Final Covid-19 Update No. 2 Ds.Sq .Ds Who Ds 002.Sq Ds.Pdf (English)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

S/PV.8734 the Situation in the Middle East 27/02/2020
United Nations S/ PV.8734 Security Council Provisional Seventy-fifth year 8734th meeting Thursday, 27 February 2020, 10 a.m. New York President: Mr. De Croo ................................... (Belgium) Members: China ......................................... Mr. Wu Haitao Dominican Republic ............................. Mrs. Cedano Estonia ........................................ Mr. Jürgenson France ........................................ Mr. De Rivière Germany ...................................... Mr. Maas Indonesia. Mr. Syihab Niger ......................................... Mr. Abarry Russian Federation ............................... Mr. Nebenzia Saint Vincent and the Grenadines ................... Ms. Prince South Africa ................................... Ms. Goolab Tunisia ........................................ Mr. Ladeb United Kingdom of Great Britain and Northern Ireland .. Mr. Allen United States of America .......................... Mrs. Craft Viet Nam ...................................... Mr. Dang Agenda The situation in the Middle East Report of the Secretary-General on the review of alternative modalities for the border crossing of Ya‘rubiyah (S/2020/139) Report of the Secretary-General on the implementation of Security Council resolutions 2139 (2014), 2165 (2014), 2191 (2014), 2258 (2015), 2332 (2016), 2393 (2017), 2401(2018), 2449 (2018) and 2504 (2020) (S/2020/141) This record contains the text of speeches delivered in English and of the translation of speeches delivered in other languages. The final text will be -

The PYD's Precarious Rise in Syria
Flight of Icarus? The PYD’s Precarious Rise in Syria Middle East Report N°151 | 8 May 2014 International Crisis Group Headquarters Avenue Louise 149 1050 Brussels, Belgium Tel: +32 2 502 90 38 Fax: +32 2 502 50 38 [email protected] Table of Contents Executive Summary ................................................................................................................... i I. Introduction ..................................................................................................................... 1 II. An Opportunity Grasped .................................................................................................. 4 A. The PKK Returns to Syria .......................................................................................... 4 B. An Unspoken Alliance? .............................................................................................. 7 C. Brothers and Rivals .................................................................................................... 10 III. From Fighters to Rulers ................................................................................................... 12 A. The Rojava Project ..................................................................................................... 12 B. In Need of Protection ................................................................................................. 16 IV. Messy Geopolitics ............................................................................................................. 18 A. Turkey and -
Regime and Allies: November 9, 2015
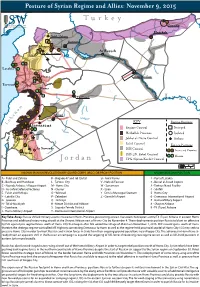
Posture of Syrian Regime and Allies: November 9, 2015 Turkey Z Qamishli Hasakah Nubl / Zahraa A Kuweires Aleppo B E C D Ar Raqqah Fu’ah / Kefraya Idlib 4 1 F G Latakia 2 H I J Hama Deir ez-Zor 3 7 K Tartous L Homs 5 M S 9 Y R I A N 8 T4 (Tiyas) Iraq n o n O a Sayqal b P e KEY Regime Positions L Q R Damascus S T 6 Regime Control Besieged U V Hezbollah Presence Isolated W Quneitra Jabhat al-Nusra Control Airbase l Rebel Control e X Foreign Positions a r As Suwayda ISIS Control s Y A B Iran and Proxies I Deraa ISIS, JN, Rebel Control 1 2 Russia Jordan YPG (Syrian Kurds) Control 10 mi 20 km KNOWN IRANIAN REVOLUTIONARY GUARD CORPS (IRGC) OR PROXY POSITION KNOWN RUSSIAN POSITION A - Nubl and Zahraa K - Brigade 47 and Tel Qartal U - Amal Farms 1 - Port of Latakia B - Bashkuy and Handarat L - Tartous City V - Nabi