SITREP#108 17Feb 2017Final
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Black Christs of the Black Christs of by J. Penn De
The Black Christs of Africa A Bible of Poems By J. Penn de Ngong Above all, I am not concerned with Poetry. My subject is War, and the pity of War. The Poetry is in the pity. Wilfred Owen, British Poet Poem 22 petition for partition We, the auto-government of the Republic of Ruralia, Voicing the will of the democratic public of Ruralia, Are writing to your Theocratic Union of Urbania. Our grievances are on the following discontentment: Firstly, your purely autocratic Government of Urbania, Has solely dishonoured and condemned the document That we all signed – and codenamed – “Bible of Peace”. You’ve violated its gospel, the cause of our fatal disagreement; Wealth: You’re feeding our autonomous nation with ration apiece. In your annual tour, compare our city – Metropollutant – of Ruralia With its posh sister city of Urbania, proudly dubbed Metropolitania. All our resources, on our watching, are consumed up in Urbania. Our intellectuals and workforce are abundant but redundant. Henceforth, right here, we demarcate to be independent! You are busy strategizing to turn Ruralia into Somalia: Yourselves landlords, creating warlords, tribal militia, And bribing our politicians to speak out your voice, And turning our villages into large ghettos of slum, And our own towns into large cities of Islam. With these experiences, we’ve no choice, But t’ ask, demand, fight... for our voice. They oft’ say the end justifies the means, We, Ruralians, must reform all our ruins; The first option: thru the ballot, Last action: bullet! J. Penn de Ngong (John Ngong Alwong Alith as known in his family) came into this world on a day nobody knows. -

South Sudan Village Assessment Survey
IOM DISPLACEMENT TRACKING MATRIX VILLAGE ASSESSMENT SURVEY SOUTH SUD AN IOM DISPLACEMENT TRACKING MATRIX SOUTH SUDAN SOUTH SUDAN VILLAGE ASSESSMENT SURVEY DATA COLLECTION: August-November 2019 COUNTIES: Bor South, Rubkona, Wau THEMATIC AREAS: Shelter and Land Ownership, Access and Communications, Livelihoods, Markets, Food Security and Coping Strategies, Health, WASH, Education, Protection 1 IOM DISPLACEMENT TRACKING MATRIX VILLAGE ASSESSMENT SURVEY SOUTH SUD AN CONTENTS RUBKONA COUNTY OVERVIEW 15 DISPLACEMENT DYNAMICS 15 RETURN PATTERNS 15 PAYAM CONTEXTUAL INFORMATION 16 KEY FINDINGS 17 Shelter and Land Ownership 17 EXECUTIVE SUMMARY 4 Access and Communications 17 LIST OF ACRONYMS 3 Markets, Food Security and Coping Strategies 17 EXECUTIVE SUMMARY 4 Livelihoods 18 BACKROUND 6 Health 19 WASH 19 METHODOLOGY 6 Education 20 LIMITATIONS 7 Protection 20 WAU COUNTY OVERVIEW 8 BOR SOUTH COUNTY OVERVIEW 21 DISPLACEMENT DYNAMICS 8 RETURN PATTERNS 8 DISPLACEMENT DYNAMICS 21 PAYAM CONTEXTUAL INFORMATION 9 RETURN PATTERNS 21 KEY FINDINGS 10 PAYAM CONTEXTUAL INFORMATION 22 KEY FINDINGS 23 Shelter and Land Ownership 10 Access and Communications 10 Shelter and Land Ownership 23 Markets, Food Security and Coping Strategies 10 Access and Communications 23 Livelihoods 11 Markets, Food Security and Coping Strategies 23 Health 12 Livelihoods 24 WASH 13 Health 25 Protection 13 Education 26 Education 14 WASH 27 Protection 27 2 3 IOM DISPLACEMENT TRACKING MATRIX VILLAGE ASSESSMENT SURVEY SOUTH SUD AN LIST OF ACRONYMS AIDS: Acquired Immunodeficiency Syndrome -
Jonglei State, South Sudan Introduction Key Findings
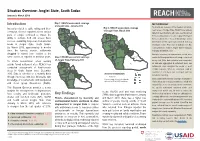
Situation Overview: Jonglei State, South Sudan January to March 2019 Introduction Map 1: REACH assessment coverage METHODOLOGY of Jonglei State, January 2019 To provide an overview of the situation in hard-to- Insecurity related to cattle raiding and inter- Map 3: REACH assessment coverage of Jonglei State, March 2019 reach areas of Jonglei State, REACH uses primary communal violence reported across various data from key informants who have recently arrived parts of Jonglei continued to impact the from, recently visited, or receive regular information ability to cultivate food and access basic Fangak Canal/Pigi from a settlement or “Area of Knowledge” (AoK). services, sustaining large-scale humanitarian Nyirol