Eosinophilic Gastroenteritis Presenting with Severe Anemia and Near Syncope
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Section 8: Hematology CHAPTER 47: ANEMIA
Section 8: Hematology CHAPTER 47: ANEMIA Q.1. A 56-year-old man presents with symptoms of severe dyspnea on exertion and fatigue. His laboratory values are as follows: Hemoglobin 6.0 g/dL (normal: 12–15 g/dL) Hematocrit 18% (normal: 36%–46%) RBC count 2 million/L (normal: 4–5.2 million/L) Reticulocyte count 3% (normal: 0.5%–1.5%) Which of the following caused this man’s anemia? A. Decreased red cell production B. Increased red cell destruction C. Acute blood loss (hemorrhage) D. There is insufficient information to make a determination Answer: A. This man presents with anemia and an elevated reticulocyte count which seems to suggest a hemolytic process. His reticulocyte count, however, has not been corrected for the degree of anemia he displays. This can be done by calculating his corrected reticulocyte count ([3% × (18%/45%)] = 1.2%), which is less than 2 and thus suggestive of a hypoproliferative process (decreased red cell production). Q.2. A 25-year-old man with pancytopenia undergoes bone marrow aspiration and biopsy, which reveals profound hypocellularity and virtual absence of hematopoietic cells. Cytogenetic analysis of the bone marrow does not reveal any abnormalities. Despite red blood cell and platelet transfusions, his pancytopenia worsens. Histocompatibility testing of his only sister fails to reveal a match. What would be the most appropriate course of therapy? A. Antithymocyte globulin, cyclosporine, and prednisone B. Prednisone alone C. Supportive therapy with chronic blood and platelet transfusions only D. Methotrexate and prednisone E. Bone marrow transplant Answer: A. Although supportive care with transfusions is necessary for treating this patient with aplastic anemia, most cases are not self-limited. -

A Distant Gene Deletion Affects Beta-Globin Gene Function in an Atypical Gamma Delta Beta-Thalassemia
A distant gene deletion affects beta-globin gene function in an atypical gamma delta beta-thalassemia. P Curtin, … , A D Stephens, H Lehmann J Clin Invest. 1985;76(4):1554-1558. https://doi.org/10.1172/JCI112136. Research Article We describe an English family with an atypical gamma delta beta-thalassemia syndrome. Heterozygosity results in a beta-thalassemia phenotype with normal hemoglobin A2. However, unlike previously described cases, no history of neonatal hemolytic anemia requiring blood transfusion was obtained. Gene mapping showed a deletion that extended from the third exon of the G gamma-globin gene upstream for approximately 100 kilobases (kb). The A gamma-globin, psi beta-, delta-, and beta-globin genes in cis remained intact. The malfunction of the beta-globin gene on a chromosome in which the deletion is located 25 kb away suggests that chromatin structure and conformation are important for globin gene expression. Find the latest version: https://jci.me/112136/pdf A Distant Gene Deletion Affects ,8-Globin Gene Function in an Atypical '6y5-Thalassemia Peter Curtin, Mario Pirastu, and Yuet Wai Kan Howard Hughes Medical Institute and Department ofMedicine, University of California, San Francisco, California 94143 John Anderson Gobert-Jones Department ofPathology, West Suffolk County Hospital, Bury St. Edmunds IP33-2QZ, Suffolk, England Adrian David Stephens Department ofHaematology, St. Bartholomew's Hospital, London ECIA-7BE, England Herman Lehmann Department ofBiochemistry, University ofCambridge, Cambridge CB2-lQW, England Abstract tologic picture of f3-thalassemia minor in adult life. Globin syn- thetic studies reveal a ,3 to a ratio of -0.5, but unlike the usual We describe an English family with an atypical 'yS6-thalassemia fl-thalassemia heterozygote, the levels of HbA2 (and HbF) are syndrome. -

