NIH Public Access Author Manuscript J Neuroimmunol
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

IN the UNITED STATES COURT of FEDERAL CLAIMS OFFICE of SPECIAL MASTERS No. 01-162V Filed: February 12, 2009 to Be Published
IN THE UNITED STATES COURT OF FEDERAL CLAIMS OFFICE OF SPECIAL MASTERS No. 01-162V Filed: February 12, 2009 To Be Published * * * * * * * * * * * * * * * * * * * * * * * * * * * * COLTEN SNYDER, by and through * KATHRYN SNYDER and JOSEPH SNYDER, * his natural guardians and next friends * Omnibus Autism * Proceeding; * Autism Spectrum Disorder, * Pervasive Developmental * Disorder, Causation, Petitioners, * Measles, MMR, Mercury, * Thimerosal, Waiver v. * Applying Daubert, * Weight of Expert Opinions, SECRETARY OF THE DEPARTMENT * Credibility of Witnesses OF HEALTH AND HUMAN SERVICES, * * Respondent. * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * Christopher W. Wickersham, Sr., Esq., Lloyd Bowers, Esq., and Thomas B. Powers, Esq., for petitioners. Alexis S. Babcock, Esq., Katherine Esposito, Esq., Voris Johnson, Esq., and Vincent Matanoski, Esq., U.S. Department of Justice, Washington, DC, for respondent. DECISION1 Vowell, Special Master: On March 22, 2001, Kathryn and Joseph Snyder [“petitioners”] filed a petition for compensation under the National Vaccine Injury Compensation Program, 42 U.S.C. 1 Vaccine Rule 18(b) provides the parties 14 days to request redaction of any material “(i) which is trade secret or commercial or financial information which is privileged and confidential, or (ii) which are medical files and similar files, the disclosure of which would constitute a clearly unwarranted invasion of privacy.” 42 U.S.C. § 300aa12(d)(4)(B). Petitioners have waived their right to request such redaction. See Petitioners’ Notice to W aive the 14-Day “W aiting” Period as Defined in Vaccine Rule 18(b), filed December 2, 2008. Respondent also waived the right to object to the disclosure of information submitted by respondent. See Respondent’s Consent to Disclosure, filed January 14, 2009. Accordingly, this decision will be publicly available immediately after it is filed. -
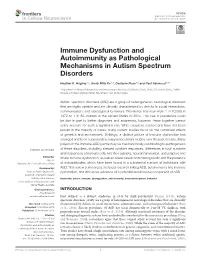
Immune Dysfunction and Autoimmunity As Pathological Mechanisms in Autism Spectrum Disorders
REVIEW published: 13 November 2018 doi: 10.3389/fncel.2018.00405 Immune Dysfunction and Autoimmunity as Pathological Mechanisms in Autism Spectrum Disorders Heather K. Hughes 1,2, Emily Mills Ko 1,2, Destanie Rose 1,2 and Paul Ashwood 1,2* 1 Department of Medical Microbiology and Immunology, University of California, Davis, Davis, CA, United States, 2 MIND Institute, UC Davis Medical Center, Sacramento, CA, United States Autism spectrum disorders (ASD) are a group of heterogeneous neurological disorders that are highly variable and are clinically characterized by deficits in social interactions, communication, and stereotypical behaviors. Prevalence has risen from 1 in 10,000 in 1972 to 1 in 59 children in the United States in 2014. This rise in prevalence could be due in part to better diagnoses and awareness, however, these together cannot solely account for such a significant rise. While causative connections have not been proven in the majority of cases, many current studies focus on the combined effects of genetics and environment. Strikingly, a distinct picture of immune dysfunction has emerged and been supported by many independent studies over the past decade. Many players in the immune-ASD puzzle may be mechanistically contributing to pathogenesis of these disorders, including skewed cytokine responses, differences in total numbers and frequencies of immune cells and their subsets, neuroinflammation, and adaptive and Edited by: innate immune dysfunction, as well as altered levels of immunoglobulin and the presence Jijun Li, Shanghai Jiao Tong University, China of autoantibodies which have been found in a substantial number of individuals with Reviewed by: ASD. This review summarizes the latest research linking ASD, autoimmunity and immune Andreas Martin Grabrucker, dysfunction, and discusses evidence of a potential autoimmune component of ASD. -

Different Minds
