Advances in Seborrheic Keratosis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Prevalence of Cutaneous Manifestations in Young Patients with Type 1 Diabetes
Clinical Care/Education/Nutrition/Psychosocial Research ORIGINAL ARTICLE The Prevalence of Cutaneous Manifestations in Young Patients With Type 1 Diabetes 1 2 MILOSˇ D. PAVLOVIC´, MD, PHD SLAANA TODOROVIC´, MD tions, such as neuropathic foot ulcers; 2 4 TATJANA MILENKOVIC´, MD ZORANA ÐAKOVIC´, MD and 4) skin reactions to diabetes treat- 1 1 MIROSLAV DINIC´, MD RADOSˇ D. ZECEVIˇ , MD, PHD ment (1). 1 5 MILAN MISOVIˇ C´, MD RADOJE DODER, MD, PHD 3 To understand the development of DRAGANA DAKOVIC´, DS skin lesions and their relationship to dia- betes complications, a useful approach would be a long-term follow-up of type 1 OBJECTIVE — The aim of the study was to assess the prevalence of cutaneous disorders and diabetic patients and/or surveys of cuta- their relation to disease duration, metabolic control, and microvascular complications in chil- neous disorders in younger type 1 dia- dren and adolescents with type 1 diabetes. betic subjects. Available data suggest that skin dryness and scleroderma-like RESEARCH DESIGN AND METHODS — The presence and frequency of skin mani- festations were examined and compared in 212 unselected type 1 diabetic patients (aged 2–22 changes of the hand represent the most years, diabetes duration 1–15 years) and 196 healthy sex- and age-matched control subjects. common cutaneous manifestations of Logistic regression was used to analyze the relation of cutaneous disorders with diabetes dura- type 1 diabetes seen in up to 49% of the tion, glycemic control, and microvascular complications. patients (3). They are interrelated and also related to diabetes duration. Timing RESULTS — One hundred forty-two (68%) type 1 diabetic patients had at least one cutaneous of appearance of various cutaneous le- disorder vs. -

A Review of the Evidence for and Against a Role for Mast Cells in Cutaneous Scarring and Fibrosis
International Journal of Molecular Sciences Review A Review of the Evidence for and against a Role for Mast Cells in Cutaneous Scarring and Fibrosis Traci A. Wilgus 1,*, Sara Ud-Din 2 and Ardeshir Bayat 2,3 1 Department of Pathology, Ohio State University, Columbus, OH 43210, USA 2 Centre for Dermatology Research, NIHR Manchester Biomedical Research Centre, Plastic and Reconstructive Surgery Research, University of Manchester, Manchester M13 9PT, UK; [email protected] (S.U.-D.); [email protected] (A.B.) 3 MRC-SA Wound Healing Unit, Division of Dermatology, University of Cape Town, Observatory, Cape Town 7945, South Africa * Correspondence: [email protected]; Tel.: +1-614-366-8526 Received: 1 October 2020; Accepted: 12 December 2020; Published: 18 December 2020 Abstract: Scars are generated in mature skin as a result of the normal repair process, but the replacement of normal tissue with scar tissue can lead to biomechanical and functional deficiencies in the skin as well as psychological and social issues for patients that negatively affect quality of life. Abnormal scars, such as hypertrophic scars and keloids, and cutaneous fibrosis that develops in diseases such as systemic sclerosis and graft-versus-host disease can be even more challenging for patients. There is a large body of literature suggesting that inflammation promotes the deposition of scar tissue by fibroblasts. Mast cells represent one inflammatory cell type in particular that has been implicated in skin scarring and fibrosis. Most published studies in this area support a pro-fibrotic role for mast cells in the skin, as many mast cell-derived mediators stimulate fibroblast activity and studies generally indicate higher numbers of mast cells and/or mast cell activation in scars and fibrotic skin. -