Anemia in Heart Failure - from Guidelines to Controversies and Challenges
52 Education Anemia in heart failure - from guidelines to controversies and challenges Oana Sîrbu1,*, Mariana Floria1,*, Petru Dascalita*, Alexandra Stoica1,*, Paula Adascalitei, Victorita Sorodoc1,*, Laurentiu Sorodoc1,* *Grigore T. Popa University of Medicine and Pharmacy; Iasi-Romania 1Sf. Spiridon Emergency Hospital; Iasi-Romania ABSTRACT Anemia associated with heart failure is a frequent condition, which may lead to heart function deterioration by the activation of neuro-hormonal mechanisms. Therefore, a vicious circle is present in the relationship of heart failure and anemia. The consequence is reflected upon the pa- tients’ survival, quality of life, and hospital readmissions. Anemia and iron deficiency should be correctly diagnosed and treated in patients with heart failure. The etiology is multifactorial but certainly not fully understood. There is data suggesting that the following factors can cause ane- mia alone or in combination: iron deficiency, inflammation, erythropoietin levels, prescribed medication, hemodilution, and medullar dysfunc- tion. There is data suggesting the association among iron deficiency, inflammation, erythropoietin levels, prescribed medication, hemodilution, and medullar dysfunction. The main pathophysiologic mechanisms, with the strongest evidence-based medicine data, are iron deficiency and inflammation. In clinical practice, the etiology of anemia needs thorough evaluation for determining the best possible therapeutic course. In this context, we must correctly treat the patients’ diseases; according with the current guidelines we have now only one intravenous iron drug. This paper is focused on data about anemia in heart failure, from prevalence to optimal treatment, controversies, and challenges. (Anatol J Cardiol 2018; 20: 52-9) Keywords: anemia, heart failure, intravenous iron, ferric carboxymaltose, quality of life Introduction g/dL in men) (2). -

Abdominal Pain - Gastroesophageal Reflux Disease
ACS/ASE Medical Student Core Curriculum Abdominal Pain - Gastroesophageal Reflux Disease ABDOMINAL PAIN - GASTROESOPHAGEAL REFLUX DISEASE Epidemiology and Pathophysiology Gastroesophageal reflux disease (GERD) is one of the most commonly encountered benign foregut disorders. Approximately 20-40% of adults in the United States experience chronic GERD symptoms, and these rates are rising rapidly. GERD is the most common gastrointestinal-related disorder that is managed in outpatient primary care clinics. GERD is defined as a condition which develops when stomach contents reflux into the esophagus causing bothersome symptoms and/or complications. Mechanical failure of the antireflux mechanism is considered the cause of GERD. Mechanical failure can be secondary to functional defects of the lower esophageal sphincter or anatomic defects that result from a hiatal or paraesophageal hernia. These defects can include widening of the diaphragmatic hiatus, disturbance of the angle of His, loss of the gastroesophageal flap valve, displacement of lower esophageal sphincter into the chest, and/or failure of the phrenoesophageal membrane. Symptoms, however, can be accentuated by a variety of factors including dietary habits, eating behaviors, obesity, pregnancy, medications, delayed gastric emptying, altered esophageal mucosal resistance, and/or impaired esophageal clearance. Signs and Symptoms Typical GERD symptoms include heartburn, regurgitation, dysphagia, excessive eructation, and epigastric pain. Patients can also present with extra-esophageal symptoms including cough, hoarse voice, sore throat, and/or globus. GERD can present with a wide spectrum of disease severity ranging from mild, intermittent symptoms to severe, daily symptoms with associated esophageal and/or airway damage. For example, severe GERD can contribute to shortness of breath, worsening asthma, and/or recurrent aspiration pneumonia. -

Gastroesophageal Reflux Disease (GERD)
Guidelines for Clinical Care Quality Department Ambulatory GERD Gastroesophageal Reflux Disease (GERD) Guideline Team Team Leader Patient population: Adults Joel J Heidelbaugh, MD Objective: To implement a cost-effective and evidence-based strategy for the diagnosis and Family Medicine treatment of gastroesophageal reflux disease (GERD). Team Members Key Points: R Van Harrison, PhD Diagnosis Learning Health Sciences Mark A McQuillan, MD History. If classic symptoms of heartburn and acid regurgitation dominate a patient’s history, then General Medicine they can help establish the diagnosis of GERD with sufficiently high specificity, although sensitivity Timothy T Nostrant, MD remains low compared to 24-hour pH monitoring. The presence of atypical symptoms (Table 1), Gastroenterology although common, cannot sufficiently support the clinical diagnosis of GERD [B*]. Testing. No gold standard exists for the diagnosis of GERD [A*]. Although 24-hour pH monitoring Initial Release is accepted as the standard with a sensitivity of 85% and specificity of 95%, false positives and false March 2002 negatives still exist [II B*]. Endoscopy lacks sensitivity in determining pathologic reflux but can Most Recent Major Update identify complications (eg, strictures, erosive esophagitis, Barrett’s esophagus) [I A]. Barium May 2012 radiography has limited usefulness in the diagnosis of GERD and is not recommended [III B*]. Content Reviewed Therapeutic trial. An empiric trial of anti-secretory therapy can identify patients with GERD who March 2018 lack alarm or warning symptoms (Table 2) [I A*] and may be helpful in the evaluation of those with atypical manifestations of GERD, specifically non-cardiac chest pain [II B*]. Treatment Ambulatory Clinical Lifestyle modifications. -

