Determination
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
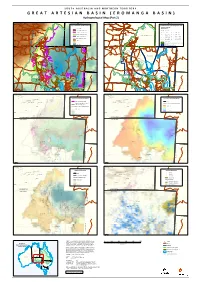
GREAT ARTESIAN BASIN Responsibility to Any Person Using the Information Or Advice Contained Herein
S O U T H A U S T R A L I A A N D N O R T H E R N T E R R I T O R Y G R E A T A R T E S I A N B A S I N ( E RNturiyNaturiyaO M A N G A B A S I N ) Pmara JutPumntaara Jutunta YuenduYmuuendumuYuelamu " " Y"uelamu Hydrogeological Map (Part " 2) Nyirri"pi " " Papunya Papunya ! Mount Liebig " Mount Liebig " " " Haasts Bluff Haasts Bluff ! " Ground Elevation & Aquifer Conditions " Groundwater Salinity & Management Zones ! ! !! GAB Wells and Springs Amoonguna ! Amoonguna " GAB Spring " ! ! ! Salinity (μ S/cm) Hermannsburg Hermannsburg ! " " ! Areyonga GAB Spring Exclusion Zone Areyonga ! Well D Spring " Wallace Rockhole Santa Teresa " Wallace Rockhole Santa Teresa " " " " Extent of Saturated Aquifer ! D 1 - 500 ! D 5001 - 7000 Extent of Confined Aquifer ! D 501 - 1000 ! D 7001 - 10000 Titjikala Titjikala " " NT GAB Management Zone ! D ! Extent of Artesian Water 1001 - 1500 D 10001 - 25000 ! D ! Land Surface Elevation (m AHD) 1501 - 2000 D 25001 - 50000 Imanpa Imanpa ! " " ! ! D 2001 - 3000 ! ! 50001 - 100000 High : 1515 ! Mutitjulu Mutitjulu ! ! D " " ! 3001 - 5000 ! ! ! Finke Finke ! ! ! " !"!!! ! Northern Territory GAB Water Control District ! ! ! Low : -15 ! ! ! ! ! ! ! FNWAP Management Zone NORTHERN TERRITORY Birdsville NORTHERN TERRITORY ! ! ! Birdsville " ! ! ! " ! ! SOUTH AUSTRALIA SOUTH AUSTRALIA ! ! ! ! ! ! !!!!!!! !!!! D !! D !!! DD ! DD ! !D ! ! DD !! D !! !D !! D !! D ! D ! D ! D ! D ! !! D ! D ! D ! D ! DDDD ! Western D !! ! ! ! ! Recharge Zone ! ! ! ! ! ! D D ! ! ! ! ! ! N N ! ! A A ! L L ! ! ! ! S S ! ! N N ! ! Western Zone E -
Wallace Rockhole Is Open for Business…
MacDonnell Regional Council Staff Newsletter SEPTEMBER 2015 volume 7 issue 3 Developing supportive communities communitiesLiveable communitiesEngaged A organisation COUNCIL GOAL COUNCIL GOAL COUNCIL GOAL COUNCIL GOAL #1 #2 #3 #4 Despite being a small community Wallace Rockhole has always shown great initiative to get things done Wallace Rockhole is open for business… Following the completion of MacDonnell Regional Council’s upgrade of the access road linking Wallace Rockhole to Larapinta Drive, tourists can now drive regular cars to experience the rock art and dot painting tours the community offers. Along with the road upgrade, a recent announcement by the Federal Government to install a mobile phone tower at this and three other communities, in the coming years will add to their accessibility. All this follows Wallace Rockhole being named the first ever community to be awarded a Tidy Town 4 Gold Star Tourism Award, after many years of community support for its cultural tourism infrastructure and services… Find out the latest instalments at Wallace Rockhole and other communities of the MacDonnell Regional Council inside MacDonnell Regional Council Staff Newsletter SEPTEMBER 2015 volume 7 issue 3 page 2 Welcome to MacDonnell Regional Council, CEO UPDATE We have all been very busy since the last MacNews finalising Our Regional Plan, meeting our Key Performance Indicators (KPIs) and finishing off another financial year full of improvements to the lives of our residents. At our most recent Council meeting, the KPI Report for the past financial year was presented, showing an outstanding effort across all areas of the MacDonnell Regional Council through some very impressive results. -
Alice Springs Community Services Directory 2021