Information for this report was collected from key needs in Jonglei State, South Sudan. Ayod informants in Bor Protection of Civilians site, Bor By March 2019, approximately 5 months Town and Akobo Town in Jonglei State in January, since the harvest season, settlements February and March 2019. Akobo Duk Uror struggled to extend food rations to the In-depth interviews on humanitarian needs were Twic Pochalla same extent as reported in previous years. Map 2: REACH assessment coverage East conducted throughout the month using a structured of Jonglei State, February 2019 survey tool. After data collection was completed, To inform humanitarian actors working Bor South all data was aggregated at settlement level, and outside formal settlement sites, REACH has Pibor settlements were assigned the modal or most conducted assessments of hard-to-reach credible response. When no consensus could be areas in South Sudan since December found for a settlement, that settlement was not Assessed settlements 2015. -
SHELTER/NFI ANALYSIS REPORT - FLOOD RESPONSE Field with (*) and Italicized Questions Are Mandatory
Shelter Cluster South Sudan sheltersouthsudan.org Coordinating Humanitarian Shelter SHELTER/NFI ANALYSIS REPORT - FLOOD RESPONSE Field with (*) and italicized questions are mandatory. For checkboxes (☐), tick all that apply. Use charts from mobile data collection (MDC) wherever possible. 1. General Information Location* Jonglei, Bor South county- Jalle and Baidit Payams (State/County/Payam/Boma/Village) Alert Date* (first time the location 23rd September 2019 mentioned to the Cluster) Analysis Dates* 29/01/2020- 30/01/2020 2. Location Information Report Date* (date completed) 03/2/2020 GPS Coordinates* Jalle: Latitude N 06 o 40’ 11.64’’ Longitude: E 031 o 28’ 33.20’’ Baidit: Latitude N 06 o 29’ 38.58095’’ Longitude: E 031o 32’ 5.8957’’ Makuach Centre: Latitude N 06 o 13’ 18.97’’ Longitude: E 031 o 34’ 3.34’’ Type of settlement (PoC, informal Informal settlement camp, etc.) 3. Team Details* (Indicate the team leader) Name Organisation Title Contacts: Email/Mobile/Sat Phone Alex Kayidri Anthony PAH ES/NFIs Officer 0922791412/[email protected] Juma John Benjamin ACTED Senior Project Officer 0921268010/[email protected] Peter Mathiang HDC Field Assistant O916795955/[email protected] Jacob Mayom Yuot HDC Field Assistant 0924040077/[email protected] Did the team read the S/NFI project indicators? ☒ Yes ☐ No 4. Desk Research: Displacement, Movement, and Conflict Trends NOTE: TO BE CONDUCTED BEFORE DEPARTURE TO AFFECTED AREAS What information did you find about the context and trends in this location more than six months ago? What triggered the analysis? The analysis was triggered by the recent flooding which hit Bor South county and the surrounding payams including Jalle and Baidit. -

LOCATION: WFP Tukul Conference Room DATE: 25 September, 2014
SOUTH SUDAN FSL JONGLEI COORDINATION – MEETING MINUTES LOCATION: WFP Tukul Conference Room DATE: 25 September, 2014 CHAIR: George Mvula, FSL Area Cluster Coordinator AGENDA: The following was the agenda of the meeting: 1. Introductions; 2. Review and endorsing previous minutes; 3. Recap of the FSL Partners meeting; 4. Key challenges to humanitarian response interventions in Jonglei; 5. Partners’ presentation of county level information (planned versus actual) and where; 6. Presentation by SAADO on elevated Hunger Situation in Twic East; 7. Presentation by Oxfam Intermon on Urban Livelihood assessment in Bor Town; 8. Review of gaps per county; 9. Briefing on the IPC report September 2014 and implications on response programming; 10. AOB Monthly Updates from Partners Church and Development Key achievements in the month of September: Trained 150 women headed households on construction and usage of energy efficient stoves (Rocket Lorena model). Trained 300 fish folks (277 male, 03 female) on fish processing and preservation, this also involved construction of improved fish drying ovens using local materials. 60 households trained on village savings and loans association methodology and equipping them with startup kits. 400 beneficiaries from Bor Town registered and verified for unconditional cash transfer. http://foodsecuritycluster.net/operations/south-sudan SOUTH SUDAN FSL JONGLEI COORDINATION – MEETING MINUTES Plans for October 600 households in Bor targeted to receive ganny bags and assorted tools for construction of secondary dykes around their homesteads Cash transfer to verified 400 vulnerable households Post cash transfer assessment in Bor main market and other markets in the Payam. Catholic Relief Services (Jonglei Food Security Programme) General Food Distribution: CRS has been doing general food distributions in Bor and Twic East. -