DIFFERENT MINDS if there’s one thing Ralph Or not. the fact that there are few AN INFECTIOUS THEORY Adolphs wants you to under- absolutes is part of why the set of dis- Much of that insight comes from Pat- stand about autism, it’s this: “it’s orders—autism, Asperger’s, pervasive terson, who pioneered the study of the wrong to call many of the people developmental disorder not otherwise connections between the brain and the on the autism spectrum impaired,” says specified (PDD-NOS)—that fall under immune system in autism, schizophrenia, the Caltech neuroscientist. “they’re autism’s umbrella are referred to as and depression a decade ago. simply different.” a spectrum. As with the spectrum of the main focus of that connection? these differences are in no way insig- visible light—where red morphs into Some kind of viral infection during preg- nificant—they are, after all, why so much orange, which morphs into yellow— nancy, Patterson explains. Or, rather, the effort and passion is being put into un- it is difficult to draw sharp lines immune response that infection inevitably derstanding autism’s most troublesome between the various diagnoses in engenders. traits—but neither are they as inevitably the autism spectrum. to bolster his argument, Patterson devastating as has often been depicted. And, like the autism spectrum itself, points to a recent study by hjordis O. they are simply differences; intriguing, the spectrum of autism research at Atladottir of Aarhus University, Denmark, fleeting glimpses into minds that work in Caltech also runs a gamut. Adolphs, and colleagues—“an extraordinary look at ways most of us don’t quite understand, for example, studies brain differences over 10,000 autism cases” in the Danish and yet which may ultimately give each between adults on the high-functioning Medical Register, which is a comprehen- and every one of us a little more insight portion of the autism spectrum and the sive database of every Dane’s medical into our own minds, our own selves. -

UC San Francisco Electronic Theses and Dissertations
UCSF UC San Francisco Electronic Theses and Dissertations Title Anticipating Autism: Navigating Science, Uncertainty, and Care in the Post-Genomic Era Permalink https://escholarship.org/uc/item/3h13w1wf Author Lappe, Martine Danielle Publication Date 2012 Peer reviewed|Thesis/dissertation eScholarship.org Powered by the California Digital Library University of California Anticipating Autism: Navigating Science, Uncertainty, and Care in the Post-Genomic Era by Martine Danielle Lappe DISSERTATION Submitted in partial satisfaction of the requirements for the degree of DOCTOR OF PHILOSOPHY in Sociology in the GRADUATE DIVISION of the UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Copyright 2012 by Martine Danielle Lappé ii ACKNOWLEDGEMENTS This dissertation would not have been possible without the generosity and support of many people. I want to especially thank the parents, scientists and advocates who shared their experiences and perspectives with me, answering my questions with patience and candor. This research would not have been possible without them. I also owe a debt of gratitude to the coordinators and staff of the epidemiologic study I followed. I want to thank Kristine Wise and McKenzie Oliver in particular, for going above and beyond to help facilitate my research. I have been very fortunate to have an incredibly thoughtful, generous and inspiring dissertation committee to guide me through this process. My chair Adele Clarke has been a trusted resource and caring advisor. Her mentorship has nourished my thinking and supported this project from its beginning. I am particularly grateful to her for helping me make important theoretical and empirical connections, and for always asking thought-provoking questions. This dissertation would not have been possible without her incredible balance of cheerleading and encouragement, cultivated over an inspiring career. -

IN the UNITED STATES COURT of FEDERAL CLAIMS OFFICE of SPECIAL MASTERS No
IN THE UNITED STATES COURT OF FEDERAL CLAIMS OFFICE OF SPECIAL MASTERS No. 01-162V Filed: February 12, 2009 To Be Published * * * * * * * * * * * * * * * * * * * * * * * * * * * * COLTEN SNYDER, by and through * KATHRYN SNYDER and JOSEPH SNYDER, * his natural guardians and next friends * Omnibus Autism * Proceeding; * Autism Spectrum Disorder, * Pervasive Developmental * Disorder, Causation, Petitioners, * Measles, MMR, Mercury, * Thimerosal, Waiver v. * Applying Daubert, * Weight of Expert Opinions, SECRETARY OF THE DEPARTMENT * Credibility of Witnesses OF HEALTH AND HUMAN SERVICES, * * Respondent. * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * Christopher W. Wickersham, Sr., Esq., Lloyd Bowers, Esq., and Thomas B. Powers, Esq., for