HEALTH-RELATED QUALITY of LIFE in MORPHEA by NATASHA
HEALTH-RELATED QUALITY OF LIFE IN MORPHEA by NATASHA KLIMAS In collaboration with Angela D. Shedd, M.D., Ira H. Bernstein, Ph.D., and Heidi T. Jacobe, M.D., M.S.C.S. DISSERTATION Presented to the Faculty of the Medical School The University of Texas Southwestern Medical Center In Partial Fulfillment of the Requirements For the Degree of DOCTOR OF MEDICINE WITH DISTINCTION IN RESEARCH The University of Texas Southwestern Medical Center Dallas, TX TABLE OF CONTENTS ABSTRACT …………………………………………… iii INTRODUCTION …………………………………………… iv MATERIALS AND METHODS …………………………………….. v RESULTS ………………….………………………………………… x DISCUSSION …….…………………………………………………………….. xiii KEY MESSAGES………………………………………………………………………….. xvi TABLES AND FIGURES…………………………………………………………………… xvii ACKNOWLEDGEMENTS ………………………………………………………………. xxvi REFERENCES…………………………………………………………………………… xxvii ii ABSTRACT Objective: Little is known about health-related quality of life (HRQOL) of patients with morphea (localized scleroderma). We determined the impact of morphea on HRQOL and clinical and demographic correlates of HRQOL. Methods: Cross sectional survey of Morphea in Adults and Children (MAC) cohort. Results: Morphea impairs HRQOL. Patients were particularly affected with respect to emotional well-being and concerns that the disease will progress to their internal organs. Patients with morphea had worse skin-specific HRQOL than those with other skin diseases, including non-melanoma skin cancer, vitiligo, and alopecia (lowest P <.0001). The morphea population was found to have significantly worse global HRQOL scores than the general U.S. population for all subscales (all P ≤.004) with the exception of bodily pain. Comorbidity (r =.35-.51, P ≤ .0029 -.0001) and symptoms of pruritus (r =.38 -.64, P ≤.001-.0001) and pain (r =.46-.74, P <.0001) were associated with impairment in multiple domains of skin-specific and global HRQOL. -

A Case of Focal Acral Hyperkeratosis
Ann Dermatol Vol. 21, No. 4, 2009 CASE REPORT A Case of Focal Acral Hyperkeratosis Eun Ah Lee, M.D., Hei Sung Kim, M.D., Hyung Ok Kim, M.D., Young Min Park, M.D. Department of Dermatology, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea Focal acral hyperkeratosis (FAH) is a rare genodermatosis the two; FAH does not have elastorrhexis. There has been with an autosomal dominant pattern of inheritance; how- only one previous report of FAH in a Korean patient; a ever, it may also be sporadic. FAH is characterized by 23-year-old female with a non-specific family history of late-onset crateriform keratotic papules, some coalescing in- FAH has been previously described3. We herein report a to plaques, along the borders of the hands and feet. We here- typical case of FAH in a 47-year-old Korean male with an in report a case of FAH in a 47-year-old male with a family autosomal dominant pattern of inheritance. history of similar lesions in three generations. The histo- logical findings revealed focal areas of orthohyperkeratosis CASE REPORT over an area of depressed but otherwise normal epidermis. The dermis showed no specific changes, which dis- A 47-year-old male presented with multiple persistent tinguished this case from acrokeratoelastoidosis, which flesh colored papules on the hands that were first noted shows elastorrhexis of clinically similar lesions. (Ann during early adulthood. The number of lesions had gradu- Dermatol 21(4) 426∼428, 2009) ally increased over the years. -

Fundamentals of Dermatology Describing Rashes and Lesions
Dermatology for the Non-Dermatologist May 30 – June 3, 2018 - 1 - Fundamentals of Dermatology Describing Rashes and Lesions History remains ESSENTIAL to establish diagnosis – duration, treatments, prior history of skin conditions, drug use, systemic illness, etc., etc. Historical characteristics of lesions and rashes are also key elements of the description. Painful vs. painless? Pruritic? Burning sensation? Key descriptive elements – 1- definition and morphology of the lesion, 2- location and the extent of the disease. DEFINITIONS: Atrophy: Thinning of the epidermis and/or dermis causing a shiny appearance or fine wrinkling and/or depression of the skin (common causes: steroids, sudden weight gain, “stretch marks”) Bulla: Circumscribed superficial collection of fluid below or within the epidermis > 5mm (if <5mm vesicle), may be formed by the coalescence of vesicles (blister) Burrow: A linear, “threadlike” elevation of the skin, typically a few millimeters long. (scabies) Comedo: A plugged sebaceous follicle, such as closed (whitehead) & open comedones (blackhead) in acne Crust: Dried residue of serum, blood or pus (scab) Cyst: A circumscribed, usually slightly compressible, round, walled lesion, below the epidermis, may be filled with fluid or semi-solid material (sebaceous cyst, cystic acne) Dermatitis: nonspecific term for inflammation of the skin (many possible causes); may be a specific condition, e.g. atopic dermatitis Eczema: a generic term for acute or chronic inflammatory conditions of the skin. Typically appears erythematous, -

