ADDENDUM for THORIUM Supplement to the 1990 Toxicological Profile for Thorium
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Radiological Significance of Thorium Processing in Manufacturing
Attention Microfiche User, . The original document from which this microfiche was made was found to contain some imperfection or imperfections that redtice full comprehension of some of the text despite the gcod technical quality of the microfiche itself. The imperfections may be: - missing or illegible pages/figures - wrong pagination - poor overall printing quality, etc. We normally refuse to microfiche such a document and request a replacement document (or pages) from the National INIS Centre concerned. However, our experience shows that many months pass before such documents are replaced. Sometimes the Centre is not able to supply a better copy or, in some cases, the pages that were supposed to be missing correspond to a wrong pagination only. Me feel that it is better to proceed with distributing the microfiche made of these documents than to withhold them till the imperfections are removed. If the removals are subsequestly made then replacement microfiche can be issued. In line with this approach then, our specific practice for microfiching documents with imperfections is as follows: 1. A microfiche of an imperfect document will be marked with a special symbol (black circle) on the left of the title. This symbol will appear on all masters and copies of the document (1st fiche and trailer fiches) even if the imperfection is on one fiche of the report only. 2. If imperfection is not too general the reason will be specified on a sheet such as this, in the space below. 3. The microfiche will be considered as temporary, but sold at the normal price. Replacements, if they can be issued, will be available for purchase at the regular price. -

Thermodynamic Properties of Thorium Dioxide from 298 to 1200 Ok
JO URNAL OF RESEARCH of the National Bureau of Standards-A. Physics and Chemistry Vol. 65, No.2, March- April 1961 Thermodynamic Properties of Thorium Dioxide From 298 to 1,200 oK Andrew C. Victor and Thomas B. Douglas (November 26, 1960) As a step in developing new standards of he.at ca l ~ac i ty applicable up to very h~gh temperatures, t he heat content (enthalpy) of thol'lum dlOxldoe, I h02 , relatn:,e to 2~3 K , was accurately measured at ten temperatures from 323 to 1,173 K . A Bunsen 1.ce ca l ol'l~neter and a drop method were used to make t he mea ~ urements on two samples of ":ldely d Iff erent bulk densities. The corresponding heat-capacity values for the hIgher denSIty sample ~re represented within t heir uncertain ty (estimated to be ± 0.3 to 0.5 %) by the followlI1g empirical equation 1 (cal mole- I deg- I at T OK) : C ~ = 17 . 057 + 1 8. 06 ( 10 -4) T - 2.5166 (1 05)/1'2 At 298 oK t his equation agrees with previously reported low-temperatu.re measurements made with an adiabatic calorimeter. Values of heat content, heat capaelty, entropy, and Gibb's free energy function are tabulated from 298.15 t o 1,200 oK. 1. Introduction measll remen ts arc soon to be extended up to ap proximately 1,800 OK. Current practical and theoretical developm~l!ts However, at higher temperatures aluminum oxide have increased the need for accurate heat capaCltlOs is impractical as a heat standard, for it becomes and related thermal properties at high temp ~rature s, increasingly volatile, and melts at approximately yet the values reported for the same mat~nal from 2,300 OK. -

Extraction of Thorium Oxide from Monazite Ore
University of Tennessee, Knoxville TRACE: Tennessee Research and Creative Exchange Supervised Undergraduate Student Research Chancellor’s Honors Program Projects and Creative Work 5-2019 Extraction of Thorium Oxide from Monazite Ore Makalee Ruch University of Tennessee, Knoxville, [email protected] Chloe Frame University of Tennessee, Knoxville Molly Landon University of Tennessee, Knoxville Ralph Laurel University of Tennessee, Knoxville Annabelle Large University of Tennessee, Knoxville Follow this and additional works at: https://trace.tennessee.edu/utk_chanhonoproj Part of the Environmental Chemistry Commons, Geological Engineering Commons, and the Other Chemical Engineering Commons Recommended Citation Ruch, Makalee; Frame, Chloe; Landon, Molly; Laurel, Ralph; and Large, Annabelle, "Extraction of Thorium Oxide from Monazite Ore" (2019). Chancellor’s Honors Program Projects. https://trace.tennessee.edu/utk_chanhonoproj/2294 This Dissertation/Thesis is brought to you for free and open access by the Supervised Undergraduate Student Research and Creative Work at TRACE: Tennessee Research and Creative Exchange. It has been accepted for inclusion in Chancellor’s Honors Program Projects by an authorized administrator of TRACE: Tennessee Research and Creative Exchange. For more information, please contact [email protected]. Extraction of Thorium Oxide from Monazite Ore Dr. Robert Counce Department of Chemical and Biomolecular Engineering University of Tennessee Chloe Frame Molly Landon Annabel Large Ralph Laurel Makalee Ruch CBE 488: Honors -

