MR Findings in Kernicterus
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Neonatal Orthopaedics
NEONATAL ORTHOPAEDICS NEONATAL ORTHOPAEDICS Second Edition N De Mazumder MBBS MS Ex-Professor and Head Department of Orthopaedics Ramakrishna Mission Seva Pratishthan Vivekananda Institute of Medical Sciences Kolkata, West Bengal, India Visiting Surgeon Department of Orthopaedics Chittaranjan Sishu Sadan Kolkata, West Bengal, India Ex-President West Bengal Orthopaedic Association (A Chapter of Indian Orthopaedic Association) Kolkata, West Bengal, India Consultant Orthopaedic Surgeon Park Children’s Centre Kolkata, West Bengal, India Foreword AK Das ® JAYPEE BROTHERS MEDICAL PUBLISHERS (P) LTD. New Delhi • London • Philadelphia • Panama (021)66485438 66485457 www.ketabpezeshki.com ® Jaypee Brothers Medical Publishers (P) Ltd. Headquarters Jaypee Brothers Medical Publishers (P) Ltd. 4838/24, Ansari Road, Daryaganj New Delhi 110 002, India Phone: +91-11-43574357 Fax: +91-11-43574314 Email: [email protected] Overseas Offices J.P. Medical Ltd. Jaypee-Highlights Medical Publishers Inc. Jaypee Brothers Medical Publishers Ltd. 83, Victoria Street, London City of Knowledge, Bld. 237, Clayton The Bourse SW1H 0HW (UK) Panama City, Panama 111, South Independence Mall East Phone: +44-2031708910 Phone: +507-301-0496 Suite 835, Philadelphia, PA 19106, USA Fax: +02-03-0086180 Fax: +507-301-0499 Phone: +267-519-9789 Email: [email protected] Email: [email protected] Email: [email protected] Jaypee Brothers Medical Publishers (P) Ltd. Jaypee Brothers Medical Publishers (P) Ltd. 17/1-B, Babar Road, Block-B, Shaymali Shorakhute, Kathmandu Mohammadpur, Dhaka-1207 Nepal Bangladesh Phone: +00977-9841528578 Mobile: +08801912003485 Email: [email protected] Email: [email protected] Website: www.jaypeebrothers.com Website: www.jaypeedigital.com © 2013, Jaypee Brothers Medical Publishers All rights reserved. No part of this book may be reproduced in any form or by any means without the prior permission of the publisher. -

Necrotizing Enterocolitis in a Newborn Following Intravenous Immunoglobulin Treatment for Haemolytic Disease
CASE REPORT Necrotizing Enterocolitis in a Newborn Following Intravenous Immunoglobulin Treatment for Haemolytic Disease Semra Kara1, Hulya Ulu-ozkan2, Yavuz Yilmaz2, Fatma Inci Arikan3, Ugur Dilmen4 and Yildiz Dallar Bilge3 ABSTRACT ABO iso-immunization is the most frequent haemolytic disease of the newborn. Treatment depends on the total serum bilirubin level, which may increase very rapidly in the first 48 hours of life in cases of haemolytic disease of the newborn. Phototherapy and, in severe cases, exchange transfusion are used to prevent hyperbilirubinaemic encephalopathy. Intravenous immunoglobulins (IVIG) are used to reduce exchange transfusion. Herein, we present a female newborn who was admitted to the NICU because of ABO immune haemolytic disease. After two courses of 1 g/kg of IVIG infusion, she developed necrotizing enterocolitis (NEC). Administration of IVIG to newborns with significant hyperbilirubinaemia due to ABO haemolytic disease should be cautiously administered and followed for complications. Key Words: Necrotizing enterocolitis. Hyperbilirubinaemia. Newborn. Intravenous immunoglobulins. Iso-immunization. INTRODUCTION important adverse reactions,6 one of which is described Blood group incompatibilities are most frequent and hereby. severe conditions causing hyperbilirubinaemia in the neonatal period.1 Phototherapy and in severe cases CASE REPORT exchange transfusion are used to prevent kernicterus A female newborn was admitted to our neonatal unit and reduce perinatal mortality. Exchange transfusion because of jaundice on the tenth hours after being born. is not free of severe complications such as thrombo- The baby was born by uncomplicated vaginal delivery to cytopenia, apnoea, pulmonary haemorrhage, haemodyna- a healthy 31-year-old mother who was fourth gravida mic instability, septicaemia and necrotizing enterocolitis and second para. -

