Measurement of the Maxilla and Zygoma As an Aid in Installing
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Development of the Human Maxilla, Vomer, and Paraseptal Cartilages
THE DEVELOPMENT OF THE HUMAN MAXILLA, VOMER, AND PARASEPTAL CARTILAGES. By Professor FAWCETT, M.D., University of Bristol. THE usually accepted descriptions of the development of the maxilla of man state that it arises by a number of separate centres-the number varying somewhat with the authority, likewise the situation of these centres. No description of the maxilla can be considered complete unless at the same time notice is taken of the manner of development of the premaxilla, which, of course, forms the anterior segment of the adult bone as usually interpreted. But the consideration of the development of the premaxilla may be left until that of the maxilla has been fully dealt with. Before breaking new ground, it may be well to state what are the usual statements with reference to the ossification of the maxilla. These statements are apparently for the most part based on work done by Callender, Toldt, Rambaud and Renault, and Bland Sutton, so far as concerns human anatomy. More recently Franklin Mall has given his views on the subject in the American Jouarnal of Anatomy, views based on observation of specimens treated by the "clearing" method of Schulze. So far as they go, these statements are in harmony with my own notions, which I have for several years now taught. A very precise account is given in Cunningham's Text-book of Anatomy. The maxilla is there stated to be developed in the connective tissue around the oral cavity of the embryo from centres which are not preceded by cartilage, of uncertain number, as early fusion takes place between them. -

Morfofunctional Structure of the Skull
N.L. Svintsytska V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 Ministry of Public Health of Ukraine Public Institution «Central Methodological Office for Higher Medical Education of MPH of Ukraine» Higher State Educational Establishment of Ukraine «Ukranian Medical Stomatological Academy» N.L. Svintsytska, V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 2 LBC 28.706 UDC 611.714/716 S 24 «Recommended by the Ministry of Health of Ukraine as textbook for English- speaking students of higher educational institutions of the MPH of Ukraine» (minutes of the meeting of the Commission for the organization of training and methodical literature for the persons enrolled in higher medical (pharmaceutical) educational establishments of postgraduate education MPH of Ukraine, from 02.06.2016 №2). Letter of the MPH of Ukraine of 11.07.2016 № 08.01-30/17321 Composed by: N.L. Svintsytska, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor V.H. Hryn, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor This textbook is intended for undergraduate, postgraduate students and continuing education of health care professionals in a variety of clinical disciplines (medicine, pediatrics, dentistry) as it includes the basic concepts of human anatomy of the skull in adults and newborns. Rewiewed by: O.M. Slobodian, Head of the Department of Anatomy, Topographic Anatomy and Operative Surgery of Higher State Educational Establishment of Ukraine «Bukovinian State Medical University», Doctor of Medical Sciences, Professor M.V. -

MAXILLARY FRACTURES Is Mandatory and May Include Both Plain Films and a Computed Tomographic (CT) the Maxilla Forms the Largest Component of Scan
Radiographic evaluation of the fracture MAXILLARY FRACTURES is mandatory and may include both plain films and a computed tomographic (CT) The maxilla forms the largest component of scan. The CT scan has now essentially the middle third of the facial skeleton. The maxil- replaced plain films as the Ògold standardÓ la is a key bone in the midface that is closely asso- in both evaluation and treatment planning. ciated with adjacent bones providing structural If physical findings and plain films are not support between the cranial base and the occlusal suggestive of a zygomatic fracture, the eval- plane. Fractures of the maxilla occur less fre- uation may end here. However, if they do quently than those of the mandible or nose due to suggest fracture, a coronal and axial CT the strong structural support of this bone. The scan should be obtained. The CT scan will midface consists of alternating thick and thin sec- accurately reveal the extent of orbital tions of bone that are capable of resisting signifi- involvement, as well as degree of displace- cant force. This structurally strong bone provides ment of the fractures. This study is vital for protection for the globes and brain, projection of planning the operative approach. the midface, and support for occlusion. Reestablishing continuity of these buttresses is the Historically, closed reduction was the foundation on which maxillary fracture treatment method of choice for nearly all zygomatic is based. fractures. Multiple methods were employed, but most involved simply exert- Renee LeFort (1901) provided the earliest clas- ing pressure underneath the malar emi- sification system of maxillary fractures. -