al-Fawwar 2 - Bassel al-Assad Airport C - Neyrab Airbase / Aleppo Airport M - Homs City W - Sanamayn 3 - Tartous Naval Facility D - As-Sara Defense Factories N - Qusayr X - Izraa 4 - Slinfah E - Fu’ah and Kefraya O - Yabroud Y - Dera’a Municipal Stadium 5 - Homs City F - Latakia City P - Zabadani Z - Qamishli Airport 6 - Damascus International Airport G - Joureen Q - Jamraya 7 - Hama Military Airport H - Tel al-Nasiriyah R - Mezze District and Airbase 8 - Shayrat Airbase I - Qumhana S - Sayyida Zeinab District 9 - T4 (Tiyas) Airbase J - Hama Military Airport T - Damascus International Airport Key Take-Away: Russia shifted military assets into eastern Homs Province, positioning at least ve attack helicopters at the T4 (Tiyas) Airbase in eastern Homs Province and additional rotary-wing aircraft at the Shayrat Airbase east of Homs City by November 4. -

Erkenntnismittelliste Syrien
VERWALTUNGSGERICHT STADE Verzeichnis der vorhandenen Materialien über die Arabische Republik Syrien - 10. Kammer - Stand: 16.09.2021 --------------------------------------------------------------------------------------------------------------------- Das Gericht beabsichtigt, gemäß § 86 VwGO die genannten Materialien gegebenenfalls zur Entscheidung heranzuziehen. Falls Sie Einsicht in ein nicht frei verfügbares Erkenntnismit- tel benötigen, wenden Sie sich bitte an die Service-Einheit der 10. Kammer. I. Auswärtiges Amt A. Lageberichte 01.04.2004 13.12.2004 14.07.2005 17.03.2006 26.02.2007 05.05.2008 09.07.2009 28.12.2009 (Ad-hoc Ergänzungsbericht) 07.04.2010 (Ad-hoc Ergänzungsbericht) 27.09.2010 17.02.2012 (Ad-hoc-Bericht) 13.11.2018 Stand: November 2018 kein regulärer Asyllagebericht; Er- stellung im Hinblick auf die IMK im November 2018 20.11.2019 Stand: November 2019 kein regulärer Asyllagebericht; Er- stellung im Hinblick auf die IMK im Dezember 2019 19.05.2020 Fortschreibung des Berichts über die Lage in der Arabischen Republik Sy- rien vom November 2019 (Stand: Mai 2020), kein regulärer Asyllage- bericht; Erstellung im Hinblick auf die IMK im Juni 2020 04.12.2020 Bericht über die Lage in der Arabischen Republik Syrien (Stand: November 2020), kein regulärer Asyllagebericht; Erstellung im Hin- blick auf die IMK im Dezember 2020 - 2 - B. Auskünfte Datum Adressat Inhalt 14.01.2004 VG Darmstadt staatenlose Kurden; rot-orange- nes Plastikdokument; Wehr- dienst 14.01.2004 VG Darmstadt staatenlose Kurden; Ausweispa- piere; Bescheinigung des Orts- vorstehers; rot-orangene Plas- tikkarte; Maktumin 14.01.2004 VG Darmstadt Echtheit Personaldokument - Wehrdienst staatenloser Kurden 19.01.2004 VG Darmstadt Identitätsbescheinigung eines Mukhtars; geringer Beweiswert 19.01.2004 VG Bayreuth Identitätsbescheinigung; Volkszäh- lung 1962; rot-orangene Plastikkar- ten 04.03.2004 VG Braunschweig Ehrenmorde; Familienehre; Az. -
The PYD's Separatist Project
The PYD’s Separatist Project in the Syrian Euphrates Region Abdullah Al-Najjar Political research Hermon Center for Contemporary Studies is a non-profit organization, focused mainly on producing studies and research on the Syrian situation, implementing and managing projects, activities and initiatives to rebuild Syria on the foundations of democracy, freedom, social justice, human rights, human dignity and equal citizenship values. For Contacts: e-mail: [email protected] Harmoon Center For Contemporary Studies The PYD’s Separatist Project in the Syrian Euphrates Region January 2020 Abdullah Al-Najjar Authors This study was conducted by Abdullah Al-Najjar, with the help of former col- leagues and acquaintances who assisted him in collecting and verifying the infor- mation. Three of them had submitted three background papers: two on education, and one on the oil issue. In light of the positions of these individuals where they live, we will not be disclosing their names, but would like to thank them very much. Abdullah Al-Najjar is a former officer at the Political Security Directorate, with a degree in law. He worked in Hasakeh Province for 12 years, including nine and a half years in Qamishli district, as an assistant and head of the Qamishli police station, and head of the Amuda police station. He defected from the Political Se- curity Directorate in 2012 with the rank of major. He currently works in the field of studies and research related to east of the Euphrates, and on issues related to security and the military. Harmoon Center For Contemporary -