Hypotonia and Lethargy in a Two-Day-Old Male Infant Adrienne H
Hypotonia and Lethargy in a Two-Day-Old Male Infant Adrienne H. Long, MD, PhD,a,b Jennifer G. Fiore, MD,a,b Riaz Gillani, MD,a,b Laurie M. Douglass, MD,c Alan M. Fujii, MD,d Jodi D. Hoffman, MDe A 2-day old term male infant was found to be hypotonic and minimally abstract reactive during routine nursing care in the newborn nursery. At 40 hours of life, he was hypoglycemic and had intermittent desaturations to 70%. His mother had an unremarkable pregnancy and spontaneous vaginal delivery. The mother’s prenatal serology results were negative for infectious risk factors. Apgar scores were 9 at 1 and 5 minutes of life. On day 1 of life, he fed, stooled, and voided well. Our expert panel discusses the differential diagnosis of hypotonia in a neonate, offers diagnostic and management recommendations, and discusses the final diagnosis. DRS LONG, FIORE, AND GILLANI, birth weight was 3.4 kg (56th PEDIATRIC RESIDENTS percentile), length was 52 cm (87th aDepartment of Medicine, Boston Children’s Hospital, d e percentile), and head circumference Boston, Massachusetts; and Neonatology Section, Medical A 2-day old male infant born at Genetics Section, cDivision of Child Neurology, and 38 weeks and 4 days was found to be was 33 cm (12th percentile). His bDepartment of Pediatrics, Boston Medical Center, Boston, limp and minimally reactive during physical examination at birth was Massachusetts routine care in the newborn nursery. normal for gestational age, with Drs Long, Fiore, and Gillani conceptualized, drafted, Just 5 hours before, he had an appropriate neurologic, cardiac, and and edited the manuscript; Drs Douglass, Fujii, and appropriate neurologic status when respiratory components. -

Hypotonia Surestep Product Catalog Page 29 in Step with Pediatric Hypotonia
SPECIAL EDUCATIONAL SERIES DIAGNOSTIC INSIGHTS ANALYZING GAIT CHANGES GROSS MOTOR SKILLS ORTHOTIC MANAGEMENT CLI N I CAL CASE STUDIES Sponsored by an educational grant from: In Step With Pediatric Hypotonia SureStep Product Catalog Page 29 In Step With Pediatric Hypotonia Contents VIEWPOINT FROM THE EDITOR: An Unexpected Path, Mobility and More an Invaluable Perspective At the most basic level, mobility is about get- PAGE 3 ting from point A to point B. But, for many children with hypotonia, it’s about so much 4 more. FEATURES It’s about independence. It’s about con- fidence. It’s about maintaining strength, fit- ness, and healthy bones. It’s about not being Understanding Hypotonia excluded from activities enjoyed by their PAGE 4 typically developing peers. And improved mobility may have even Gait: The Cornerstone more benefits in those children whose hy- potonia is associated with social and behav- of Intervention ioral developmental delays. New research PAGE 8 has identified an association between motor skills and sociobehavioral milestones in chil- 8 The Importance of Gross dren with autism spectrum disorder, who often present with hypotonia (see “The Im- Motor Skills portance of Gross Motor Skills,” page 12). PAGE 12 This suggests that early intervention to improve gross motor skills—including or- thotic devices and physical therapy—may Orthotic Solutions for also help certain children interact more Children with Hypotonia comfortably with others. That won’t come as PAGE 16 a surprise to the clinicians and parents who 12 have personally seen it happen. This special issue is filled with evidence- Orthotic Success Stories: based information and personal success sto- Four Cases in a Series ries illustrating how effective interventions can enhance mobility in children with hy- PAGE 20 potonia. -

Delayed Cord Clamping in Red Blood Cell Alloimmunization: Safe, Effective, and Free?