2021 Alice Springs Community Services Directory Communities for Children – Anglicare NT Since 2010, Anglicare NT in Alice Springs has been funded by the Australian Government Department of Social Services as the Facilitating Partner for Communities for Children. The Facilitating Partner subcontracts Community Partners to deliver place-based, evidence- based early intervention activities in order to provide positive and sustainable outcomes for the most vulnerable and at-risk children, up to 12 years of age, and their families in Alice Springs. Our current Community Partners are Akeyulerre, FAST NT, Lutheran Community Care, Multicultural Community Services Central Australia, Red Cross and Relationships Australia. These organisations deliver a number of activities that promote Communities for Children’s objectives and vision. In addition to this, Communities for Children is working collaboratively in a Collective Impact Initiative with Connected Beginnings, Larapinta Child and Family Centre and Red Cross to promote Child Friendly Alice with the aim of encouraging greater integrated service delivery in Alice Springs. In 2021 Communities for Children will continue its strong focus on creating interconnected systems and networks, of supporting new ways of working together with local community that will help children thrive and make the most of their potential. Funded by the Australian Government Department of Social Services 0 Table of Contents Other Directories ____________________________________________________________ 2 Government Services -

Map of NT Electoral Boundaries (2008)
LINGIARI & SOLOMON LINGIARI & SOLOMON Latitude 10° S Latitude 10° S 2008 COMMONWEALTH OF AUSTRALIA Kilometres 0 50 100 200 Kilometres Christmas Island and the Cocos (Keeling) Islands are part of the Division of Lingiari ARAFURA SEA CHRISTMAS ISLAND COCOS (KEELING) Croker Island Cape North Keeling Wessel 105°40' Island ISLANDS Minjilang 024 kilometres Cape Don Cape Cockburn Commonwealth Electoral Act 1918 11°50' 11°50' 024 GURIG NATIONAL 105°35' Pularumpi PARK Wessel North East kilometres Milikapiti Islands Point 96°50' Rocky Point Goulburn Map of the Commonwealth Electoral Divisions of 10°25' 10°25' Settlement BATHURST ISLAND Islands 96°50' 96°55' MELVILLE ISLAND Warruwi Smith Point Horsburgh Island North West Point Brathwaite Point 12°05' 12°05' Moantu Nguilu Direction Van Diemen Gulf Cape Island Kilimiraka Stewart Jackson Point McPherson Point Waterfall LINGIARI & Martin Point Maningrida Galiwinku Cape Hotham Beagle Gulf Milingimbi Home Gunn Point Namaidpa District Island Point Stuart Maragulidban District GunyanGunyangara Nhulunbuy SOLOMONMurrumujuk Wright Point Gunbatgari District White Star Landing Yirrkala Jacks Point Oenpelli Ramingining Yarawoi District iver Deans Point Swim Creek Blyth 10°30' 10°30' DARWIN Woolner R Cape Arnhem Howard Adelaide East Rogers Bay River Springs SOLOMON Egeria Melaleuca River Bamboo Point Ja Ja Gapuwiyak Point Middle Point South Keeling (see enlargement) SOURCES Jones Point John D Point Belyuenuen Humpty Doo Alligator Point Stuart River Bees Creek Middle Point Mary This map has been compiled by Sinclair -

Independent Review of Policing in Remote Indigenous Communities in the Northern Territory Policing Further Into Remote Communities
Independent Review of Policing in Remote Indigenous Communities in the Northern Territory Policing further into remote communities April 2010 Report to the Australian Government and the Northern Territory Government Allen Consulting Group Pty Ltd ACN 007 061 930, ABN 52 007 061 930 Melbourne Level 9, 60 Collins St Melbourne VIC 3000 Telephone: (61-3) 8650 6000 Facsimile: (61-3) 9654 6363 Sydney Level 1, 50 Pitt St Sydney NSW 2000 Telephone: (61-2) 8272 5100 Facsimile: (61-2) 9247 2455 Canberra Empire Chambers, Level 2, 1-13 University Ave Canberra ACT 2600 GPO Box 418, Canberra ACT 2601 Telephone: (61-2) 6204 6500 Facsimile: (61-2) 6230 0149 Online Email: [email protected] Website: www.allenconsult.com.au Suggested citation for this report: Allen Consulting Group 2010, Independent Review of Policing in Remote Indigenous Communities in the Northern Territory. Disclaimer: While the Allen Consulting Group endeavours to provide reliable analysis and believes the material it presents is accurate, it will not be liable for any claim by any party acting on such information. © Allen Consulting Group 2010 The Allen Consulting Group ii I NDEPENDENT R EVIEW OF P OLICING IN R EMOTE I NDIGENOUS C OMMUNITIES Contents Executive summary v Summary of recommendations ix Introduction 11 Project objectives and scope of services 11 Conceptual framework — remote community safety 13 Review method 15 Chapter 1 The Northern Territory context 17 Chapter 2 Current policing in remote NT communities 23 2.1 Remote communities in the Northern Territory 24 2.2 -