petitioners. Alexis S. Babcock, Esq., Katherine Esposito, Esq., Voris Johnson, Esq., and Vincent Matanoski, Esq., U.S. Department of Justice, Washington, DC, for respondent. DECISION1 Vowell, Special Master: On March 22, 2001, Kathryn and Joseph Snyder [“petitioners”] filed a petition for compensation under the National Vaccine Injury Compensation Program, 42 U.S.C. 1 Vaccine Rule 18(b) provides the parties 14 days to request redaction of any material “(i) which is trade secret or commercial or financial information which is privileged and confidential, or (ii) which are medical files and similar files, the disclosure of which would constitute a clearly unwarranted invasion of privacy.” 42 U.S.C. § 300aa12(d)(4)(B). Petitioners have waived their right to request such redaction. See Petitioners’ Notice to W aive the 14-Day “W aiting” Period as Defined in Vaccine Rule 18(b), filed December 2, 2008. Respondent also waived the right to object to the disclosure of information submitted by respondent. See Respondent’s Consent to Disclosure, filed January 14, 2009. Accordingly, this decision will be publicly available immediately after it is filed. -
IMFAR 2004 Program Book
2004 PROGRAM Friday & Saturday May 7 – 8, 2004 The Hyatt Hotel Sacramento, California 1 I M F A R Acknowledgements Board Members Program Committee President David Amaral Linda Daly Marian Sigman, PhD University of California, Davis University of California, Los MIND Institute Petrus de Vries Angeles Cambridge University Anthony Bailey Oxford University Glen Dunlap Vice President Sally Rogers, PhD University of South Florida Grace Baranek University of California, Davis University of North Carolina at MIND Institute Chapel Hill Deborah Fein University of Connecticut Treasurer Simon Baron-Cohen Edwin Cook, MD Cambridge University Eric Fombonne University of Chicago McGill University Marlene Behrmann Secretary Carnegie Mellon University Christopher Gillberg Diane Chugani, PhD Hill Goldsmith Wayne State University Susan Bookheimer University of California, Los University of Wisconsin Program Chair Angeles Robin Hansen Nancy Minshew, MD University of California, Davis University of Pittsburgh Medical Dermot Bowler City University Center Sandra Harris Rutgers University Membership Chair Marie Bristol-Power Robert Schultz, PhD Robert Hendren Yale University Jacob Burak University of California, Davis McGill University Nominations Chair Susan Hyman Joseph Piven, MD Tony Charman University of Rochester University of North Carolina University College London Chapel Hill Bob Joseph Diane Chugani Boston University School of Publications Chair Wayne State University/ Medicine David Amaral, PhD Children’s Hospital of Michigan University of California, -

2014 2 Brain & Behavior Research Foundation
BRAIN & BEHAVIOR RESEARCH FOUNDATION Research for Better Treatments and Cures ANNUAL REPORT 2014 2 BRAIN & BEHAVIOR RESEARCH FOUNDATION Our Vision Our History / Who We Are To dramatically improve The Foundation began as a family movement and has become the world’s the lives of those with mental illness leading private funder of mental health research grants. The Foundation and ultimately enable people to live funds the most innovative ideas in neuroscience and psychiatry to better full, happy and productive lives. understand the causes and develop new ways to effectively treat brain and behavior disorders. These disorders include depression, bipolar disorder, schizophrenia, autism, attention-deficit hyperactivity disorder, anxiety, borderline personality disorder, obsessive-compulsive disorder and post-traumatic stress disorder. The first NARSAD Grants were awarded in 1987. Since then the Foundation has awarded more than $324 million to fund more than 4,800 grants to more than 3,800 leading scientists around the world. This has led to over $3 billion in additional funding for these scientists. ANNUAL REPORT 2014 3 How We Do It Our Values 100% of dollars raised for research are invested in grants leading to advances • We believe better treatments and and breakthroughs in brain and behavior research. breakthroughs come from scien- tific discovery. Our grants support a broad range of the best ideas in brain research. • We fund only those scientists Funding for our grants is focused on three priority areas to better understand whose research is reviewed and and treat mental illness, aiming toward prevention and ultimately cures: recommended by our world-re- nowned Scientific Council. -