SHELTER/NFI ANALYSIS REPORT - FLOOD RESPONSE Field with (*) and Italicized Questions Are Mandatory
Shelter Cluster South Sudan sheltersouthsudan.org Coordinating Humanitarian Shelter SHELTER/NFI ANALYSIS REPORT - FLOOD RESPONSE Field with (*) and italicized questions are mandatory. For checkboxes (☐), tick all that apply. Use charts from mobile data collection (MDC) wherever possible. 1. General Information Location* Jonglei, Bor South county- Jalle and Baidit Payams (State/County/Payam/Boma/Village) Alert Date* (first time the location 23rd September 2019 mentioned to the Cluster) Analysis Dates* 29/01/2020- 30/01/2020 2. Location Information Report Date* (date completed) 03/2/2020 GPS Coordinates* Jalle: Latitude N 06 o 40’ 11.64’’ Longitude: E 031 o 28’ 33.20’’ Baidit: Latitude N 06 o 29’ 38.58095’’ Longitude: E 031o 32’ 5.8957’’ Makuach Centre: Latitude N 06 o 13’ 18.97’’ Longitude: E 031 o 34’ 3.34’’ Type of settlement (PoC, informal Informal settlement camp, etc.) 3. Team Details* (Indicate the team leader) Name Organisation Title Contacts: Email/Mobile/Sat Phone Alex Kayidri Anthony PAH ES/NFIs Officer 0922791412/[email protected] Juma John Benjamin ACTED Senior Project Officer 0921268010/[email protected] Peter Mathiang HDC Field Assistant O916795955/[email protected] Jacob Mayom Yuot HDC Field Assistant 0924040077/[email protected] Did the team read the S/NFI project indicators? ☒ Yes ☐ No 4. Desk Research: Displacement, Movement, and Conflict Trends NOTE: TO BE CONDUCTED BEFORE DEPARTURE TO AFFECTED AREAS What information did you find about the context and trends in this location more than six months ago? What triggered the analysis? The analysis was triggered by the recent flooding which hit Bor South county and the surrounding payams including Jalle and Baidit. -

Cattle Rustling and Its Effects Among Three Communities (Dinka, Murle and Nuer) in Jonglei State, South Sudan Phillip T
Nova Southeastern University NSUWorks Department of Conflict Resolution Studies Theses CAHSS Theses and Dissertations and Dissertations 1-1-2017 Cattle Rustling and Its Effects among Three Communities (Dinka, Murle and Nuer) in Jonglei State, South Sudan Phillip T. Manyok Nova Southeastern University, [email protected] This document is a product of extensive research conducted at the Nova Southeastern University College of Arts, Humanities, and Social Sciences. For more information on research and degree programs at the NSU College of Arts, Humanities, and Social Sciences, please click here. Follow this and additional works at: https://nsuworks.nova.edu/shss_dcar_etd Part of the Social and Behavioral Sciences Commons Share Feedback About This Item NSUWorks Citation Phillip T. Manyok. 2017. Cattle Rustling and Its Effects among Three Communities (Dinka, Murle and Nuer) in Jonglei State, South Sudan. Doctoral dissertation. Nova Southeastern University. Retrieved from NSUWorks, College of Arts, Humanities and Social Sciences – Department of Conflict Resolution Studies. (62) https://nsuworks.nova.edu/shss_dcar_etd/62. This Dissertation is brought to you by the CAHSS Theses and Dissertations at NSUWorks. It has been accepted for inclusion in Department of Conflict Resolution Studies Theses and Dissertations by an authorized administrator of NSUWorks. For more information, please contact [email protected]. Cattle Rustling and Its Effects among Three Communities (Dinka, Murle and Nuer) in Jonglei State, South Sudan by Phillip Tor Manyok A Dissertation Presented to the College of Arts, Humanities, and Social Sciences of Nova Southeastern University in Partial Fulfillment of the Requirements for the Degree of Doctor of Philosophy Nova Southeastern University 2016 Acknowledgement I appreciate the effort made by my supervisor during the writing of this dissertation. -