Annual Report 2018–19
CENTRAL LAND COUNCIL ANNUAL REPORT 2018–19 CENTRAL LAND COUNCIL Creative Commons licence With the exception of the Commonwealth Coat of Arms and where otherwise noted, all material presented in this report is provided under a Creative Commons licence. The details of the relevant licence conditions are available on the Creative Commons website at: http://creativecommons.org/licences/byl3.0/legalcode. The document must be attributed as the Central Land Council annual report 2018–19. Third party copyright for publications This organisation has made all reasonable effort to: • clearly label material where the copyright is owned by a third party • ensure that the copyright owner has consented to this material being presented in this publication. ISSN 1034-3652 All photos Central Land Council, unless otherwise credited. 19 September 2019 Minister for Indigenous Australians Hon Ken Wyatt AM, MP 19 September 2019 PO Box 6022 HouseMinister of forRepresentatives Indigenous Australians ParliamentHon Ken Wyatt House AM, MP CanberraPO Box 6022 ACT 2600 House of Representatives Parliament House Canberra ACT 2600 Dear Minister In accordanceaccordance with with the the Aboriginal Aboriginal Land Land Rights Rights (Northern (Northern Territory) Territory) Act Act1976 1976, the (Cth),Native the Title Native TitleActDear 1993 ActMinister 1993and the and Public the Public Governance Governance and Accountability and Accountability Act 2013 Act, I 2013am pleased (Cth) (the to approve PGPA Act), Iand am submit pleased the to 2018 approve-19 Annual and submit -

Annual Report 2019/20
............ 2019-2020 Central Australian Aboriginal Congress ANNUAL REPORT ICN 7823 ............................................................... ........................................................................................................................ 2019-2020 Central Australian Aboriginal Congress ANNUAL REPORT ........................................................................................................................ Please be advised that this publication may contain images of deceased persons ........................................................................................................................... ACKNOWLEDGEMENTS Central Australian Aboriginal Congress (Congress) • Alcohol and Other Drugs Services of Central • Central Australian Aboriginal Family Violence works in partnership with the community to Australia Legal Unit (CAAFLU) deliver coordinated and effective primary health • Alice Springs Town Council • Central Australian Women’s Legal Service (CAWLS) care to Aboriginal people living in Central • Australian Drug Foundation Australia. • Central Australian Academic Health Science • Australian Institute of Aboriginal and Torres Network Strait Islander Studies (AIATSIS) Congress members, patients and clients continue to play • Central Australian Football Club the most vital role in determining the direction of our • Australian Nurse Family Partnership Program services and programs—we thank you for your continued (ANFPP) • Central Australian Remote Health Development Services (CARHDS) support -

Opening of the Alice Springs Office of the Commonwealth Ombudsman
Opening of the Alice Springs office of the Commonwealth Ombudsman The opening of a new office in Alice Springs is an important and historic development for the Commonwealth Ombudsman. We are especially pleased to be joined on this occasion by members from Aboriginal communities in the Alice Springs region. I begin by acknowledging the Mbantua people, the traditional owners of the land on which we meet. We pay our respects to their elders and descendants, past and present. It is a great pleasure also to welcome many others who work in government agencies and community organisations. I note the presence of Government Business Managers and other officers from Australian Government and Northern Territory Government agencies, the community leaders from Aboriginal land councils and support groups, and staff from local media agencies. I extend