Managing Your Scar
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Review of the Evidence for and Against a Role for Mast Cells in Cutaneous Scarring and Fibrosis
International Journal of Molecular Sciences Review A Review of the Evidence for and against a Role for Mast Cells in Cutaneous Scarring and Fibrosis Traci A. Wilgus 1,*, Sara Ud-Din 2 and Ardeshir Bayat 2,3 1 Department of Pathology, Ohio State University, Columbus, OH 43210, USA 2 Centre for Dermatology Research, NIHR Manchester Biomedical Research Centre, Plastic and Reconstructive Surgery Research, University of Manchester, Manchester M13 9PT, UK; [email protected] (S.U.-D.); [email protected] (A.B.) 3 MRC-SA Wound Healing Unit, Division of Dermatology, University of Cape Town, Observatory, Cape Town 7945, South Africa * Correspondence: [email protected]; Tel.: +1-614-366-8526 Received: 1 October 2020; Accepted: 12 December 2020; Published: 18 December 2020 Abstract: Scars are generated in mature skin as a result of the normal repair process, but the replacement of normal tissue with scar tissue can lead to biomechanical and functional deficiencies in the skin as well as psychological and social issues for patients that negatively affect quality of life. Abnormal scars, such as hypertrophic scars and keloids, and cutaneous fibrosis that develops in diseases such as systemic sclerosis and graft-versus-host disease can be even more challenging for patients. There is a large body of literature suggesting that inflammation promotes the deposition of scar tissue by fibroblasts. Mast cells represent one inflammatory cell type in particular that has been implicated in skin scarring and fibrosis. Most published studies in this area support a pro-fibrotic role for mast cells in the skin, as many mast cell-derived mediators stimulate fibroblast activity and studies generally indicate higher numbers of mast cells and/or mast cell activation in scars and fibrotic skin. -

Wound Healing: a Paradigm for Regeneration
SYMPOSIUM ON REGENERATIVE MEDICINE Wound Healing: A Paradigm for Regeneration Victor W. Wong, MD; Geoffrey C. Gurtner, MD; and Michael T. Longaker, MD, MBA From the Hagey Laboratory for Pediatric Regenerative Medi- CME Activity cine, Department of Surgery, Stanford University, Stanford, Target Audience: The target audience for Mayo Clinic Proceedings is primar- relationships with any commercial interest related to the subject matter ily internal medicine physicians and other clinicians who wish to advance of the educational activity. Safeguards against commercial bias have been CA. their current knowledge of clinical medicine and who wish to stay abreast put in place. Faculty also will disclose any off-label and/or investigational of advances in medical research. use of pharmaceuticals or instruments discussed in their presentation. Statement of Need: General internists and primary care physicians must Disclosure of this information will be published in course materials so maintain an extensive knowledge base on a wide variety of topics covering that those participants in the activity may formulate their own judgments all body systems as well as common and uncommon disorders. Mayo Clinic regarding the presentation. Proceedings aims to leverage the expertise of its authors to help physicians In their editorial and administrative roles, William L. Lanier, Jr, MD, Terry L. understand best practices in diagnosis and management of conditions Jopke, Kimberly D. Sankey, and Nicki M. Smith, MPA, have control of the encountered in the clinical setting. content of this program but have no relevant financial relationship(s) with Accreditation: College of Medicine, Mayo Clinic is accredited by the Accred- industry. itation Council for Continuing Medical Education to provide continuing med- The authors report no competing interests. -