Linear Scleroderma “En Coup De Sabre” Coexisting with Plaque-Morphea
661 J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.74.5.661 on 1 May 2003. Downloaded from SHORT REPORT Linear scleroderma “en coup de sabre” coexisting with plaque-morphea: neuroradiological manifestation and response to corticosteroids I Unterberger, E Trinka, K Engelhardt, A Muigg, P Eller, M Wagner, N Sepp, G Bauer ............................................................................................................................. J Neurol Neurosurg Psychiatry 2003;74:661–664 progression of skin lesions or any neurological abnormalities A 24 year old woman in the 33rd week of pregnancy during follow up. developed progressive neurological complications with On admission the patient was in the 33rd week of right sided hemiparesis in association with the occurrence pregnancy. She was fully oriented, had normal speech, and of linear scleroderma “en coup de sabre” (LSCS) and pre- presented with a right sided hemiparesis (grade 3/5, MRC existing plaque-morphea, already being treated by scale) with a positive Babinski sign on the right. There was no balneophototherapy. Further progression of neurological history of head trauma. symptoms led to a caesarean section with the delivery of a Routine laboratory testing and comprehensive serological healthy child. Brain magnetic resonance imaging (MRI) screening including antineutrophilic cytoplasmic antibodies showed focal T2 signal increases in the left frontoparietal (ANCA), anticardiolipin antibodies, and antibodies against region directly adjacent to the area of LSCS. -
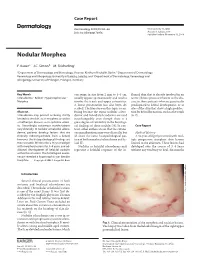
Nodular Morphea
Case Report Dermatology 2009;218:63–66 Received: July 13, 2008 DOI: 10.1159/000173976 Accepted: July 23, 2008 Published online: November 13, 2008 Nodular Morphea a b c F. Kauer J.C. Simon M. Sticherling a b Department of Dermatology and Venerology, Vivantes Klinikum Neukölln, Berlin , Department of Dermatology, c Venerology and Allergology, University of Leipzig, Leipzig , and Department of Dermatology, Venerology and Allergology, University of Erlangen, Erlangen , Germany Key Words can range in size from 2 mm to 4–5 cm, flamed skin that is already involved in an -Scleroderma ؒ Keloid ؒ Hypertrophic scar ؒ usually appear spontaneously and tend to active fibrotic process inherent to the dis Morphea involve the trunk and upper extremities. ease in those patients who are genetically A linear presentation has also been de- predisposed to keloid development, or at scribed. The literature on this topic is con- sites of the skin that show a high predilec- Abstract fusing because the terms ‘nodular sclero- tion for keloid formation, such as the trunk Scleroderma may present as being strictly derma’ and ‘keloidal scleroderma’ are used [6, 7] . limited to the skin, as in morphea, or within interchangeably even though there is a a multiorgan disease, as in systemic sclero- great degree of variability in the histologi- sis. Accordingly, cutaneous manifestations cal findings of these nodules [4] . In con- C a s e R e p o r t vary clinically. In nodular or keloidal sclero- trast, other authors stress that the cutane- derma, patients develop lesions that are ous manifestations may vary clinically, but Medical History clinically indistinguishable from a keloid; all share the same histopathological pat- A 16-year-old girl presented with mul- however, the histopathological findings are tern of both morphea/scleroderma and ke- tiple progressive morpheic skin lesions more variable. -

Early Diagnosis and Treatment of Discoid Lupus Erythematosus
J Am Board Fam Med: first published as 10.3122/jabfm.2009.02.080075 on 5 March 2009. Downloaded from BRIEF REPORT Early Diagnosis and Treatment of Discoid Lupus Erythematosus Suresh Panjwani, MD, MSc, FRACGP Discoid lupus erythematosus is a chronic dermatological disease that can lead to scarring, hair loss, and hyperpigmentation changes in skin if it is not treated early and promptly. It has a prolonged course and can have a considerable effect on quality of life. Early recognition and treatment improves the prog- nosis. The diagnosis is usually made by clinical examination. In some cases histopathology may be re- quired to confirm the diagnosis. The histology is that of an inflammatory interface dermatosis. There is insufficient evidence for which treatment is most effective. Because lesions are induced or exacerbated by ultraviolet exposure, photoprotective measures are important. Potent topical steroids and antima- larials are the mainstay of treatment. Some cases of discoid lupus erythematosus can be refractory to standard therapy; in these cases retinoids, thalidomide, and topical tacrolimus offer alternatives, as do immunosuppressives like azathioprine, cyclosporine, mycophenolate mofetil, and methotrexate. (J Am Board Fam Med 2009;22:206–213.) Lupus erythematosus (LE) is thought to be an 5% of patients with discoid lupus may develop autoimmune disease among other connective tissue SLE1 and 25% of patients with SLE may develop diseases like scleroderma, rheumatoid arthritis, typical chronic discoid lesions at some time during copyright. -