a special welcome also to Major General Dave Chalmers, the head of the Northern Territory Emergency Response team, who has kindly joined us for this opening. Another highlight of this opening is the ‘welcome to country’ by Elaine Peckham, a member of the Mbantua community. Elaine’s welcome opens the door to all of us, from many different backgrounds and organisations, to work together as a community as we open a new office in a traditional setting. The office of the Commonwealth Ombudsman was established in 1977 - just over thirty years ago. A foundation principle that has guided the work of the office is that it must be a national operation. An office that helps people resolve problems they encounter in dealing with government should be in close contact with people and government around the country. -

Solar Setup Fact Sheet
Transforming the way we power the Territory The Solar Energy Transformation Program (SETuP) saw the rollout of 10MW of power to benefit 25 remote Northern Territory communities. The program was completed in 2019. 94 million litres Estimated savings of 94 million litres of diesel will be achieved over the life of the program 1MW solar with $59 million 2MWh battery Total program cost Flagship project at Daly funded by the Australian River allowing 100% of solar Renewable Energy Agency energy use during the day (ARENA) and the Northern Territory Government 50% 250,000 15% 25 years Diesel savings Average reduction Estimated life of tonnes the program for Daly River CO2 emissions saved over in diesel reliance the life of the program overall across 24 sites without battery The Solar Energy Transformation Program is delivering cleaner, greener energy to remote Aboriginal communities across the Northern Territory. Warruwi (175kW) Pirlangimpi Milikapiti Minjilang (100kW) Maningrida Milingimbi Galiwinku (1175kW) (400kW) (750kW) Gunbalanya Wurrumiyanga (675kW) (1075kW) Gunyangara Ramingining Yirrkala Darwin (500kW) Belyuen Jabiru Gapuwiyak Acacia Larrakia (425kW) NORTHERN Daly River Milyakburra (1000kW) REGION (100kW) Weemol Kybrook Farm Umbakumba Bulman Angurugu (100kW) Peppimenarti Jodetluk Wadeye Numbulwar Nganmarriyanga Manyalluk Katherine Barunga Rockhole Beswick Rittarangu Binjari Jilkminggan Ngukurr (400kW) Minyerri Timber Creek KATHERINE (275kW) Gudabijin REGION Borroloola Daly Waters Amanbidiji Yarralin Pigeon Hole Mungoobada Daguragu Kalkarindji -

Translations Indigenous Languages
TRANSLATIONS TRANSLATIONS INDIGENOUS LANGUAGES How do you talk to someone who Northern Territory Australian Capital Territory doesn’t understand your language? Aboriginal Interpreter Services NAATI What good are written translations to www.ais.nt.gov.au www.naati.com.au someone who can’t read? 08 8999 6060 02 6260 3035 High quality translated messages CAAMA Radio New South Wales are the key to engaging your target www.caama.com.au audience. NAATI 08 8951 9778 Professional translation services will work www.naati.com.au to improve linguistics including changing Radio Larrakia 02 9267 1357 jargon, and grammar to reflect the www.radiolarrakia.org Victoria features of your chosen language. They 08 8943 7900 simplify scripts to ensure your message NAATI translates well into any language and Queensland www.naati.com.au provide high quality files, produced at 2M Language Services 03 9642 3303 perfect pitch, volume, length and speed. www.2m.com.au Tasmaina 07 3367 8722 Please note OneTalk requires WAV files to NAATI produce Talking Products. NAATI www.naati.com.au www.naati.com.au Translation services available in Australia 03 6223 6534 07 3393 1358 are listed right.. Other languages and national Western Australia services Kimberley Interpreting Service All Graduates Interpreting and Translating www.kimberleyinterpreting.org.au www.allgraduates.com.au 08 9192 3981 1300 854 799 NAATI 2M Language Services www.naati.com.au www.2m.com.au 07 3393 1358 1800 462 742 South Australia NAATI NAATI www.naati.com.au www.naati.com.au 02 6260 3035 08 8410 5233 ONETALK PRODUCTS SPEAK FOR THEMSELVES TRANSLATIONS LANGUAGES AND COMMUNITIES ACROSS THE NORTHERN TERRITORY. -