SYRIA CRISIS WATCH International Strategic Studies Group (08-22 Dec 19)
© 2019 Beyond the Horizon SYRIA CRISIS WATCH International Strategic Studies Group (08-22 Dec 19) www.behorizon.org 6. At least 25,000 people fled Syria's Idlib for Turkey over two days - media. KEY EVENTS 22.12.2019 At least 25,000 civilians have fled Syria’s northwestern region of Idlib and headed towards Turkey over the past two days, Turkish state media said on Sunday, as Syrian and 1. Russian Military Opened Fire on an Israeli Aircraft. Russian forces intensified their bombardment of the region. Syrian President Bashar al-Assad has 19.12.2019 Russia has allegedly opened fire on Israeli aircraft that entered Syria’s airspace vowed to recapture Idlib, pushing more people towards Turkey. On Thursday, Turkish President in the southwestern part of the country, the Hebrew-language website Channel 12 Tayyip Erdogan said 50,000 people were fleeing from Idlib towards Syria’s border with Turkey. reported. Citing the website Top War, the Channel 12 report said the Russian military (Reuters) https://reut.rs/36YWBIB opened fire on an Israeli unmanned aerial vehicle (UAV) that was along the eastern axis of the occupied Golan Heights region. (The Syrian Observer) http://bit.ly/2PLSM3E 7. Lack of refugee aid forced Turkey into Syria operation : Erdogan. 17.12.2019 A lack of international assistance to Turkey to support millions of refugees on its soil 2. Russia & Syria Signal West With Joint Naval Drills, “Hundreds” Of Airstrikes pushed Ankara to launch operations in northeast Syria, Turkish President Recep Tayyip Erdogan On Idlib. said Tuesday. Despite broad international criticism, Turkish forces in October launched a major 22.12.2019 Multiple developments related to Russia's military role in Syria mean that the cross-border raid to clear a so-called safe-zone of Kurdish fighters, who Ankara considers years-long conflict could once again become front and center for Washington during 2020. -

Syria COI Meeting Report November 2017
European Asylum Support Office EASO COI Meeting Report Syria 30 November & 1 December 2017 Valletta, Malta March 2018 SUPPORT IS OUR MISSION European Asylum Support Office EASO COI Meeting Report Syria 30 November & 1 December 2017 Valletta, Malta March 2018 Europe Direct is a service to help you find answers to your questions about the European Union. Freephone number (*): 00 800 6 7 8 9 10 11 (*) Certain mobile telephone operators do not allow access to 00800 numbers or these calls may be billed. More information on the European Union is available on the Internet (http://europa.eu). © European Asylum Support Office 2018 Reproduction is authorised, provided the source is acknowledged, unless otherwise stated. For third-party materials reproduced in this publication, reference is made to the copyrights statements of the respective third parties. Cover photo: © Shelly Kittleson, Destroyed parts of Aleppo, 2015 Neither EASO nor any person acting on its behalf may be held responsible for the use which may be made of the information contained herein. EASO COI MEETING REPORT - SYRIA: COI MEETING 30 NOVEMBER-1 DECEMBER 2017 — 3 Acknowledgements EASO would like to acknowledge the members of the EASO COI Specialist Network on Syria for their active contributions and participation. EASO would also like to thank the following external experts and organisations for their presentations: Christopher Kozak, Institute for the Study of War Esther van Eijk, Maastricht University Fabrice Balanche, University of Lyon 2 and Hoover Institution, Stanford University UNHCR 4 — EASO COI MEETING REPORT - SYRIA: COI MEETING 30 NOVEMBER-1 DECEMBER 2017 Table of Contents Acknowledgements .................................................................................................................. -
Kurdish Self-Governance in Syria: Survival and Ambition