Fabrication of Thorium and Thorium Dioxide
Natural Science, 2015, 7, 10-17 Published Online January 2015 in SciRes. http://www.scirp.org/journal/ns http://dx.doi.org/10.4236/ns.2015.71002 Fabrication of Thorium and Thorium Dioxide Balakrishna Palanki (Retired) Nuclear Fuel Complex, Hyderabad, India Email: [email protected] Received 10 November 2014; revised 9 December 2014; accepted 28 December 2014 Copyright © 2015 by author and Scientific Research Publishing Inc. This work is licensed under the Creative Commons Attribution International License (CC BY). http://creativecommons.org/licenses/by/4.0/ Abstract Thorium based nuclear fuel is of immense interest to India by virtue of the abundance of Thorium and relative shortage of Uranium. Thorium metal tubes were being cold drawn using copper as cladding to prevent die seizure. After cold drawing, the copper was removed by dissolution in ni- tric acid. Thorium does not dissolve being passivated by nitric acid. Initially the copper cladding was carried out by inserting copper tubes inside and outside the thorium metal tube. In an inno- vative development, the mechanical cladding with copper was replaced by electroplated copper with a remarkable improvement in thorium tube acceptance rates. Oxalate derived thoria powder was found to require lower compaction pressures compared to ammonium diuranate derived urania powders to attain the same green compact density. However, the green pellets of thoria were fragile and chipped during handling. The strength improved after introducing a ball milling step before compaction and maintaining the green density above the specified value. Alternatively, binders were used later for greater handling strength. Magnesia was conventionally being used as dopant to enhance the sinterability of thoria. -
Aec-Nasa Tech Brief
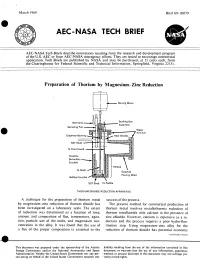
March 1969 Brief 69-10079 sty C AEC-NASA TECH BRIEF YES AEC-NASA Tech Briefs describe innovations resulting from the research and development program of the U.S. AEC or from AEC-NASA interagency efforts. They are issued to encourage commercial application. Tech Briefs are published by NASA and may be purchased, at 15 cents each, from the Clearinghouse for Federal Scientific and Technical Information, Springfield, Virginia 22151. Preparation of Thorium by Magnesium—Zinc Reduction Stirring Motor Ball Valve Stuffing Box Assembly Sampling Port - Water Annulus Graphitar Bearing 1___._Hea t Shields SST Shaft Ta Thermowell Graphite Secondary Crucible Heated Ta Shaft Graphite Pouring Mold Baffled Crucible^v I SST Shell Ta Paddle THORIUM DIOXIDE REDUCTION APPARATUS A technique for the preparation of thorium metal success of the process. by magnesium—zinc reduction of thorium dioxide has The present method for commercial production of been investigated on a laboratory scale. The extent thorium metal involves metallothermic reduction of of reduction was determined as a function of time, thorium tetrafluoride with calcium in the presence of amount and composition of flux, temperature, agita- zinc chloride. However, calcium is expensive as a re- tion, particle size of the oxide, and magnesium con- ductant and the process requires a prior hydro-fluo- centration in the alloy. It was found that the use of rination step. Using magnesium—zinc alloy for the a flux of the proper composition is essential to the reduction of thorium dioxide has potential economic (continued overleaf) This document was prepared under the sponsorship of the Atomic liability resulting from the use of the information contained in this Energy Commission and/or the National Aeronautics and Space document, or warrants that the use of any information, apparatus, Administration. -