IMFAR-Prgm-Bk2011:San Diego.Qxd
International Meeting for Autism Research May 12 -14, 2011 Manchester Grand Hyatt n San Diego, California www.autism-insar.org PROGRAM BOOK IMFAR WELCOME IMFAR is celebrating its 10th anniversary and returning to the site of the first conference, San Diego! We are delighted to welcome everyone to what we feel is our best meeting yet. We believe we have planned a very exciting and informative three days covering the very latest in research focusing on autism. This year the Scientific Program Committee reviewed over 1,000 abstracts from around the world and has put together a solid meeting. As Scientific Program Chair, Dan Geschwind, notes in his remarks, there are a few new events planned in addition to several of IMFAR’s popular features including the Invited Educational Symposia, exceptional keynote speakers, oral sessions, poster presentations, Lifetime Achievement Award and Special Interest Group meetings. We also have a few special surprises planned for the main reception following the presentation of the Lifetime Achievement Award so do not miss it. Planning a meeting like this requires the efforts of some very special people and I would like to acknowledge those who contributed so much of their time and effort to INSAR and the IMFAR event. Along these lines I would like to thank the INSAR Board, the Scientific Program Committee, and the many abstract reviewers who helped ensure the inclusion of the best in autism research. A special thank you goes to Joe Dymek of ConferenceDirect whose invaluable assistance made the job of planning the meeting a pleasure. I would like also to personally acknowledge the members of the Meeting Planning Committee who have worked very hard to make the 2011 IMFAR experience special. -
Program Book
Kursaal Centre Donostia / San Sebastián, Spain IMFAR WELCOME Bienvenidos! Ongi etorri! We are very excited to have IMFAR for the first time in continental Europe and in the beautiful town of Donostia / San Sebastián, in the Basque Country of Spain! We hope you will enjoy some of our attractions, including its famous gastronomic offers, the impressive beaches and the Old Quarter. All the sessions in the main auditorium will offer simultaneous translation into Basque, French and Spanish, making this IMFAR truly international. There is a wonderful program planned for you. The Scientific Program Committee reviewed a record number of abstracts, and under the leadership of Dr. Thomas Bourgeron has planned what is sure to be an outstanding meeting. The keynote speakers will excite and inspire with new information and perspectives from research into autism and other fields of study. The Educational Symposia cover diverse topics and integrate basic and clinical sciences, and the Oral and Poster Sessions promise to be superb. Other highlights will include the Special Interest Group meetings, the ‘Meet the Experts’ luncheon for trainees, and the always popular Innovative Technology Demonstration Session. The Lifetime Achievement Award and Advocate Award presentations are sure to be memorable. The Basque Government invites you to our San Telmo Museum, an old Dominican convent from the mid-sixteenth century, for a reception on Thursday night that will embed you in our local culture! This year’s meeting would not have been possible without the tireless efforts of many special people. I would like to acknowledge and thank the INSAR Board for their support and guidance, as well as the Scientific Program Committees, both the Executive Scientific Committee and the main Scientific Committee, and the many abstract reviewers who have striven to ensure the excellence of the science presented at IMFAR. -

Autism Research and Treatment
Autism Research and Treatment Autism: Where Genetics Meets the Immune System Guest Editors: Antonio M. Persico, Judy Van de Water, and Carlos A. Pardo Autism: Where Genetics Meets the Immune System Autism Research and Treatment Autism: Where Genetics Meets the Immune System Guest Editors: Antonio M. Persico, Judy Van de Water, and Carlos A. Pardo Copyright © 2012 Hindawi Publishing Corporation. All rights reserved. This is a special issue published in “Autism Research and Treatment.” All articles are open access articles distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Editorial Board Jean-Louis Adrien, France Mohammad Ghaziuddin, USA Klaus-Peter Ossenkopp, Canada M. Aman, USA Barry Gordon, USA Alan K. Percy, USA Elizabeth Aylward, USA H. Jyonouchi, USA Mikhail V. Pletnikov, USA R. F. Berman, USA Connie Kasari, USA Herbert Roeyers, Belgium Roberto Canitano, Italy Walter E. Kaufmann, USA John A. Sweeney, USA Manuel F. Casanova, USA Bryan King, USA Akio Wakabayashi, UK Jamel Chelly, France N. Kraus, USA Geraldine Dawson, USA Bennett L. Leventhal, USA Valsamma Eapen, Australia M.