Remote Housing Arrangements in the NT Aboriginal Housing Forum Darwin, Hilton 7 March 2018 Dr Josie Douglas – Manager, CLC Policy Central Land Council
Remote Housing Arrangements in the NT Aboriginal Housing Forum Darwin, Hilton 7 March 2018 Dr Josie Douglas – Manager, CLC Policy Central Land Council • Statutory authority under Land Rights Act NT (1976) and Native Title Act (1993) • Long history of working effectively in region – land claims, land use agreements, land management, advocacy, community and economic development • Strong representative organisation - governed by a Council of 90 traditional owners CLC Region – southern half of NT • 24,000 constituents • 15 languages, across 771,747 square kilometers • More than 400,000sq kms (50%) is Aboriginal freehold Tenure status of main communities ALRA – Aboriginal Ali Curung freehold Alpurrurulam CLA – NT freehold Amoonguna ALRA Ampilatwatja ALRA Apatula (Finke) NT freehold Areyonga ALRA Atitjere CLA Canteen Creek Under Claim Daguragu ALRA Engawala CLA Haasts Bluff ALRA Hermannsburg (Ntaria) ALRA Imangara CLA Imanpa CLA Kalkaringi NT freehold Kaltukatjara (Docker River) ALRA Kintore ALRA Lajamanu ALRA Laramba CLA Mt Liebig ALRA Nturiya ALRA Papunya ALRA Pmara Jutunta ALRA Santa Teresa ALRA Titjikala CLA Wallace Rockhole ALRA Wilora CLA Willowra ALRA Wutunugurra CLA Yuelamu ALRA Yuendumu ALRA Remote Housing and Tenure - Background • Until 2008 all community housing was managed by ICHOs, around 75% were run through the local councils, with no tenure • June 2007 Howard announced the – NTER – the ‘Intervention’ • NTER - compulsory acquisition of five year ‘leases’ over most remote communities (31 in the CLC area) • Australian Government became the landlord and in September 2007 they signed an MoU with the NT Government: ‘for all communities, access to…funds for repairs and upgrades will be dependent on those communities agreeing to the transfer of their housing to publicly owned Territory Housing..’ Background • The five year lease allowed the wholesale take-over by Territory Housing • ‘Secure tenure’ policy was driven by both levels of government – no investment in remote communities without a lease being secured. -
Northern Territory Government S28 2018
Northern Territory of Australia Government Gazette ISSN-0157-833X No. S34 28 May 2018 Northern Territory of Australia Medicines, Poisons and Therapeutic Goods Act Community Health Centres and Clinics Revocation, Declarations and Approvals I, Hugh Crosbie Heggie, Chief Health Officer: (a) under sections 252, 254(1) and 250(1) of the Medicines, Poisons and Therapeutic Goods Act and with reference to section 43 of the Interpretation Act, revoke the declarations and approvals made by instrument entitled "Community Health Centres and Clinics Revocation, Declarations and Approvals" dated 9 August 2017 and published in Gazette No.S57 of 10 August 2017; and (b) under section 252 of the Medicines, Poisons and Therapeutic Goods Act, declare each health centre or clinic specified in the Schedule, Part A, to be a place to which Part 2.6 of the Act applies; and (c) under section 254(1) of the Act, approve each Scheduled substance treatment protocol specified in the Schedule, Part B, for each health centre or clinic specified in the Schedule, Part A; and (d) under section 250(1)(a) of the Act, declare each nurse or midwife practising at a health centre or clinic specified in the Schedule, Part A, to be an approved nurse or approved midwife (as appropriate) to supply, administer to another person and possess the Schedule 4 and 8 Northern Territory Government Gazette No. S34, 28 May 2018 substances specified in the Schedule, Part C, in accordance with each Scheduled substance treatment protocol specified in the Schedule, Part B; and (e) under section 250(1)(b) of the Act, declare each Aboriginal and Torres Strait Islander health practitioner practising at a health centre or clinic specified in the Schedule, Part A, to be an approved ATSI health practitioner to supply, administer to another person and possess the Schedule 4 and 8 substances specified in the Schedule, Part C, in accordance with each Scheduled substance treatment protocol specified in the Schedule, Part B.