Editorial Delayed cord clamping in red blood cell alloimmunization: safe, effective, and free? Ryan M. McAdams Department of Pediatrics, University of Washington, Seattle, WA, USA Correspondence to: Ryan M. McAdams, MD, Associate Professor. Division of Neonatology, Department of Pediatrics, University of Washington, Box 356320, Seattle, WA 98195-6320, USA. Email: [email protected]. Abstract: Hemolytic disease of the newborn (HDN), an alloimmune disorder due to maternal and fetal blood type incompatibility, is associated with fetal and neonatal complications related to red blood cell (RBC) hemolysis. After delivery, without placental clearance, neonatal hyperbilirubinemia may develop from ongoing maternal antibody-mediated RBC hemolysis. In cases refractory to intensive phototherapy treatment, exchange transfusions (ET) may be performed to prevent central nervous system damage by reducing circulating bilirubin levels and to replace antibody-coated red blood cells with antigen-negative RBCs. The risks and costs of treating HDN are significant, but appear to be decreased by delayed umbilical cord clamping at birth, a strategy that promotes placental transfusion to the newborn. Compared to immediate cord clamping (ICC), safe and beneficial short-term outcomes have been demonstrated in preterm and term neonates receiving delayed cord clamping (DCC), a practice that may potentially be effective in cases RBC alloimmunization. Keywords: Red blood cell (RBC); delayed cord clamping (DCC); exchange transfusions (ET) Submitted Mar 29, 2016. Accepted for publication Apr 11, 2016. doi: 10.21037/tp.2016.04.02 View this article at: http://dx.doi.org/10.21037/tp.2016.04.02 Hemolytic disease of the newborn (HDN) is an alloimmune exchange transfusions (ET) may be performed to prevent disorder caused by transplacentally transmitted maternal kernicterus by reducing circulating bilirubin levels and immunoglobulin (Ig) G antibodies that bind to paternally to replace antibody-coated RBCs with antigen-negative inherited antigens present on fetal red blood cells RBCs. -

JMSCR Vol||05||Issue||03||Page 19659-19665||March 2017
JMSCR Vol||05||Issue||03||Page 19659-19665||March 2017 www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 83.27 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v5i3.210 Maternal and Neonatal Determinants of Neonatal Jaundice – A Case Control Study Authors Sudha Menon1, Nadia Amanullah2 1Additional Professor, Department of Obstetrics and Gynecology, Government Medical College Trivandrum, Kerala, South India 2Msc Nursing Student, Government Nursing College, Trivandrum Corresponding Author Dr Sudha Menon Email: [email protected] ABSTRACT Neonatal jaundice a common condition which affects about 60-80% of newborn and if severe can lead serious neurological sequelae. Determinants include neonatal and maternal factors. A prospective case control descriptive study in a tertiary care centre was done in 62 consecutive cases with neonatal jaundice and 124 consecutive newborns without jaundice served as controls. The major determinants for neonatal jaundice were low birth weight <2.5 kg (OR 24.54 95% CI 10.98 – 54.84 : P<0.0001), birth asphyxia (OR 16.5; 95% CI 4.63- 58.76, P<0.0001), Low APGAR score <7( OR 26.1; 95% CI 3.28- 207.47, P =0.0002), prematurity <37weeks ( OR 28.92 95% CI 12.15-68.82 P=0.0001) Preterm premature rupture of membranes (OR 58.57 95% CI 7.67 -449.87 P<0.0001) and malpresentation (OR 14.64 95% CI 3.16 - 67.792 tailed p =0.00004).The factors which evolved significant on logistic regression were Preterm premature rupture of membranes , gestational age <37 weeks , APGAR score below 7, Birth weight below 2500grams, Birth asphyxia and multiple pregnancy. -