Gastroesophageal Reflux Disease
The new england journal of medicine clinical practice Gastroesophageal Reflux Disease Peter J. Kahrilas, M.D. This Journal feature begins with a case vignette highlighting a common clinical problem. Evidence supporting various strategies is then presented, followed by a review of formal guidelines, when they exist. The article ends with the author’s clinical recommendations. A 53-year-old man, who is otherwise healthy and has a 20-year history of occasional heartburn, reports having had worsening heartburn for the past 12 months, with daily symptoms that disturb his sleep. He reports having had no dysphagia, gastroin- testinal bleeding, or weight loss and in fact has recently gained 20 lb (9 kg). What would you advise regarding his evaluation and treatment? The Clinical Problem From the Division of Gastroenterology, Gastroesophageal reflux disease is the most common gastrointestinal diagnosis re- Feinberg School of Medicine, Chicago. Ad- corded during visits to outpatient clinics.1 In the United States, it is estimated that dress reprint requests to Dr. Kahrilas at the Feinberg School of Medicine, 676 St. Clair 14 to 20% of adults are affected, although such percentages are at best approxima- St., Suite 1400, Chicago, IL 60611-2951, tions, given that the disease has a nebulous definition and that such estimates are or at [email protected]. based on the prevalence of self-reported chronic heartburn.2 A current definition of N Engl J Med 2008;359:1700-7. the disorder is “a condition which develops when the ref lux of stomach contents causes Copyright © 2008 Massachusetts Medical Society. troublesome symptoms (i.e., at least two heartburn episodes per week) and/or complications.”3 Several extraesophageal manifestations of the disease are well rec- ognized, including laryngitis and cough (Table 1). -

Alpha Thalassemia Trait
Alpha Thalassemia Trait Alpha Thalassemia Trait Produced by St. Jude Children’s Research Hospital, Departments of Hematology, Patient Education, 1 and Biomedical Communications. Funds were provided by St. Jude Children’s Research Hospital, ALSAC, and a grant from the Plough Foundation. This document is not intended to replace counseling by a trained health care professional or genetic counselor. Our aim is to promote active participation in your care and treatment by providing information and education. Questions about individual health concerns or specific treatment options should be discussed with your doctor. For general information on sickle cell disease and other blood disorders, please visit our Web site at www.stjude.org/sicklecell. Copyright © 2009 St. Jude Children’s Research Hospital Alpha thalassemia trait All red blood cells contain hemoglobin (HEE muh glow bin), which carries oxygen from your lungs to all parts of your body. Alpha thalassemia (thal uh SEE mee uh) trait is a condition that affects the amount of hemo- globin in the red blood cells. • Adult hemoglobin (hemoglobin A) is made of alpha and beta globins. • Normally, people have 4 genes for alpha globin with 2 genes on each chromosome (aa/aa). People with alpha thalassemia trait only have 2 genes for alpha globin, so their bodies make slightly less hemoglobin than normal. This trait was passed on from their parents, like hair color or eye color. A trait is different from a disease 2 Alpha thalassemia trait is not a disease. Normally, a trait will not make you sick. Parents who have alpha thalassemia trait can pass it on to their children. -