Chemical Compatibility Storage Group
CHEMICAL SEGREGATION Chemicals are to be segregated into 11 different categories depending on the compatibility of that chemical with other chemicals The Storage Groups are as follows: Group A – Compatible Organic Acids Group B – Compatible Pyrophoric & Water Reactive Materials Group C – Compatible Inorganic Bases Group D – Compatible Organic Acids Group E – Compatible Oxidizers including Peroxides Group F– Compatible Inorganic Acids not including Oxidizers or Combustible Group G – Not Intrinsically Reactive or Flammable or Combustible Group J* – Poison Compressed Gases Group K* – Compatible Explosive or other highly Unstable Material Group L – Non-Reactive Flammable and Combustible, including solvents Group X* – Incompatible with ALL other storage groups The following is a list of chemicals and their compatibility storage codes. This is not a complete list of chemicals, but is provided to give examples of each storage group: Storage Group A 94‐75‐7 2,4‐D (2,4‐Dichlorophenoxyacetic acid) 94‐82‐6 2,4‐DB 609-99-4 3,5-Dinitrosalicylic acid 64‐19‐7 Acetic acid (Flammable liquid @ 102°F avoid alcohols, Amines, ox agents see SDS) 631-61-8 Acetic acid, Ammonium salt (Ammonium acetate) 108-24-7 Acetic anhydride (Flammable liquid @102°F avoid alcohols see SDS) 79‐10‐7 Acrylic acid Peroxide Former 65‐85‐0 Benzoic acid 98‐07‐7 Benzotrichloride 98‐88‐4 Benzoyl chloride 107-92-6 Butyric Acid 115‐28‐6 Chlorendic acid 79‐11‐8 Chloroacetic acid 627‐11‐2 Chloroethyl chloroformate 77‐92‐9 Citric acid 5949-29-1 Citric acid monohydrate 57-00-1 Creatine 20624-25-3 -
A Computational Analysis of Thorium Dioxide and Th(1-X)Uxo2 Systems
University College London A Computational Analysis of Thorium Dioxide and Th(1-x)UxO2 Systems Thesis submitted for the degree of Doctor of Philosophy (PhD) by Ashley Elizabeth Shields Supervisor: Professor Nora H. de Leeuw University College London Department of Chemistry December 2015 Declaration I, Ashley Elizabeth Shields, confirm that the work presented in this thesis is my own. Where information has been derived from other sources, I confirm that this has been properly indicated and fully acknowledged in the thesis. Ashley Elizabeth Shields December 2015 2 Abstract Nuclear power generation is an important way to satisfy rising global energy needs without increasing dependence on coal and petroleum. However, conventional nuclear fuels, such as uranium and plutonium dioxides, raise several safety concerns. Many countries have shown a renewed interest in thorium-based fuels as a potentially safer alternative. Thorium dioxide requires small amounts of a neutron source, such as uranium or plutonium, to generate a sustainable fission reaction. Due to the hazards of conducting experimental work on radioactive substances, a robust theoretical understanding of this doped- ThO2 fuel is needed. Using Density Functional Theory (DFT), we have studied the effects of uranium addition on the electronic structures of both the pure thoria bulk structure and three flat surfaces of ThO2 and simulated Scanning Tunneling Microscopy (STM) images of each surface. We have also studied the effect of a uranium adatom on these surfaces. However, we wished to study larger systems than are practical to simulate with DFT, and so we developed a new Th-O Buckingham- type force field that has been optimized to work with a leading UO2 interatomic potential. -