-Reza Mohammadi, Iran Contents Autism: Where Genetics Meets the Immune System, Antonio M. Persico, Judy Van de Water, and Carlos A. Pardo Volume 2012, Article ID 486359, 2 pages Is Autism a Member of a Family of Diseases Resulting from Genetic/Cultural Mismatches? Implications for Treatment and Prevention, Staci D. Bilbo, John P. Jones, and William Parker Volume 2012, Article ID 910946, 11 pages Prenatal and Postnatal Epigenetic Programming: Implications for GI, Immune, and Neuronal Function in Autism, Mostafa I. -

Interagency Autism Coordinating Committee
1 INTERAGENCY AUTISM COORDINATING COMMITTEE HEALTH OUTCOMES WORKING GROUP THURSDAY, SEPTEMBER 27, 2018 The Interagency Autism Coordinating Committee (IACC) Health Outcomes Working Group convened in Rockville, Maryland, at the National Institute of Mental Health (NIMH), 6001 Executive Blvd., at 8:37 a.m., David Amaral, Ph.D. and Julie Lounds Taylor, Ph.D., Co- Chairs, presiding. PRESENT: SUSAN DANIELS, Ph.D., Executive Secretary, IACC, Office of Autism Research Coordination (OARC), NIMH DAVID AMARAL, Ph.D., Co-Chair, IACC WG, University of California, Davis, (UC) JULIE LOUNDS TAYLOR, Ph.D., Co-Chair, IACC WG, Vanderbilt University SHELLI AVENEVOLI, Ph.D., (representing NIMH) GREGORY BARNES, M.D., Ph.D., University of Louisville School of Medicine TIMOTHY BUIE, M.D., Harvard Medical School JUDITH COOPER, Ph.D., National Institute on Deafness and other Communication Disorders (NIDCD) 2 PRESENT: (continued) DAN COURY, M.D., The Ohio State University College of Medicine SAMANTHA CRANE, J.D., Autistic Self Advocacy Network (ASAN) GERALDINE DAWSON, Ph.D., Duke University PATRICIA DIETZ, Dr.P.H., M.P.H., U.S. Centers for Disease Control and Prevention (CDC) SARAH GARDNER, University of California, Davis (attended by phone) DENA GASSNER, M.S.W., Adelphi University ANTONIO HARDAN, M.D., Stanford University Medical Center JENNIFER JOHNSON, Ed.D., U.S. Department of Health and Human Services (HHS) JOSEPH JOYCE, M.B.A., Autism Society of America (attended by Phone) DENISE JULIANO-BULT, M.S.W., NIMH ALICE KAU, Ph.D., Eunice Kennedy Shriver National -
Consensus Paper: Pathological Role of the Cerebellum in Autism
Cerebellum (2012) 11:777–807 DOI 10.1007/s12311-012-0355-9 REVIEW Consensus Paper: Pathological Role of the Cerebellum in Autism S. Hossein Fatemi & Kimberly A. Aldinger & Paul Ashwood & Margaret L. Bauman & Charles D. Blaha & Gene J. Blatt & Abha Chauhan & Ved Chauhan & Stephen R. Dager & Price E. Dickson & Annette M. Estes & Dan Goldowitz & Detlef H. Heck & Thomas L. Kemper & Bryan H. King & Loren A. Martin & Kathleen J. Millen & Guy Mittleman & Matthew W. Mosconi & Antonio M. Persico & John A. Sweeney & Sara J. Webb & John P. Welsh Published online: 28 February 2012 # Springer Science+Business Media, LLC 2012 Abstract There has been significant advancement in various the pathology of autism. Recent emergent findings in literature aspects of scientific knowledge concerning the role of related to cerebellar involvement in autism are discussed, cerebellum in the etiopathogenesis of autism. In the including: cerebellar pathology, cerebellar imaging and current consensus paper, we will observe the diversity of symptom expression in autism, cerebellar genetics, cerebellar opinions regarding the involvement of this important site in immune function, oxidative stress and mitochondrial S. H. Fatemi (*) G. J. Blatt University of Minnesota Medical School, Department of Anatomy and Neurobiology, 420 Delaware St. SE, MMC 392, Boston University School of Medicine, Minneapolis, MN 55455, USA Boston, MA, USA e-mail: [email protected] A. Chauhan : V. Chauhan K. A. Aldinger NYS Institute for Basic Research in Developmental Disabilities, Zilkha Neurogenetic Institute, Keck School of Medicine, Staten Island, NY, USA University of Southern California, Los Angeles, USA S. R. Dager Departments of Radiology and Bioengineering, P. Ashwood University of Washington, Department of Medical Microbiology and Immunology, Seattle, USA The Medical Investigation of Neurodevelopmental Disorders : (M.I.N.D.) Institute, University of California, S.