lab: The skeletal system Part I: Vertebrae and Thoracic cage Spine (Vertebrae) Body Vertebral arch Vertebral canal Pedicle Lamina Spinous process Transverse process Sup. articular facets Inf. articular facets Sup. vertebral notch Inf. vertebral notch Intervertebral foramen Cervical vertebrae: 7 Typical (C3-C6) Transverse foramen C1, Atlas C2, Axis: dens C7 Thoracic vertebrae: 12 Typical (T2-T10) T1 T11, 12 Lumbar vertebrae: 5 Typical (L1-4) Sacrum: 5 Ala Anterior sacral foramina Posterior sacral foramina Sacral canal ANA Lab: Bone 2 Sacral hiatus promontory median sacral crest intermediate crest lateral crest Coccyx Horns Transverse process Thoracic cages Ribs: 12 pairs Typical ribs (R3-R10): Head, 2 facets intermediate crest neck tubercle angle costal cartilage costal groove R1 R2 R11,12 Sternum Manubrium of sternum Clavicular notch for sternoclavicular joint body xiphoid process ANA Lab: Bone 3 Part II: Skull and Facial skeleton Skull Cranial skeleton, Calvaria (neurocranium) Facial skeleton (viscerocranium) Overview: identify the margin of each bone Cranial skeleton 1. Lateral view Frontal Temporal Parietal Occipital 2. Cranial base midline: Ethmoid, Sphenoid, Occipital bilateral: Temporal Viscerocranium 1. Anterior view Ethmoid, Vomer, Mandible Maxilla, Zygoma, Nasal, Lacrimal, Inferior nasal chonae, Palatine 2. Inferior view Palatine, Maxilla, Zygoma Sutures: external view vs. internal view Coronal suture Sagittal suture Lambdoid suture External appearance of skull Posterior view external occipital protuberance -

Upper Extremity 2 Lower Extremity 1
Upper extremity 2 Lower extremity 1 Carpal bones Scaphoid Lunate Triquetrum Pisiform Trapezium Phalanges Metacarpals [I-V] Proximal phalanx Base Trapezoid Middle phalanx Shaft; Body Capitate Distal phalanx Head Hamate Tuberosity of distal phalanx Styloid process of Hook of hamate Base of phalanx third metacarpal [III] Carpal groove Body of phalanx Head of phalanx,Trochlea of phalanx Hip bone; Coxal bone; Pelvic bone Ischium, Ilium, Pubic Acetabulum Acetabular margin Acetabular fossa Acetabular notch Lunate surface Ischiopubic ramus Obturator foramen Greater sciatic notch Ilium Body of ilium Ala of ilium; Wing of ilium Arcuate line Iliac crest Anterior superior iliac spine Anteriror inferior iliac spine Posterior superior iliac spine Posterior inferior iliac spine Iliac fossa Gluteal surface Anterior gluteal line Posterior gluteal line Inferior gluteal line Sacropelvic surface Auricular surface Iliac tuberosity Ischium Body Ramus Ischial tuberosity Ischial spine Lesser sciatic notch Pubis Body Pubic tubercle Symphysial surface Superior pubic ramus Iliopubic ramus Pecten pubis; Pectineal line Obturator groove Inferior pubic ramus Head Fovea for ligament Neck Lesser trochanter Intertrochanteric line and crest Shaft of femur; Body of femur Linea aspera, Lateral lip, Medial lip Pectinal line; Gluteal tuberosity Popliteal surface Medial condyle, Medial epicondyle Adductor tubercle Lateral condyle and epicondyle Patellar surface Intercondylar fossa Intercondylar line The proximal femur is bent (L-shaped) so that the long axis of the head and neck project superomedially at an angle to that of the obliquely oriented shaft This obtuse angle of inclination in the adult is 115 to 140 degrees, averaging 126 degrees. The angle is less in females because of the increased width between the acetabula and the greater obliquity of the shaft.