Thermodynamic Model for the Solubility of Thorium Dioxide in The
Radiochim. Acta 88, 2972306 (2000) by Oldenbourg Wissenschaftsverlag, München Thermodynamic model for the solubility of thorium dioxide + – – ° ° in the Na -Cl -OH -H2O system at 23 C and 90 C By Dhanpat Rai1,*, Dean A. Moore1, Charles S. Oakes1 and Mikazu Yui2 1 Pacific Northwest National Laboratory, Richland, Washington 99352, USA 2 Japan Nuclear Cycle Development Institute, Tokai Works, Tokai, Japan (Received August 30, 1999; accepted in revised form March 8, 2000) Solubility / Thermodynamics / Thorium dioxide / ThO2(c) / at room temperature. Therefore, potential thorium concen- ThO2(am) / Temperature effects on ThO2 crystallinity / trations in aqueous solutions contacting failed repositories Solubility product / Solubility products at different may be many orders of magnitude lower than indicated by temperatures measurements of ThO2(am) solubility at 25 °C. At 25 °C, the precipitation/dissolution kinetics of Summary. Data are extremely limited on the effects of tem- ThO2(c) are not known, which makes it difficult to accu- perature on crystallinity and the resulting changes in solubility rately ascertain the solubility product of ThO2(c) at this products of thermally transformed thorium oxide phases. Such temperature. Fortunately, in addition to being relevant to data are required to reliably predict thorium behavior in high- expected repository conditions, a moderate increase in tem- level waste repositories where higher than ambient tempera- perature accelerates the precipitation/dissolution kinetics tures are expected. Solubility studies were conducted as a func- such that the solubility of ThO2(c) can be approached from tion of pH and time and at 0.1 M NaCl for 1) ThO2(am) at both the oversaturation and undersaturation directions. -

Toxicological Profile for Thorium
f Toxicological Profile for Thorium September 2019 ***DRAFT – DO NOT CITE OR QUOTE – August 29, 2019*** Version 4.0 THORIUM ii DISCLAIMER Use of trade names is for identification only and does not imply endorsement by the Agency for Toxic Substances and Disease Registry, the Public Health Service, or the U.S. Department of Health and Human Services. THORIUM iii FOREWORD This toxicological profile is prepared in accordance with guidelines* developed by the Agency for Toxic Substances and Disease Registry (ATSDR) and the Environmental Protection Agency (EPA). The original guidelines were published in the Federal Register on April 17, 1987. Each profile will be revised and republished as necessary. The ATSDR toxicological profile succinctly characterizes the toxicologic and adverse health effects information for these toxic substances described therein. Each peer-reviewed profile identifies and reviews the key literature that describes a substance's toxicologic properties. Other pertinent literature is also presented, but is described in less detail than the key studies. The profile is not intended to be an exhaustive document; however, more comprehensive sources of specialty information are referenced. The focus of the profiles is on health and toxicologic information; therefore, each toxicological profile begins with a relevance to public health discussion which would allow a public health professional to make a real-time determination of whether the presence of a particular substance in the environment poses a potential threat to human health. The adequacy of information to determine a substance's health effects is described in a health effects summary. Data needs that are of significance to the protection of public health are identified by ATSDR. -

Denton Infinity 22 E-Beam Evaporation Users Manual
Denton Infinity 22 E-beam Evaporation Users Manual Coral name: E-beam Evap 2 Model: Infinity 22 Location: CNST NanoFab, Building 215, Room B104 Contact: [email protected] Version: 1.0 Page | Coral Name: E-Beam 2 Equipment Information Sheet CNST NanoFab Denton Electron Beam Evaporator #2 TOOL CONTACT INFORMATION Phone Extension Email Process: Gerard Henein x5645 [email protected] Process: Jerry Bowser x8187 [email protected] Maintenance: Bill Young x4467 [email protected] Maintenance: Larry Buck x2242 [email protected] Training: Gerard Henein x5645 [email protected] APPLICATIONS Vacuum deposition of metallic and dielectric thin films SYSTEM 6-pocket electron gun turret Oxygen ion gun for ion-assisted deposition and native oxide removal Base vacuum: 1E-7 Torr Pumpdown from atmosphere to 3E-6 Torr in ~ 20 minutes SAFETY No unusual hazards during normal operation Do not attempt to unjam turret if stuck. Contact NanoFab staff for help. MATERIAL RESTRICTIONS No high vapor pressure materials (Bi, Pb, Sn, Zn, Cd, etc.). No In, Li. Maximum thickness per layer 200nm. Any exception must be approved by NanoFab staff REQUIREMENTS Only qualified users may operate MUST LOGIN TO CORAL AND ENABLE TOOL BEFORE OPERATING Fill out logbook Make sure materials are loaded in correct pockets Make sure beam is centered in pocket (LED indicators and direct view) PROHIBITIONS Never touch any internal part on the tool with bare hands or contaminated gloves Contact staff before depositing any new material OTHER INFORMATION Page | Always check the material file parameters in film deposition controller prior to evaporation Report problem to the maintenance staff and leave a note on Coral Always leave tool pumped down when you are finished Overview This tool is an electron beam evaporator (also referred to as “electron gun” or “e-beam”). -