Results Description of the SKULLS. the Overall Size of Both Skulls Was Considered to Be Within Normal Limits for Their Ethnic
Ossification Defects and Craniofacial Morphology In Incomplete Forms of Mandibulofacial Dysostosis A Description of Two Dry Skulls ERIK DAHL, D.D.S., DR. ODONT. ARNE BJORK, D.D.S., ODONT. DR. Copenhagen, Denmark The morphology of two East Indian dry skulls exhibiting anomalies which were suggested to represent incomplete forms of mandibulofacial dysostosis is described. Obvious although minor ossification anomalies were found localized to the temporal, sphenoid, the zygomatic, the maxillary and the mandibular bones. The observations substantiate the concept of the regional and bilateral nature of this malformation syndrome. Bilateral orbital deviations, hypoplasia of the malar bones, and incomplete zygomatic arches appear to be hard tissue aberrations which may be helpful in exami- nation for subclinical carrier status. Changes in mandibular morphology seem to be less distinguishing features in incomplete or abortive types of mandibulofacial dysostosis. KEY WORDS craniofacial problems, mandible, mandibulofacial dysostosis, maxilla, sphenoid bone, temporal bone, zygomatic bone Mandibulofacial dysostosis (MFD) often roentgencephalometric examinations were results in the development of a characteristic made of the skulls, and tomograms were ob- facial disfigurement with considerable simi- tained of the internal and middle ear. Com- larity between affected individuals. However, parisons were made with normal adult skulls the symptoms may vary highly in respect to and with an adult skull exhibiting the char- type and degree, and both incomplete and acteristics of MFD. All of the skulls were from abortive forms of the syndrome have been the same ethnic group. ' reported in the literature (Franceschetti and Klein, 1949; Moss et al., 1964; Rogers, 1964). Results In previous papers, we have shown the DEsCRIPTION OF THE SKULLS. -

Lab Manual Axial Skeleton Atla
1 PRE-LAB EXERCISES When studying the skeletal system, the bones are often sorted into two broad categories: the axial skeleton and the appendicular skeleton. This lab focuses on the axial skeleton, which consists of the bones that form the axis of the body. The axial skeleton includes bones in the skull, vertebrae, and thoracic cage, as well as the auditory ossicles and hyoid bone. In addition to learning about all the bones of the axial skeleton, it is also important to identify some significant bone markings. Bone markings can have many shapes, including holes, round or sharp projections, and shallow or deep valleys, among others. These markings on the bones serve many purposes, including forming attachments to other bones or muscles and allowing passage of a blood vessel or nerve. It is helpful to understand the meanings of some of the more common bone marking terms. Before we get started, look up the definitions of these common bone marking terms: Canal: Condyle: Facet: Fissure: Foramen: (see Module 10.18 Foramina of Skull) Fossa: Margin: Process: Throughout this exercise, you will notice bold terms. This is meant to focus your attention on these important words. Make sure you pay attention to any bold words and know how to explain their definitions and/or where they are located. Use the following modules to guide your exploration of the axial skeleton. As you explore these bones in Visible Body’s app, also locate the bones and bone markings on any available charts, models, or specimens. You may also find it helpful to palpate bones on yourself or make drawings of the bones with the bone markings labeled. -
The Axial Skeleton Visual Worksheet
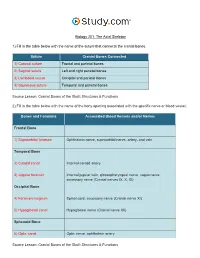
Biology 201: The Axial Skeleton 1) Fill in the table below with the name of the suture that connects the cranial bones. Suture Cranial Bones Connected 1) Coronal suture Frontal and parietal bones 2) Sagittal suture Left and right parietal bones 3) Lambdoid suture Occipital and parietal bones 4) Squamous suture Temporal and parietal bones Source Lesson: Cranial Bones of the Skull: Structures & Functions 2) Fill in the table below with the name of the bony opening associated with the specific nerve or blood vessel. Bones and Foramina Associated Blood Vessels and/or Nerves Frontal Bone 1) Supraorbital foramen Ophthalmic nerve, supraorbital nerve, artery, and vein Temporal Bone 2) Carotid canal Internal carotid artery 3) Jugular foramen Internal jugular vein, glossopharyngeal nerve, vagus nerve, accessory nerve (Cranial nerves IX, X, XI) Occipital Bone 4) Foramen magnum Spinal cord, accessory nerve (Cranial nerve XI) 5) Hypoglossal canal Hypoglossal nerve (Cranial nerve XII) Sphenoid Bone 6) Optic canal Optic nerve, ophthalmic artery Source Lesson: Cranial Bones of the Skull: Structures & Functions 3) Label the anterior view of the skull below with its correct feature. Frontal bone Palatine bone Ethmoid bone Nasal septum: Perpendicular plate of ethmoid bone Sphenoid bone Inferior orbital fissure Inferior nasal concha Maxilla Orbit Vomer bone Supraorbital margin Alveolar process of maxilla Middle nasal concha Inferior nasal concha Coronal suture Mandible Glabella Mental foramen Nasal bone Parietal bone Supraorbital foramen Orbital canal Temporal bone Lacrimal bone Orbit Alveolar process of mandible Superior orbital fissure Zygomatic bone Infraorbital foramen Source Lesson: Facial Bones of the Skull: Structures & Functions 4) Label the right lateral view of the skull below with its correct feature. -