Hematology Unit Lab 1 Review Material
Hematology Unit Lab 1 Review Material Objectives Laboratory instructors: 1. Facilitate lab discussion and answer questions Students: 1. Review the introductory material below 2. Study and review the assigned cases and questions in small groups before the Lab. This includes the pathological material using Virtual Microscopy 3. Be prepared to present your cases, questions and answers to the rest of your Lab class during the Lab Erythropoiesis: The process of red blood cell (RBC) production • Characterized by: − Increasing hemoglobin synthesis Erythroid maturation stages (Below): − Decreasing cell size - Average of 4 cell divisions during maturation − Decreasing cytoplasmic basophilia [One pronormoblast gives rise to 16 red cells] (increasing pink color) - pronormoblast → reticulocyte = 7 days − Progressive chromatin condensation of the - reticulocytes → mature RBC =1-2 days nuclei − Extrusion of nucleus (orthochromatic stage) − Extruded nuclei are subsequently phagocytized − Loss of mitotic capability after the early stage of polychromatophilic normoblast • Picture below: Erythroid progenitors (normoblasts) cluster around macrophages (arrows) in the bone marrow and spleen • Macrophages store iron • Iron is transferred from macrophages to erythroid precursor cells • Iron is used by normoblasts for hemoglobin synthesis aka nucleated rbc aka reticulocyte 1 Mature Red Blood Cell 7-8 microns; round / ovoid biconcave disc with orange-red cytoplasm, no RNA, no nucleus; survives ~120 days in circulation Classification of Anemia by Morphology 1. -
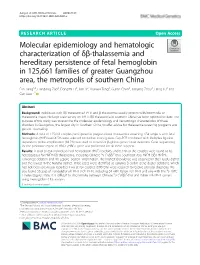
Molecular Epidemiology and Hematologic Characterization of Δβ
Jiang et al. BMC Medical Genetics (2020) 21:43 https://doi.org/10.1186/s12881-020-0981-x RESEARCH ARTICLE Open Access Molecular epidemiology and hematologic characterization of δβ-thalassemia and hereditary persistence of fetal hemoglobin in 125,661 families of greater Guangzhou area, the metropolis of southern China Fan Jiang1,2, Liandong Zuo2, Dongzhi Li2, Jian Li2, Xuewei Tang2, Guilan Chen2, Jianying Zhou2, Hang Lu2 and Can Liao1,2* Abstract Background: Individuals with δβ-thalassemia/HPFH and β-thalassemia usually present with intermedia or thalassemia major. No large-scale survey on HPFH/δβ-thalassemia in southern China has been reported to date. The purpose of this study was to examine the molecular epidemiology and hematologic characteristics of these disorders in Guangzhou, the largest city in Southern China, to offer advice for thalassemia screening programs and genetic counseling. Methods: A total of 125,661 couples participated in pregestational thalassemia screening. 654 subjects with fetal hemoglobin (HbF) level ≥ 5% were selected for further investigation. Gap-PCR combined with Multiplex ligation dependent probe amplification (MLPA) was used to screen for β-globin gene cluster deletions. Gene sequencing for the promoter region of HBG1 /HBG2 gene was performed for all those subjects. Results: A total of 654 individuals had hemoglobin (HbF) levels≥5, and 0.12% of the couples were found to be heterozygous for HPFH/δβ-thalassemia, including Chinese Gγ (Aγδβ)0-thal, Southeast Asia HPFH (SEA-HPFH), Taiwanese deletion and Hb Lepore–Boston–Washington. The highest prevalence was observed in the Huadu district and the lowest in the Nansha district. Three cases were identified as carrying β-globin gene cluster deletions, which had not been previously reported. -
Basics of Hematology and Patho-Histology
Basics of Hematology and Patho-histology Practical Course in Molecular Pathology Winter Term 2015 Ernst Müllner MFPL (Max F Perutz Laboratories) Department of Medical Biochemistry Medical University of Vienna [email protected] www.mfpl.ac.at/mfpl-group/group/muellner.html (Müllner homepage / research) E. coli + macrophages medicalschool.tumblr.com/post/43914024728/sem-image-of-e-coli-bacteria-and-macrophages medicalschool.tumblr.com/post/18256087351/r ed-blood-cells-erythrocytes-trapped-by-fibrin Overview on main white blood cell (WBC) types – (Wikipedia) Mature white blood cell types I White Blood cells (WBCs) are frequently also referred to as peripheral blood mononuclear cells (PBMCs). Granulocytes in general are part of the innate immune system. Names derive from staining with hematoxylin and eosin. Whereas basophils stain dark blue and eosinophils are bright red, neutrophils stain neutral to pink. Basophil granulocytes Eosinophil granulocytes Neutrophil granulocytes Least common granulocyte type About 1-6% of WBCs; component Most abundant WBC type (40- (0.01- 0.3% of WBCs. Large of innate immune system to com- 75%) and essential part of the cytoplasmic granules obscure the bat parasites and certain infec- innate immune system. A patho- nucleus under the microscope. tions; also associated with allergy gen is likely to first encounter a When unstained, the nucleus is and asthma. Following activation, neutrophil. Normally contain a nu- visible and usually has 2 lobes. eosinophils effector functions in- cleus of 2-5 lobes. Neutrophils Basophils appear in inflammatory clude production and release (de- quickly congregate at a infection reactions, particularly those granulation) of cytotoxic substan- site, attracted by cytokines from causing allergies, mainly via the ces (granule proteins, reactive activated endothelium, mast cells, vasodilator histamine (antihistami- oxygen species …) and production or macrophages. -