Research Paper Ghadi Sary Middle East and North Africa Programme | September 2016 Kurdish Self-governance in Syria: Survival and Ambition EMBARGOED UNTIL 15 SEPTEMBER 2016 EMBARGOED UNTIL 15 SEPTEMBER 2016 Contents Summary 2 1 Introduction 3 2 Syria’s Kurds Before 2011 6 3 2011: The Syrian Uprising and the Kurds’ Decisive Moment 7 4 Beyond Security: Local Administration in Rojava 11 5 Rojava and Damascus: Decentralization or a Marriage of Convenience? 15 6 Conclusion: Rojava, Limiting the Threat of Ambition 19 Acronyms 21 About the Author 22 Acknowledgments 23 1 | Chatham House Kurdish Self-governance in Syria: Survival and Ambition EMBARGOED UNTIL 15 SEPTEMBER 2016 Summary • Syria’s Kurds have emerged at the forefront of the battle with self-styled Islamic State of Iraq and Syria (ISIS), gaining them support from the United States even as tensions between them and the Syrian opposition have increased. Their strategic gains have been significant, but remain fragile. • Ideological and tactical divisions between Syrian Kurdish political movements have manifested in their response to the Syrian uprising. The ascension to power of the Democratic Union Party (PYD) signalled a pragmatic approach in which tacit agreements with the regime have been sought in order to obtain greater autonomy from the central government. • The Syrian opposition has consequently criticized the PYD as no more than a regime proxy. But the reality is more complex. The PYD’s relationship with the regime should be seen as an ambitious survival strategy adopted in the circumstances of the Syrian civil war. • The PYD’s local legitimacy, while not uncontested, stems from its success in combating ISIS and its ability to deliver a localized form of governance. -
SYRIAN ARAB REPUBLIC COVID-19 Response Update No.03 As of 13 May 2020
SYRIAN ARAB REPUBLIC COVID-19 Response Update No.03 As of 13 May 2020 47 total confirmed cases Active cases 15 29 Recovered 3 Deaths Source: Syrian Ministry of Health (MoH) *MoH data does not include areas outside of GoS control This report is produced by the World Health Organization (WHO) and the Office for the Coordination of Humanitarian Affairs (OCHA), in collaboration with humanitarian partners. The next report will be issued on or around 18 May 2020. HIGHLIGHTS • The Syrian Ministry of Health (MoH) confirmed 47 people with COVID-19, including three people who died and 29 who recovered, as of 10 May. • As of 10 May, six people with COVID-19 were reported in north-east Syria (NES), including one death. Lack of a common reporting approach creates challenges in verifying/triangulating information on reported/suspected cases. • In north-west Syria (NWS), no laboratory confirmed cases of COVID-19 have been reported as of 10 May. • COVID-19 testing has now commenced at laboratories in Aleppo and Lattakia governorates. • Areas of concern: Densely populated areas, notably Damascus/Rural Damascus, Aleppo and Homs, and those living in camps and informal settlements in NES and NWS, as well as collective shelters throughout the country • As of 11 May, WHO managed to deliver a 30-ton medical shipment by road to Al Qamishli in NES as a part of its response to the emergency health needs, including COVID-19, The delivered supplies contained ICU beds, ventilators, X-Rays machines and other vital medical equipment needed for case management • The enhancement of laboratory and case investigation capacity across Syria, including training of laboratory technicians and rapid response teams (RRTs) remains a priority, as does the timely communication of all information relevant to the safeguarding of public health. -

Syria Conflict (RAS) Is Now Produced Quarterly, Replacing 3.7 Deir-Ez-Zor the Monthly RAS of 2013