Three-Dimensional Radiographic Evaluation of the Malar Bone Engagement Available for Ideal Zygomatic Implant Placement
Article Three-Dimensional Radiographic Evaluation of the Malar Bone Engagement Available for Ideal Zygomatic Implant Placement Gerardo Pellegrino 1,* , Francesco Grande 2 , Agnese Ferri 1, Paolo Pisi 3, Maria Giovanna Gandolfi 4 and Claudio Marchetti 1 1 Oral and Maxillofacial Surgery Unit, Department of Biomedical and Neuromotor Sciences, University of Bologna, 40125 Bologna, Italy; [email protected] (A.F.); [email protected] (C.M.) 2 Oral Surgery Unit, Dental School, Department of Biomedical and Neuromotor Sciences, University of Bologna, 40125 Bologna, Italy; [email protected] 3 Dental Radiology Unit, Dental School, Department of Biomedical and Neuromotor Sciences, University of Bologna, 40125 Bologna, Italy; [email protected] 4 Medical-technical Science, Dental School, Department of Biomedical and Neuromotor Sciences, University of Bologna, 40125 Bologna, Italy; mgiovanna.gandolfi@unibo.it * Correspondence: [email protected]; Tel.: +39-051-208-8157 Received: 11 June 2020; Accepted: 21 July 2020; Published: 22 July 2020 Abstract: Zygomatic implant rehabilitation is a challenging procedure that requires an accurate prosthetic and implant plan. The aim of this study was to evaluate the malar bone available for three-dimensional zygomatic implant placement on the possible trajectories exhibiting optimal occlusal emergence. After a preliminary analysis on 30 computed tomography (CT) scans of dentate patients to identify the ideal implant emergencies, we used 80 CT scans of edentulous patients to create two sagittal planes representing the possible trajectories of the anterior and posterior zygomatic implants. These planes were rotated clockwise on the ideal emergence points and three different hypothetical implant trajectories per zygoma were drawn for each slice. -