Newborn Metabolic Profile Associated with Hyperbilirubinemia with and Without Kernicterus
Citation: Clin Transl Sci (2019) 12, 28–38; doi:10.1111/cts.12590 ARTICLE Newborn Metabolic Profile Associated with Hyperbilirubinemia With and Without Kernicterus Molly E. McCarthy1,2,*, Scott P. Oltman3, Rebecca J. Baer4,5, Kelli K. Ryckman6, Elizabeth E. Rogers7, Martina A. Steurer-Muller8, John S. Witte9 and Laura L. Jelliffe-Pawlowski10 Our objective was to assess the relationship between hyperbilirubinemia with and without kernicterus and metabolic profile at newborn screening. Included were 1,693,658 infants divided into a training or testing subset in a ratio of 3:1. Forty- two metabolites were analyzed using logistic regression (odds ratios (ORs), area under the receiver operating characteristic curve (AUC), 95% confidence intervals (CIs)). Several metabolite patterns remained consistent across gestational age groups for hyperbilirubinemia without kernicterus. Thyroid stimulating hormone (TSH) and C- 18:2 were decreased, whereas tyrosine and C- 3 were increased in infants across groupings. Increased C- 3 was also observed for kernicterus (OR: 3.17; 95% CI: 1.18–8.53). Thirty- one metabolites were associated with hyperbilirubinemia without kernicterus in the training set. Phenylalanine (OR: 1.91; 95% CI: 1.85–1.97), ornithine (OR: 0.76; 95% 0.74–0.77), and isoleucine + leucine (OR: 0.63; 95% CI: 0.61–0.65) were the most strongly associated. This study showed that newborn metabolic function is associated with hyper- bilirubinemia with and without kernicterus. Study Highlights WHAT IS THE CURRENT KNOWLEDGE ON THE TOPIC? WHAT DOES THIS STUDY ADD TO OUR KNOWLEDGE? ✔ A variety of neonatal and maternal characteristics are ✔ Forty-one infant metabolites collected at newborn known to be associated with increased risk of hyperbili- screening were shown to be associated with neonatal hy- rubinemia. -
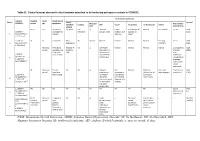
IUGR: Intrauterine Growth Restriction
Table S1. Clinical features observed in the 6 patients described so far harboring pathogenic variants in FOXRED1. Evolutionary symptoms Variants Prenatal Onset Onset clinical Patient Lactic/ Survival FOXRED1 period age symptoms Muscular Psychomotor Metabolic Epilepsy MRI Visual Respiratory Cardiovascular Others tone development acidosis IUGR 2m Hypotonia Yes (+++) Yes ↓ Normal Latent Bronchospasm Normal AEP normal IQ: 48 Alive c.920G>A Development refractary (2m,4y,7y3m) strabismus of episodes in (15y) 1 (p.Gly307Glu) / al delay right eye infant c.733+1G>A c.920G>A NI 4y Clumsiness With No Normal Normal Normal Normal Normal Learning IQ: 99 Alive 2 (p.Gly307Glu) / exercise (+) disorders (19y) c.733+1G>A - Neonatal Premature; No (only ↑ Yes ↓ Decreased Normal Normal Normal Normal Gradually loss Alive period Hypoglycemia lactate in attenuation in of motor (22y)) Congenital LCR) the putamen skills; c.694C>T lactic acidosis and cerebellar wheelchair; (p.Gln232X) / 3 atrophy (6y) no expressive c.1289A>G language; 18 (p.Asn430Ser) understands simple commands NI Neonatal Truncal Yes Yes ↓ Delayed Eye Normal Mild non- Persistent Psychomotor Alive period hypotonia myelination movements obstructive left hepatomegaly retardation (10y) c.1054 C>T Poor feeding ventricular have always ventricular (p.Arg352Trp) / dilatation; been roving hypertrophy 4 c.1054 C>T abnormal signal bilateral optic (p.Arg352Trp) 19 in the thalami atrophy and basal ganglia (8m) c.1308G>A ND ND ND ND Yes NA NA NA NA NA NA Severe Alive (p.Val421Met) / psychomotor (¿) 5 c.1308G>A retardation (p.Val421Met)20 IUGR; Neonatal Congenital Yes Yes ↓ Large -- Persistent Dilated right - - Death (3 c.612_615dupA Cerebral period lactic periventricular severe ventricle and months) CTG intraventric acidosis. -

Cerebral Hypotonia by Mihee Bay MD (Dr