Post-Summer Skin Repair
36 RIVIERA WELLNESS POST-SUMMER SKIN REPAIR Healthy, radiant skin begins from within season of summer indulgences, whe- Niacin (B3) is found in avocado and turkey and ther it be swimming in chlorinated pools, helps to speed up skin cell regeneration - essen- A several weeks of rosé wine, or too much tial for repairing sun damage, acne hyperpigmen- sun bathing, our skin can look a little worse for tation, and reduces the symptoms of rosacea. wear. Once the summer holidays are over, we Niacin also helps your skin to retain moisture, so can be left with dehydrated and perhaps wrinkly make sure you are properly hydrated! Turkey has skin, sun damage, blocked pores and chapped 30 x more niacin than avocado. lips. So what´s the best remedy? Good nutrition Green Tea - Epigallocatechin gallate (EGCG), the can help protect the skin not just pre-holiday antioxidant found in green tea has been shown season, but also post-holiday to help the skin re- prevent genetic damage in skin cells exposed to pair. UV radiation. A large mug of green tea (250ml) The skin can be thought of as the window to ove- with a squeeze of fresh lemon juice to add the rall health of the body. It is the largest elimination vitamin C may help achieve that post-summer route for toxins, so an overworked liver from a glow! long summer of excesses can show up on the skin. The simplest step to a fresher complexion DON´T FORGET is to address water intake. Well-hydrated skin LIFESTYLE FACTORS! looks plump and less wrinkled. -

Fundamentals of Dermatology Describing Rashes and Lesions
Dermatology for the Non-Dermatologist May 30 – June 3, 2018 - 1 - Fundamentals of Dermatology Describing Rashes and Lesions History remains ESSENTIAL to establish diagnosis – duration, treatments, prior history of skin conditions, drug use, systemic illness, etc., etc. Historical characteristics of lesions and rashes are also key elements of the description. Painful vs. painless? Pruritic? Burning sensation? Key descriptive elements – 1- definition and morphology of the lesion, 2- location and the extent of the disease. DEFINITIONS: Atrophy: Thinning of the epidermis and/or dermis causing a shiny appearance or fine wrinkling and/or depression of the skin (common causes: steroids, sudden weight gain, “stretch marks”) Bulla: Circumscribed superficial collection of fluid below or within the epidermis > 5mm (if <5mm vesicle), may be formed by the coalescence of vesicles (blister) Burrow: A linear, “threadlike” elevation of the skin, typically a few millimeters long. (scabies) Comedo: A plugged sebaceous follicle, such as closed (whitehead) & open comedones (blackhead) in acne Crust: Dried residue of serum, blood or pus (scab) Cyst: A circumscribed, usually slightly compressible, round, walled lesion, below the epidermis, may be filled with fluid or semi-solid material (sebaceous cyst, cystic acne) Dermatitis: nonspecific term for inflammation of the skin (many possible causes); may be a specific condition, e.g. atopic dermatitis Eczema: a generic term for acute or chronic inflammatory conditions of the skin. Typically appears erythematous, -

Advances in Seborrheic Keratosis
A CME/CE-Certified Supplement to Original Release Date: December 2018 Advances in Seborrheic Expiration Date: December 31, 2020 Estimated Time To Complete Activity: 1 hour Participants should read the activity information, Keratosis review the activity in its entirety, and complete the online post-test and evaluation. Upon completing this activity as designed and achieving a passing score on FACULTY the post-test, you will be directed to a Web page that will Joseph F. Fowler Jr, MD Michael S. Kaminer, MD allow you to receive your certificate of credit via e-mail Clinical Professor and Director Associate Clinical Professor of Dermatology or you may print it out at that time. Contact and Occupational Yale Medical School The online post-test and evaluation can be accessed Dermatology New Haven, Connecticut at http://tinyurl.com/SebK2018. University of Louisville School of Adjunct Assistant Professor of Medicine Medicine (Dermatology), Warren Alpert Medical School Inquiries about continuing medical education (CME) Louisville, Kentucky of Brown University accreditation may be directed to the University of Providence, Rhode Island Louisville Office of Continuing Medical Education & Professional Development (CME & PD) at cmepd@ louisville.edu or (502) 852-5329. Designation Statement eborrheic keratosis (SK) has been called keratinizing surface.12 They can develop virtually The University of Louisville School of Medicine the “Rodney Dangerfield of skin lesions”— anywhere except for the palms, soles, and mucous designates this Enduring material for a maximum of 9 1.0 AMA PRA Category 1 Credit(s)™. Physicians should it earns little respect (as a clinical concern) membranes, but are most commonly observed claim only the credit commensurate with the extent of Sbecause of its benignity, commonality, usual on the trunk and face.6,13 The tendency to develop their participation in the activity. -