Orbital Meningiomas Meningiomas Orbitários Carlos Eduardo Da Silva, M.D
31 Revisão Orbital Meningiomas Meningiomas Orbitários Carlos Eduardo da Silva, M.D. 1 Paulo Eduardo Freitas, M.D. Ph.D.2 Alicia Del Carmem Becerra Romero, M.D.3 Tâmen Moyses Pereyra4 Vicente Faraon Fonseca4 Willian Alves Martins4 Márcio Aloisio Bezerra Cavalcanti Rockenbach4 Fáberson João Mocelin Oliveira4 ABSTRACT RESUMO Orbital meningiomas usually invade the orbit as an extension Meningeomas orbitários invadem a órbita, na maioria dos ca- of the sphenoid wing meningiomas, clinoidal meningiomas, sos, como uma extensão de meningeomas da asa do esfenóide, cavernous sinus meningiomas and tuberculum sella tumors. meningeomas do seio cavernoso, meningeomas da clinóide e They also arise into the orbit originating from the optic sheath do tubérculo da sela. Eles também podem ser originados do or as ectopical lesions. The authors present a review of clini- revestimento dural do nervo óptico ou como lesões ectópicas cal aspects and surgical treatment of the orbital meningio- intraorbitais. Os autores apresentam uma revisão dos aspectos mas. Material and methods: The authors present a literature clínicos e cirúrgicos dos meningeomas orbitários. Material e review of the anatomical, clinical, and surgical aspects of métodos: Os autores apresentam uma revisão da literatura dos the orbital meningiomas, add illustrative cases, pointing aspectos anatômicos, clínicos e cirúrgicos dos meningeomas their principal concerns about the treatment of such tumors. orbitários, com casos ilustrativos, apresentando suas principais Results: Exophthalmos and unilateral visual loss are the most preocupações no manejo destes tumores. Resultados: Exoftal- common features of the orbital meningiomas. There are two mia e perda visual unilateral são os achados mais frequentes important surgical routes to approach such tumors, which are nos meningeomas orbitários. -

Evaluation of Maxillary Bone Dimensions in Specific Areas for Removable Dentures
https://doi.org/10.5272/jimab.2017232.1527 Journal of IMAB Journal of IMAB - Annual Proceeding (Scientific Papers). 2017 Apr-Jun;23(2): ISSN: 1312-773X https://www.journal-imab-bg.org Original article EVALUATION OF MAXILLARY BONE DIMENSIONS IN SPECIFIC AREAS FOR REMOVABLE DENTURES Original Articles Dobromira Shopova1, Tanya Bozhkova1, Dian Slavchev1, Spas Muletarov2, Zdravka Ivanova3, Elena Bozhikova2 1) Department of Prosthetic Dentistry, Faculty of Dental Medicine, Medical University - Plovdiv, Bulgaria; 2) Department of Anatomy, Histology and Embryology, Medical University - Plovdiv, Bulgaria; 3) Department of Plant Physiology and Molecular Biology, Plovdiv University - Plovdiv, Bulgaria. ABSTRACT similar studies for quantitative evaluation module of elas- Background: Removable prosthetics is a big part of ticity and hardness in different anatomical regions, and Prosthetic Dentistry. Prosthetic field is very important for they were established middle level in frontal area and low successful treatment with partial or complete dentures. in distal zone [3, 4, 5]. The cortical density can be meas- Maxillary bone is covered with soft tissues, but its anatomy ured by Hounsfield units (HU). The investigations proved is essential for retention, chewing stability and comfort of various levels in cortical and cancellous bone densities. the patients. Maxillary tuberosity showed the lowest level [6]. Com- Purpose: The study’s aim was to evaluate the dimen- puted tomography’s study of the edentulous posterior max- sions of maxillary bone in specific zones for removable illae showed porous cortical crest or no cortical bone, al- dentures. though the bone densities varied markedly among indi- Methods: Sixteen craniums were measured in 10 dif- viduals [7]. Micro-computed tomography (microCT) is a ferent zones. -