Cerebral hypotonia By Mihee Bay MD (Dr. Bay of Kennedy Krieger Institute and Johns Hopkins School of Medicine has no relevant financial relationships to disclose.) Originally released July 12, 2006; last updated February 1, 2016; expires February 1, 2019 Introduction This article includes discussion of cerebral hypotonia, central hypotonia, essential hypotonia, benign congenital hypotonia, and floppy infant. The foregoing terms may include synonyms, similar disorders, variations in usage, and abbreviations. Overview Hypotonia is a clinical manifestation of numerous diseases affecting the central and/or peripheral motor nervous system. The key to accurate diagnosis involves integral steps of evaluation that include a detailed history, examination, and diagnostic tests. “Cerebral” (or central) hypotonia implies pathogenesis from abnormalities from the central nervous system, and related causal disorders include cerebral dysgenesis and genetic or metabolic disorders. Patients with central hypotonia generally have hypotonia without associated weakness, in contrast to the peripheral (lower motor neuron) causes, which typically produce both hypotonia and muscle weakness. Hypotonia is a clinical manifestation of over 500 genetic disorders; thus, a logical, stepwise approach to diagnosis is essential. With recent advances in the field of genetic testing, diagnostic yield will undoubtedly improve. There is no cure, but treatment includes supportive therapies, such as physical and occupational therapy, and diagnosis-specific management. Key points • Hypotonia is reduced tension or resistance of passive range of motion. • The first step in the evaluation of a child with hypotonia is localization to the central (“cerebral”) or peripheral nervous system, or both. • Central hypotonia is more likely to be noted axially with normal strength and hyperactive to normal deep tendon reflexes. -

Hyperbilirubinemia and Kernicterus Jesus Peinado PGY2 Merle Ipson MD March 2009 Hyperbilirubinemia
Hyperbilirubinemia and Kernicterus Jesus Peinado PGY2 Merle Ipson MD March 2009 Hyperbilirubinemia Most common clinical condition requiring evaluation and treatment in the NB Most common cause of readmission in the 1 st week Generally a benign transitional phenomenon May pose a direct threat of brain damage May evolve into kernicterus Kernicterus 1. Choreoathetoid cerebral palsy 2. High-frequency central neural hearing loss 3. Palsy of vertical gaze 4. Dental enamel hypoplasia (result of bilirubin-induced cell toxicity) Kernicterus Originally described in NB with Rh hemolytic disease Recently reported in healthy term and late preterm Reported in breast-fed infants w/out hemolysis Most prevalent risk factor is late preterm Late Preterm Infant Relatively immature in their capacity to handle unconjugated bilirubin Hyperbilirubinemia is more prevalent, pronounced and protracted Eightfold increased risk of developing TSB > 20 mg/dl (5.2%) compared to term (0.7%) Pathobiology Increased bilirubin load in the hepatocyte Decreased erythrocyte survival Increased erythrocyte volume Increased enterohepatic circulation Decreased hepatic uptake from plasma Defective bilirubin conjugation Bilirubin Metabolism Bilirubin Metabolism Bilirubin Metabolism How bilirubin Damages the Brain Determinants of neuronal injury by bilirubin 1. Concentration of unconjugated bilirubin 2. Free bilirubin 3. Concentration of serum albumin 4. Ability to bind UCB 5. Concentration of hydrogen ion 6. Neuronal susceptibility Intracellular Calcium Homeostasis -

Histological Findings in the Kernicterus-Associated Vulnerable