Linear Scleroderma “En Coup De Sabre” Coexisting with Plaque-Morphea
661 J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.74.5.661 on 1 May 2003. Downloaded from SHORT REPORT Linear scleroderma “en coup de sabre” coexisting with plaque-morphea: neuroradiological manifestation and response to corticosteroids I Unterberger, E Trinka, K Engelhardt, A Muigg, P Eller, M Wagner, N Sepp, G Bauer ............................................................................................................................. J Neurol Neurosurg Psychiatry 2003;74:661–664 progression of skin lesions or any neurological abnormalities A 24 year old woman in the 33rd week of pregnancy during follow up. developed progressive neurological complications with On admission the patient was in the 33rd week of right sided hemiparesis in association with the occurrence pregnancy. She was fully oriented, had normal speech, and of linear scleroderma “en coup de sabre” (LSCS) and pre- presented with a right sided hemiparesis (grade 3/5, MRC existing plaque-morphea, already being treated by scale) with a positive Babinski sign on the right. There was no balneophototherapy. Further progression of neurological history of head trauma. symptoms led to a caesarean section with the delivery of a Routine laboratory testing and comprehensive serological healthy child. Brain magnetic resonance imaging (MRI) screening including antineutrophilic cytoplasmic antibodies showed focal T2 signal increases in the left frontoparietal (ANCA), anticardiolipin antibodies, and antibodies against region directly adjacent to the area of LSCS. -
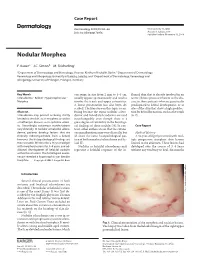
Nodular Morphea
Case Report Dermatology 2009;218:63–66 Received: July 13, 2008 DOI: 10.1159/000173976 Accepted: July 23, 2008 Published online: November 13, 2008 Nodular Morphea a b c F. Kauer J.C. Simon M. Sticherling a b Department of Dermatology and Venerology, Vivantes Klinikum Neukölln, Berlin , Department of Dermatology, c Venerology and Allergology, University of Leipzig, Leipzig , and Department of Dermatology, Venerology and Allergology, University of Erlangen, Erlangen , Germany Key Words can range in size from 2 mm to 4–5 cm, flamed skin that is already involved in an -Scleroderma ؒ Keloid ؒ Hypertrophic scar ؒ usually appear spontaneously and tend to active fibrotic process inherent to the dis Morphea involve the trunk and upper extremities. ease in those patients who are genetically A linear presentation has also been de- predisposed to keloid development, or at scribed. The literature on this topic is con- sites of the skin that show a high predilec- Abstract fusing because the terms ‘nodular sclero- tion for keloid formation, such as the trunk Scleroderma may present as being strictly derma’ and ‘keloidal scleroderma’ are used [6, 7] . limited to the skin, as in morphea, or within interchangeably even though there is a a multiorgan disease, as in systemic sclero- great degree of variability in the histologi- sis. Accordingly, cutaneous manifestations cal findings of these nodules [4] . In con- C a s e R e p o r t vary clinically. In nodular or keloidal sclero- trast, other authors stress that the cutane- derma, patients develop lesions that are ous manifestations may vary clinically, but Medical History clinically indistinguishable from a keloid; all share the same histopathological pat- A 16-year-old girl presented with mul- however, the histopathological findings are tern of both morphea/scleroderma and ke- tiple progressive morpheic skin lesions more variable. -