The Vomer Bone Analysis in Relation to Class Iii Malocclusion Using Three Dimenssional Images Analysis
International Journal of Dental and Health Sciences Original Article Volume 04,Issue 05 THE VOMER BONE ANALYSIS IN RELATION TO CLASS III MALOCCLUSION USING THREE DIMENSSIONAL IMAGES ANALYSIS Ammar Mohi 1, Kadir Beycan2, Şebnem Erçalik Yalçinkaya3 1Postgraduate PhD researcher, Department of Oral and Maxillofacial Radiology, Faculty of Dentistry, Marmara University, Istanbul, Turkey. 2Assistant professor , Department of Orthodontics, Faculty of Dentistry, Marmara University, Istanbul, Turkey. 3Professor, Chairman and Head of Department of Oral and Maxillofacial Radiology, Faculty of Dentistry, Marmara University, Istanbul, Turkey. ABSTRACT: Objective: To evaluate the vomer bone dimenssional outline changes in relation to the midface hypoplasia of a Class III malocclusion by comparing with normal controls using a three dimenssional CBCT images analysis of Mimics 19.0 software. Material and Method: In total of 96 patients images were both Class III malocclusion as study cases and normal occlusion as controls with age between 15 to 30 years old. All patients were classified into three group based on ANB angular value of Steiner’s analysis. The study group were : normal, mild and sever malocclusion type groups. Linear and angular planes were determined by using 13 skeletal points and analysed by using Mimics 19.0 software. All study groups parameters statistically analysed for significant differences and correlation. Results: A high significant differences between the vomer bone anterior variables (P<0.01) followed by vomer posterior variables (P<0.05) in relation to cranial and midfacial measurements with positive correlation. The pattern of vomer bone was shown highly anterior impaction and backward inclination in sever type malocclusion group and male higher than female. -

Reconstruction of the Pediatric Maxilla and Mandible
ORIGINAL ARTICLE Reconstruction of the Pediatric Maxilla and Mandible Eric M. Genden, MD; Daniel Buchbinder, DMD, MD; John M. Chaplin, MBChB; Edgar Lueg, MD; Gerry F. Funk, MD; Mark L. Urken, MD Background: The creation of osseous defects in the up- Results: Two patients were lost to follow-up, and 1 per and lower jaws in children is an uncommon occur- died secondary to complications related to distant meta- rence. It is therefore likely that a head and neck recon- static disease. Three of 6 patients were observed for 2 structive surgeon will accumulate only limited experience years 6 months, 4 years, and 4 years 2 months, respec- in restoring such defects. We have reviewed 7 pediatric tively. Two of the 3 patients who were observed long bone-containing microvascular free flap reconstruc- term have undergone full dental rehabilitation and cur- tions in 6 patients for reconstruction of the upper or lower rently maintain a regular diet and deny pain with masti- jaws. Three patients were available for long-term fol- cation or deglutition. One patient did not require dental low-up to evaluate the effect of osseous free flap recon- rehabilitation. All 3 patients demonstrate gross facial struction on function and growth and development of symmetry and normal dental occlusion. Assessment of the donor site. the fibular donor site demonstrated normal limb length and circumference. The patients denied pain or restric- Design: Retrospective review. tion to recreational activity. Scapular donor sites demon- strated normal range of motion, strength, and shoulder Setting: Academic tertiary referral center for otolaryn- stability. gology. -

Topographical Anatomy and Measurements of Selected Parameters of the Rat Temporal Bone
Folia Morphol. Vol. 67, No. 2, pp. 111–119 Copyright © 2008 Via Medica O R I G I N A L A R T I C L E ISSN 0015–5659 www.fm.viamedica.pl Topographical anatomy and measurements of selected parameters of the rat temporal bone J. Wysocki Clinic of Otolaryngology, Medical Faculty No. 2, Medical University of Warsaw, Kajetany, Poland Institute of Physiology and Pathology of Hearing, Warsaw, Poland [Received 22 October 2008; Accepted 22 November 2008] On the basis of dissection of 24 bones of 12 black rats a systematic anatomical description was made and measurements of selected size parameters of the tem- poral bone were taken. Besides the main air space in the middle ear, the tym- panic bulla, there are also additional air cells, namely the anterior and posterior epitympanic recesses, containing the head of the malleus and the body of the incus. On the side of the epitympanic recesses the following are easily accessi- ble: the malleus head and the core of the incus, the superior and lateral semicir- cular canals and the facial nerve. On the side of the ventral tympanic bulla it is easy access to both windows and the cochlea. The semicircular canals are rela- tively large, the lateral canal being the largest and the posterior the smallest. The length of the spiral canal of the cochlea does not exceed 11 mm. It is worth mentioning that both the vertical and horizontal dimensions of the scala vestibuli and scala tympani do not even exceed 0.7 mm in the basal turn, and are signif- icantly decreased to tenths of a millimetre in further turns.