Palmela et al. Int J Pathol Clin Res 2015, 1:1 ISSN: 2469-5807 International Journal of Pathology and Clinical Research Research Article: Open Access Histological Findings in the Kernicterus-Associated Vulnerable Brain Regions are Linked to Neurodegeneration, Alterations in Astrocyte and Pericyte Distribution, and Vascular Modifications Inês Palmela1, Pedro Pereira2,3, Masaharu Hayashi4, Dora Brites1,5 and Maria A. Brito1,5* 1Research Institute for Medicines, Faculdade de Farmácia, Universidade de Lisboa, Portugal 2Laboratory of Neuropathology, Centro Hospitalar Lisboa Norte, Portugal 3Neuromuscular Unit, Institute of Molecular Medicine, Faculdade de Medicina, Universidade de Lisboa, Portugal 4Department of Brain Development and Neural Regeneration, Tokyo Metropolitan Institute of Medical Science, Japan 5Department of Biochemistry and Human Biology, Faculdade de Farmácia, Universidade de Lisboa, Portugal *Corresponding author: Maria A. Brito, Medicines Research Institute (iMed. ULisboa), Faculdade de Farmácia, Universidade de Lisboa, Avenida Professor Gama Pinto, 1649-003 Lisbon, Portugal, Tel: 351217946449, Fax: 351217946491, E-mail: [email protected] Abstract Keywords Kernicterus is a severe manifestation of neonatal unconjugated Astrogliosis, Basement membrane, Blood-brain barrier, Caveolae, hyperbilirubinemia. We investigated the neuro-glia-vascular Hyperpermeability, Kernicterus, Pericyte vascular coverage, alterations in autopsy material from three infants with kernicterus. Transcytosis, Unconjugated bilirubin, Vascularization Histological and immunohistochemical studies were performed in the cerebellum, hippocampus and basal ganglia, the most vulnerable brain regions to bilirubin-induced neurotoxicity. The data obtained Introduction were compared with the relatively spared temporal cortex, as well as with three aged-matched controls with no hyperbilirubinaemia. Neonatal jaundice is extremely common in the first week of Our data showed a reduction of the external germinal layer life, affecting 60 to 85% of neonates [1]. -

Mean Platelet Volume in Asymptomatic Chorioamnionitis-Exposed Infants
www.jpnim.com Open Access eISSN: 2281-0692 Journal of Pediatric and Neonatal Individualized Medicine 2021;10(1):e100132 doi: 10.7363/100132 Received: 2019 Aug 22; revised: 2020 Jan 26; accepted: 2020 Feb 02; published online: 2020 Dec 28 Original article Mean platelet volume in asymptomatic chorioamnionitis- exposed infants. A retrospective case-control study Atef Alshafei, Moustafa Hassan, Yaser El saba, Anwar Khan, Mahmoud Ahmed Neonatology Section, Pediatric Department, Dubai Hospital, Dubai, UAE Abstract Introduction: Maternal chorioamnionitis (CA) is a serious condition causing several neonatal morbidities and long-term neurodevelopmental sequelae in exposed infants. Current guidelines still recommend admission, laboratory evaluation, and antibiotic administration to all CA-exposed infants. The incidence of early-onset neonatal sepsis (EOS) is currently low, owing to the routine intrapartum antibiotic administration to mothers identified to be at risk of developing CA. New diagnostic tools for early diagnosis of sepsis in apparently healthy infants exposed to maternal CA are needed. Previous studies showed that mean platelet volume (MPV) is evolving as a potential inflammatory marker of neonatal sepsis. We aimed to study whether MPV can be used as an adjuvant diagnostic tool for EOS in asymptomatic CA-exposed infants. Objective: To evaluate the role of MPV as an adjuvant biomarker of EOS in cases of asymptomatic CA-exposed infants. Design: Retrospective case-control study. Setting: A tertiary care Neonatal Intensive Care Unit (NICU). Patients: Asymptomatic CA-exposed infants 37-40 weeks of gestation admitted between May 2016 and April 2019 to the NICU of Dubai Hospital, UAE. Results: A total of 1,300 infants were admitted to NICU during the study period.