1. OVERVIEW 1.1 Executive Summary 1.2 Timeline Q3 1.3 Armed conflict and possible developments 1.4 Humanitarian Population Profile 1.5 Displacement profile 1.6 Humanitarian Access 1.7 Possible developments 1.8 Data sources and limitations REGIONAL 2. COUNTRYWIDE SECTORAL ANALYSIS 2.1 Protection 2.2 WASH 2.3 Livelihoods and Food Security 2.4 Shelter NFI ANALYSIS 2.5 Health 2.6 Education 3. GOVERNORATE PROFILES 3.1 Aleppo 3.2 Al-Hasakeh 3.3 Ar-Raqqa 3.4 As-Sweida Q3 2014 | 13 OCTOBER 2014 3.5 Damascus/Rural Damascus 3.6 Dar’a This Regional Analysis of the Syria conflict (RAS) is now produced quarterly, replacing 3.7 Deir-ez-Zor the monthly RAS of 2013. It seeks to bring together information from all sources in 3.8 Lattakia the region and provide holistic analysis of the overall Syria crisis. While Part I focuses on the situation within Syria, Part II covers the impact of the crisis on neighbouring 3.9 Hama countries. More information on how to use this document can be found on page 2. 3.10 Homs Please note that place names which are underlined are hyperlinked to their location 3.11 Idleb on Google Maps. The Syria Needs Analysis Project welcomes all information that could 3.12 Quneitra complement this report. For more information, comments or questions please email 3.13 Tartous [email protected]. 1. OVERVIEW 1.1 Executive Summary 1.2 Possible Developments 1.3 Timeline Q3 1.4 Humanitarian Population Profile 2. COUNTRIES 2.1 Lebanon 2.2 Jordan 2.3 Turkey 2.4 Iraq 2.5 Egypt ANNEX 1. -

Rojava Seeks to Break out in Syria | the Washington Institute
MENU Policy Analysis / PolicyWatch 2784 Rojava Seeks to Break Out in Syria by Fabrice Balanche Apr 12, 2017 Also available in Arabic ABOUT THE AUTHORS Fabrice Balanche Fabrice Balanche, an associate professor and research director at the University of Lyon 2, is an adjunct fellow at The Washington Institute. Brief Analysis Despite their desire for greater independence, Syria's Kurds have shown a willingness to broker agreements with the Assad regime in order to secure their near-term economic interests, and they may soon do the same with Iran. N ote: Click on maps for high-resolution versions. In February, the Syrian army met up with the Kurdish-led Syrian Democratic Forces south of Manbij, a development that Kurdish authorities have characterized as a means of linking the northwestern canton of Afrin with the rest of their territorial bloc along the Syria-Turkey border. The Democratic Union Party (PYD), the Kurdish militia that dominates the SDF, would have preferred to control this link with its own troops rather than relying on the Assad regime, but recent Turkish operations blocked its westward march. Even so, the situation gives the Syrian Kurds of Rojava another means of preventing other actors from boxing them in politically or economically, at least for now. ROJAVA STILL BELONGS TO SYRIA'S ECONOMIC SPACE Although the latest developments will facilitate the circulation of goods between Afrin and the rest of Rojava, any such movement is still subject to the regime's goodwill. Fortunately for the PYD, Bashar al-Assad has a mutual interest in expanding economic relations with the Kurds. -

Relevant Country of Origin Information to Assist with the Application Of
Relevant Country of Origin Information to Assist with the Application of UNHCR’s Country Guidance on Syria Participation in Anti-Government Protests; Draft Evasion; Issuance and Application of Partial Amnesty Decrees; Residency in (Formerly) Opposition-Held Areas; Issuance of Passports Abroad; Return and “Settling One’s Status” 7 May 2020 1. Participation in Anti-Government Protests ................................................................ 4 2. Draft Evasion ............................................................................................................... 8 3. Issuance and Application of Partial Amnesty Decrees ............................................ 11 4. Residency in (Formerly) Opposition-Held Areas ..................................................... 12 5. Issuance of National Passports Abroad ................................................................... 19 6. Possible Consequences of Illegal Exit ..................................................................... 20 7. Return and “Settling One’s Status” .......................................................................... 21 The International Protection Considerations (Update V) provide UNHCR’s guidance on the international protection needs of asylum-seekers from Syria.1 The present document provides relevant and up-to-date additional country of origin information (COI) relating to specific risk profiles and issues to assist decision-makers in asylum procedures with the application of the guidance provided by UNHCR in the International Protection