A Guide to Eosinophilic Esophagitis in Children and Adults
A GuideA toGuide Eosinophilic to Eosinophilic Esophagitis Esophagitisin Children in Children and Adultsand Adults What is Eosinophilic Esophagitis? Eosinophilic esophagitis (EoE) is an emerging disease related to food ingestion or aeroallergens. It is characterized by an isolated inflammation of the esophagus by a specific white blood cell the eosinophil. Several clinical symptoms can occur including difficulty swallowing, food becoming stuck in the esophagus, or symptoms of gastroesophageal reflux disease (GERD) such as vomiting, regurgitation, abdominal pain or heartburn. Uneffected individuals have no eosinophils in their esophagus while people with acid reflux may have a few esophageal eosinophils secondary to acid irritation. While other disorders such as parasitic disease and Crohn’s disease could potentially cause an esophageal eosinophilia, EoE is the most common cause of intense esophageal eosinophilia. What should you do if you believe that you or your child may have EoE? If you believe that either you or your child may have symptoms of EoE you should contact your primary physician, explain your concerns and ask for a referral to a gastroenterologist. An upper endoscopy with biopsy may need to be scheduled. A barium contrast study may also be useful in determining if the esophagus is narrowed or strictured. Where can you get additional information on EoE? The First International Gastrointestinal Eosinophilic Research Symposium brought together pediatric and adult experts from around the world to discuss the abundance of new information on EoE. The idea of The International Gastrointestinal Eosinophilic Research (TIGER) consortium was created. TIGER is currently in the process of understanding and assessing diagnostic techniques, treatments and treatment approaches for patients with EoE. -

Eosinophilic Gastrointestinal Disorders
Clinical Reviews in Allergy & Immunology (2019) 57:272–285 https://doi.org/10.1007/s12016-019-08732-1 Eosinophilic Gastrointestinal Disorders Nirmala Gonsalves1 Published online:22 March 2019 # Springer Science+Business Media, LLC, part of Springer Nature 2019 Abstract Eosinophilic gastrointestinal disorders (EGID) are a group of disorders characterized by pathologic eosinophilic infiltration of the esophagus, stomach, small intestine, or colon leading to organ dysfunction and clinical symptoms (J Pediatr Gastroenterol Nutr; Spergel et al., 52: 300–306, 2011). These disorders include eosinophilic esophagitis (EoE), eosinophilic gastritis (EG), eosino- philic gastroenteritis (EGE), eosinophilic enteritis (EE), and eosinophilic colitis (EC). Symptoms are dependent not only on the location (organ) as well as extent (layer invasion of the bowel wall). Common symptoms of EoE include dysphagia and food impaction in adults and heartburn, abdominal pain, and vomiting in children. Common symptoms of the other EGIDs include abdominal pain, nausea, vomiting, early satiety, diarrhea, and weight loss. These disorders are considered immune-mediated chronic inflammatory disorders with strong links to food allergen triggers. Treatment strategies focus on either medical or dietary therapy. These options include not only controlling symptoms and bowel inflammation but also on identifying potential food triggers. This chapter will focus on the clinical presentation, pathophysiology, and treatment of these increasingly recognized disorders. Keywords Eosinophilic gastroenteritis . Eosinophilic gastritis . Eosinophilic esophagitis . Dysphagia . Food impaction . Food allergy Introduction purpose of this chapter, we will discuss these disorders sepa- rately and focus on the available data on the clinical presenta- Eosinophilic gastrointestinal disorders (EGID) are a group of tion, pathophysiology, and treatment. disorders characterized by pathologic eosinophilic infiltration of the esophagus, stomach, small intestine, or colon leading to organ dysfunction and clinical symptoms [1].