Sweat Glands • Oil Glands • Mammary Glands
Chapter 4 The Integumentary System Lecture Presentation by Steven Bassett Southeast Community College © 2015 Pearson Education, Inc. Introduction • The integumentary system is composed of: • Skin • Hair • Nails • Sweat glands • Oil glands • Mammary glands © 2015 Pearson Education, Inc. Introduction • The skin is the most visible organ of the body • Clinicians can tell a lot about the overall health of the body by examining the skin • Skin helps protect from the environment • Skin helps to regulate body temperature © 2015 Pearson Education, Inc. Integumentary Structure and Function • Cutaneous Membrane • Epidermis • Dermis • Accessory Structures • Hair follicles • Exocrine glands • Nails © 2015 Pearson Education, Inc. Figure 4.1 Functional Organization of the Integumentary System Integumentary System FUNCTIONS • Physical protection from • Synthesis and storage • Coordination of immune • Sensory information • Excretion environmental hazards of lipid reserves response to pathogens • Synthesis of vitamin D3 • Thermoregulation and cancers in skin Cutaneous Membrane Accessory Structures Epidermis Dermis Hair Follicles Exocrine Glands Nails • Protects dermis from Papillary Layer Reticular Layer • Produce hairs that • Assist in • Protect and trauma, chemicals protect skull thermoregulation support tips • Nourishes and • Restricts spread of • Controls skin permeability, • Produce hairs that • Excrete wastes of fingers and supports pathogens prevents water loss provide delicate • Lubricate toes epidermis penetrating epidermis • Prevents entry of -

Genetics of Hair and Skin Color
11 Sep 2003 14:51 AR AR201-GE37-04.tex AR201-GE37-04.sgm LaTeX2e(2002/01/18) P1: GCE 10.1146/annurev.genet.37.110801.143233 Annu. Rev. Genet. 2003. 37:67–90 doi: 10.1146/annurev.genet.37.110801.143233 Copyright c 2003 by Annual Reviews. All rights reserved First published online as a Review in Advance on June 17, 2003 GENETICS OF HAIR AND SKIN COLOR Jonathan L. Rees Systems Group, Dermatology, University of Edinburgh, Lauriston Buildings, Lauriston Place, Edinburgh, EH3 9YW, United Kingdom; email: [email protected] Key Words melanin, melanocortin 1 receptor (MC1R), eumelanin, pheomelanin, red hair ■ Abstract Differences in skin and hair color are principally genetically deter- mined and are due to variation in the amount, type, and packaging of melanin polymers produced by melanocytes secreted into keratinocytes. Pigmentary phenotype is genet- ically complex and at a physiological level complicated. Genes determining a number of rare Mendelian disorders of pigmentation such as albinism have been identified, but only one gene, the melanocortin 1 receptor (MCR1), has so far been identified to explain variation in the normal population such as that leading to red hair, freckling, and sun-sensitivity. Genotype-phenotype relations of the MC1R are reviewed, as well as methods to improve the phenotypic assessment of human pigmentary status. It is argued that given advances in model systems, increases in technical facility, and the lower cost of genotype assessment, the lack of standardized phenotype assessment is now a major limit on advance. CONTENTS INTRODUCTION ..................................................... 68 BIOLOGY OF HUMAN PIGMENTATION ................................ 69 by San Jose State University on 10/05/10. -