IRNA Report: Jalle Payam - Jonglei State 10 February 2015
IRNA Report: Jalle payam - Jonglei state 10 February 2015 This IRNA Report is a product of Inter-Agency Assessment mission conducted and information compiled based on the inputs provided by partners on the ground including; government authorities, affected communities/IDPs and agencies. Situation overview The assessment team travelled by road from Bor town to Jalle Payam, Bor South County on 10 February 2015. The assessment was conducted the same day in Jalle Payam located north of Bor town (GPS N: 06˚ 40’ 11.51’’, N: 31˚28’ 34’’). The payam has a total of five payams with the population of 13.506 people as per 2008 census report, which is 7 % of the total population of the County (Bor South). The objectives of the assessment was to (i) provide an immediate and quick overview of the emergency situation in the area. (ii) to assess and determine the needs of the claimed community and estimâtes their number. (iii)Make initial rough estimates of the needs of the affected population and define the priorities for humanitarian action and; (iv) To identify aspects for which more detailed follow-on assessments, including cluster specific assessments, would be needed. On the ground the team met with boma chiefs of the affected areas, community leaders, représentatives from teachers, community health workers and représentatives from women, girls and youth groups. During the interviews it was noted that the community vividly recall the December 2013 violence which caused them to flee to the nearby islands and Mingkaman. 60 percent of the original population are reported to have returned in February and March of 2014, while the rest are still in Mingkaman. -

Facilities Types and Coverage Bor South County, Jonglei State December, 2019
Facilities Types and Coverage Bor South County, Jonglei State December, 2019 Akuai-deng Uror Jalle Mathiang Twic East Manydeng Baidit Baidit Makol-chuei Manydeng Makol-chuei Jalle Kapat Tong Jalle Makuach Bor town area Kuei-juet Yirol East Kapat Kapat Makuach Tuonygeau Makuach Pibor Gaak-yuom Ngatinag Werkok Mayen Ï ę Konbek Bor + £ Ï Anyidi Thianwei Ï Ï Ï Ï č Gaak-yuom Ï Ï Konbek £ Awerial £ Ï Ï Ï Arek + Tuonygeau Makuach Ï Ï Ï Ï Ï £ Ï Ï Ï Ï Ï Chuei-keer Ï Ï Ï Ï Arek Ï ÏÏ Ï Ï č Ï Kolnyang Ï ÏÏ Ï Ï Bor Pariak Ï Ï Ï£ Ï Thianwei Ï Anyidi BorÏ Ï ę Langbar Ï+ Ï Ï Ï Ï+ ÏÏ Terekeka Lafon Ï Mareng Ï Ï Anyidi Ï ¶£ Ï Mareng Ï Ï Pakua Coverage Boundaries Facilities Ï Ï £ Panapet ę ÏÏ ę £ę Adminstrative ¶ ÏÏ Bomas assessed Admin 2 County £ Ï Education £ Gak Chuei-magon Ïč Panapet Bomas not assessed Admin 3 Payam Healthcare JarwongÏÏ ę Waterways Admin 4 Boma Water Point ¶ £ +Ï Religious Roads Marshland £ ¶ £ Market ę Kolnyang Admin 1 State Waterbodies Transport + Ï Ï Bomas assessed £Ï vs not assessed Ï Number of facilities covered by types Awerial Awerial Ï + Ï Chuei-keer 60% Administrative Education Healthcare Market Religious Transport Water point Kolnyang Kolnyang Gak 40% 26 35 14 6 26 13 124 Ï + Ï Ï Pariak Assessed Not assessed ¶ Ï ę ¶ Kolnyang Pariak č Pariak Terekeka The boundaries on the map do not imply offcial endorsement or acceptance by the Government of the Republic of South Kilometers Data Source: IOM/DTM, National Bureau of Statistics, OCHA, Maxar, OpenStreetMap Sudan or by IOM. -

Conflict Trends, Issue 3 (2013)
IS S U E 3 , 2 0 1 3 Celebrating Nelson Mandela’s Legacy 20 YEARS OF CONTRIBUTING TO PEACE contents EDITORIAL 2 by Vasu Gounden FEATURES 3 The Other Side of Drones: Saving Wildlife in Africa and Managing Global Crime by Johan Bergenas, Rachel Stohl and Alexander Georgieff 10 At the Crossroads: Understanding Egypt’s Faltering Transition by Hazel Haddon 16 Rethinking the Tuareg Factor in the Mali Crisis by David Zounmenou 24 Inter-ethnic Conflict in South Sudan: A Challenge to Peace by Lukong Stella Shulika and Nwabufo Okeke-Uzodike 31 Exploring the Nexus between Ethnicity and Terrorism in Africa by Hussein Solomon 38 Celebrating Nelson Mandela’s Legacy: A Colloquium on