A Density Functional Theory Study of Uranium-Doped Thoria and Uranium Adatoms on the Major Surfaces of Thorium Dioxide
Journal of Nuclear Materials 473 (2016) 99e111 Contents lists available at ScienceDirect Journal of Nuclear Materials journal homepage: www.elsevier.com/locate/jnucmat A density functional theory study of uranium-doped thoria and uranium adatoms on the major surfaces of thorium dioxide * Ashley E. Shields a, David Santos-Carballal b, Nora H. de Leeuw a, b, a Department of Chemistry, University College London, 20 Gordon Street, London WC1H 0AJ, UK b School of Chemistry, Cardiff University, Main Building, Park Place, Cardiff CF10 3AT, UK highlights Uranium substitution in ThO2 is found to increase the covalent nature of the ionic bonding. The (111), (110), and (100) surfaces of ThO2 are studied and the particle morphology is proposed. STM images of the (111), (110), and (100) surfaces of ThO2 are simulated. Uranium adsorption on the major surfaces of ThO2 is studied. article info abstract Article history: Thorium dioxide is of significant research interest for its use as a nuclear fuel, particularly as part of Received 23 November 2015 mixed oxide fuels. We present the results of a density functional theory (DFT) study of uranium- Received in revised form substituted thorium dioxide, where we found that increasing levels of uranium substitution increases 12 February 2016 the covalent nature of the bonding in the bulk ThO crystal. Three low Miller index surfaces have been Accepted 21 February 2016 2 simulated and we propose the Wulff morphology for a ThO particle and STM images for the (100), (110), Available online 23 February 2016 2 and (111) surfaces studied in this work. We have also calculated the adsorption of a uranium atom and the U adatom is found to absorb strongly on all three surfaces, with particular preference for the less stable (100) and (110) surfaces, thus providing a route to the incorporation of uranium into a growing thoria particle. -

EVALUATION of THORIUM BASED NUCLEAR FUEL Chemical Aspects
JULY 1995 ECN-R--95-007 A / energy innovation EVALUATION OF THORIUM BASED NUCLEAR FUEL Chemical Aspects R.J.M. KONINGS PJ.A.M.BLANKENVOORDE E.H.P.CORDFÜNKE K. BAKKER VOL 2 7 K \ 0 The Netherlands Energy Research Foundation ECN Het Energieonderzoek Centrum Nederland (ECN) is is the leading institute in the Netherlands for energy het centrale instituut voor onderzoek op energie- research. ECN carries out basic and applied research gebied in Nederland. ECN verricht fundamenteel en in the fields of nuclear energy, fossil fuels, renewable toegepast onderzoek op het gebied van kernenergie, energy sources, policy studies, environmental aspects fossiele-energiedragers, duurzame energie, beleids- ofenergy supply and the development and application studies, milieuaspecten van de energievoorziening en of new materials. de ontwikkeling en toepassing van nieuwe materialen. ECN employs more than 800 staff. Contracts are Bij ECN zijn ruim 800 medewerkers werkzaam. De obtained from the government and from national and opdrachten worden verkregen van de overheid en van foreign organizations and industries. organisaties en industrieën uit binnen- en buitenland. ECN's research results are published in a number of De resultaten van het ECN-onderzoek worden neer- report series, each series serving a different public, gelegd in diverse rapportenseries, bestemd voor ver- from contractors to the international scientific world. schillende doelgroepen, van opdrachtgevers tot de internationale wetenschappelijke wereld. The R-series is for research reports that make the results of ECN research available to the international De R-serie is de serie research-rapporten die de technical and scientific world. resultaten van ECN-onderzoek toegankelijk maken voor de internationale technisch-wetenschappelijke wereld.