Skin 1. Describe the Basic Histological Structure of the Skin, Identifying The
Skin lecture notes 1 Lecture objectives: skin 1. Describe the basic histological structure of the skin, identifying the layers of the skin and their embryologic origin. 2. Identify the cell layers that constitute the epidermis and the differences between thick and thin skin. 3. Describe the cellular components of the epidermis and their function: keratinocytes, melanocytes, Langerhans cells and Merkel cells: 4. Describe the structural organization of the dermis and the components of the papillary and reticular layers. 5. Identify other structures present in the skin: vessels, skin sensorial receptors, hair follicles and hairs, nails and glands. 6. Understand the mechanism of skin repair 7. Describe histological findings in common skin diseases. Skin lecture notes 2 HISTOLOGY OF THE SKIN The skin is the heaviest, largest single organ of the body. It protects the body against physical, chemical and biological agents. The skin participates in the maintenance of body temperature and hydration, and in the excretion of metabolites. It also contributes to homeostasis through the production of hormones, cytokines and growth factors. 1. Describe the basic histological structure of the skin, identifying the layers of the skin and their embryologic origin. The skin is composed of the epidermis, an epithelial layer of ectodermal origin and the dermis, a layer of connective tissue of mesodermal origin. The hypodermis or subcutaneous tissue, which is not considered part of the skin proper, lies deep to the dermis and is formed by loose connective tissue that typically contains adipose cells. Skin layers 2. Identify the cell layers that constitute the epidermis and the differences between thick and thin skin. -

Skin and Soft Tissue Substitutes – Commercial Medical Policy
UnitedHealthcare® Commercial Medical Policy Skin and Soft Tissue Substitutes Policy Number: 2021T0592I Effective Date: August 1, 2021 Instructions for Use Table of Contents Page Related Commercial Policies Coverage Rationale ....................................................................... 1 • Prolotherapy and Platelet Rich Plasma Therapies Documentation Requirements ...................................................... 3 • Breast Reconstruction Post Mastectomy and Poland Definitions ...................................................................................... 4 Syndrome Applicable Codes .......................................................................... 4 Description of Services ................................................................. 7 Community Plan Policy Clinical Evidence ........................................................................... 8 • Skin and Soft Tissue Substitutes U.S. Food and Drug Administration ........................................... 53 Medicare Advantage Coverage Summary References ................................................................................... 54 • Skin Treatment, Services and Procedures Policy History/Revision Information ........................................... 60 Instructions for Use ..................................................................... 60 Coverage Rationale EpiFix® Amnion/Chorion Membrane (Non-Injectable) EpiFix is proven and medically necessary for treating diabetic foot ulcer when all of the following criteria are met: • Adequate -

Acitretin for Hypertrophic Lichen Planus Like Reaction in a Burn Scar
THE CUTTING EDGE SECTION EDITOR: GEORGE J. HRUZA, MD; ASSISTANT SECTION EDITORS: LYNN A. CORNELIUS, MD; JON STARR, MD Acitretin for Hypertrophic Lichen Planus–Like Reaction in a Burn Scar Steven Kossard, FACD; Phillip Artemi, FACD; Skin and Cancer Foundation Australia, Sydney The Cutting Edge: Challenges in Medical and Surgical Therapeutics REPORT OF A CASE men showed changes consistent with an early well- differentiated squamous cell carcinoma. A 60-year-old-man sustained a burn in childhood on the lower part of his right leg in a fire in a haystack. The area THERAPEUTIC CHALLENGE healed and remained as a stable scar for 50 years. Four months before presentation, he developed a series of hy- Squamous cell carcinoma may develop in the setting of pertrophic papules and plaques measuring up to 12 cm either a long-standing burn scar or hypertrophic lichen in diameter localized to the burn scar (Figure 1). The planus. Immunosuppressive agents, such as systemic cor- individual lesions were violaceous and hyperkeratotic. ticosteroids or cyclosporin, are used to treat lichen pla- There were no similar lesions at other skin sites or in- nus but inhibit cell-mediated immune responses that play volvement of his mucous membranes. The patient was a vital role in inhibiting the progression of skin cancers. taking warfarin sodium and digoxin, and 2 months after Clearly, the use of immunosuppressive drugs in our pa- the onset of his skin lesions, he began taking lisinopril tient, who had both a long-standing burn scar and le- for hypertension. sions resembling hypertrophic lichen planus, posed a po- Over the following 5 months, 4 skin biopsy speci- tential risk of enhancing tumor growth.