Diversity, Cohesion and Integration by Buntu Siwisa 44 Gender Equality and Women’s Empowerment through Political Parties: Africa’s Record in Democracy-building by Victor Shale 50 Decentralising Liberia’s Security Sector: The Role of Non- governmental Actors in Justice and Security Delivery by Trine Nikolaisen COVeR piCTURe: ReUTeRS / THe BiGGeR piCTURe conflict trends I 1 editorial By vasu gounden “Syria has become the great tragedy of the century – weapons, including weapons of mass destruction and a disgraceful humanitarian calamity with suffering and chemical weapons. The human costs will be devastating displacement unparalleled in recent history.” These words and the financial costs to the region and global economy were spoken by António Guterres, the United Nations High will be high. Commissioner for Refugees (UNHCR). Guterres stated this This will not be the first time that the world will following the release of a UNHCR report indicating that the experience war with such devastating consequences. -

Download File
LESSONS LEARNED in ADDRESSING ACCESS to EDUCATION in SOUTH SUDAN Through Community Engagement, School Governance, Conflict Sensitivity, and Teacher Development ROOM TO LEARN SOUTH SUDAN Imlemente in artnerhi ith FHI36 an Plan International USA ROOM www.winrock.orgTO LEARN I www.fhi360.org SOUTH I www.planusa.org SUDAN Implemented in partnership with Plan International USA Contributors The Room to Learn Technical Reflection Paper was originally four separate papers: governance, grants, school development planning and teacher professional development. These have been integrated and examined through the lenses of community engagement and conflict sensitivity. Special thanks to the Room to Learn staff, field-based and home office, who made valuable contributions to this document from inception through revision stage. Contributors include: Iftikhar Ahmad Pascal Pax Andebo Katie Appel Margaret Ayite Alyssa Cochran Sora Edwards-Thro Sue Emmott Mark Ginsburg Valerie Haugen John Jalle Abdul Hakim Jumason Cube Caesar Kenji Emily Koester Francis Lokong James Natana Seth Ong’uti Zo Rakotomalala Martha Saldinger Mojeeb Stanikzai Joan Sullivan-Owomoyela Harriet Tino Katharine Torre DeGennaro Joshua Willis Kanju Yakuma This publication is made possible by the generous support of the American people through the United States Agency for International Development (USAID). The contents are the responsibility of Winrock International and do not necessarily reflect the views of USAID or the United States Government. Cover photo: Young girl stands in front -

Jonglei and Greater Pibor Administrative Area
Jonglei and Greater Pibor Administrative Area Humanitarian Update as of 8 December 2020 HIGHLIGHTS • Large-scale inter-communal and sub-national violence, mainly during the dry season, and massive flooding during the rainy season have displaced hundreds of thousands of people in Jonglei and Greater Pibor Administrative Area (GPAA) in 2019 and 2020. These recurrent shocks have created new humanitarian needs, in addition to those planned for in the 2020 Humanitarian Response Plan (HRP), which targets some 1 million people in the area. • More than 100 humanitarian organizations have operated in Jonglei during 2020. Half of them are national NGOs. • Conflict, insecurity, flooding and COVID-19 restrictions have severely impacted humanitarian organizations’ ability to reach the most vulnerable people with much-needed assistance. Of the nine humanitarian workers killed in 2020, eight lost their lives in Jonglei and GPAA. All were South Sudanese. • It is highly likely that sub-national conflict and flooding will occur again in Jonglei and GPAA in 2021 and lead to further displacement and an increase in people’s emergency needs, unless mitigating measures are taken to reduce their impact. Pariang Panyikang Maban Baliet Waves of violence anduair displacementPul Luthni e ana in February-July 2020 Rubkona Atar Kee UPPER NILE Longochuk Guit Atar Tor Fair Pauir d ana Wunam UAN Toch Canal/Pigi Fangak Nyadin Luakpiny/Nasir EHA Pail Maiwut Nyirol CAR Koch uturu Nyirol anda Ulang anien Par UNITY Haat 30,000+ displaced DRC Tonj Ku UA KENYA North ie in