Treatment Or Removal of Benign Skin Lesions
Treatment or Removal of Benign Skin Lesions Date of Origin: 10/26/2016 Last Review Date: 03/24/2021 Effective Date: 04/01/2021 Dates Reviewed: 10/2016, 10/2017, 10/2018, 04/2019, 10/2019, 01/2020, 03/2020, 03/2021 Developed By: Medical Necessity Criteria Committee I. Description Individuals may acquire a multitude of benign skin lesions over the course of a lifetime. Most benign skin lesions are diagnosed on the basis of clinical appearance and history. If the diagnosis of a lesion is uncertain, or if a lesion has exhibited unexpected changes in appearance or symptoms, a diagnostic procedure (eg, biopsy, excision) is indicated to confirm the diagnosis. The treatment of benign skin lesions consists of destruction or removal by any of a wide variety of techniques. The removal of a skin lesion can range from a simple biopsy, scraping or shaving of the lesion, to a radical excision that may heal on its own, be closed with sutures (stitches) or require reconstructive techniques involving skin grafts or flaps. Laser, cautery or liquid nitrogen may also be used to remove benign skin lesions. When it is uncertain as to whether or not a lesion is cancerous, excision and laboratory (microscopic) examination is usually necessary. II. Criteria: CWQI HCS-0184A Note: **If request is for treatment or removal of warts, medical necessity review is not required** A. Moda Health will cover the treatment and removal of 1 or more of the following benign skin lesions: a. Treatment or removal of actinic keratosis (pre-malignant skin lesions due to sun exposure) is considered medically necessary with 1 or more of the following procedures: i. -

Successful Treatment of Ulcerative and Diabeticorum
Letters 1. Picardi A, Pasquini P, Cattaruzza MS, et al. Psychosomatic factors in first- Another prevalent transverse linear crease of the face, the onset alopecia areata. Psychosomatics. 2003;44(5):374-381. nasal crease, appears across the lower third of the nasal dor- 2. Vannatta K, Gartstein MA, Zeller MH, Noll RB. Peer acceptance and social sum. In some cases, changes of pigmentation, milia, or pseudo- behavior during childhood and adolescence: how important are appearance, comedones are present along the nasal crease.5 Transverse na- athleticism, and academic competence? Int J Behav Dev. 2009;33(4): 303-311. sal milia in the absence of a transverse nasal crease are less frequently reported. Recently, our research team6 reported a OBSERVATION case of seborrheic keratosis–like hyperplasia and horn cysts aligned along this crease. These findings were attributed to the Deep Labiomental Fold With Pseudocomedones fact that the triangular cartilage and the alar cartilage attach The labiomental fold is a transverse indentation of the face, in a linear fashion at the junction of the middle and lower third which marks the intersection of the lower lip and chin.1 It plays of the nose, producing a potential embryonic fault line in which a significant role in movement of the lower lip and in facial ex- retention cysts presenting as milia and comedones can occur.5 pression. We describe herein a child with a linear pattern of Early acne lesions favor the forehead, nose, and chin in microcomedones located along a deep labiomental fold. many children. Although many times overlooked, the exter- nal ear is another common location for open and closed com- Report of a Case | A 7-year-old healthy girl presented with a line edones in young patients with acne.7 We think that the com- of black papules on her chin. -

Necrobiosis Lipoidica: a Histopathological and Histochemical Study* Howard R
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector THE JOURNAL OF INVESTIGATIVE DERMATOLOGY Vol. 44, No. 6 Copyright C 1965 by The Williams & Wilkins Co. Printed in U.S.A. NECROBIOSIS LIPOIDICA: A HISTOPATHOLOGICAL AND HISTOCHEMICAL STUDY* HOWARD R. GRAY, M.D., JAMES H. GRAHAM, M.D. AND WAINE C. JOHNSON, M.D. Urbach (1), in 1932, described necrobiosislipoidica diabeticorum and 17 biopsy specimens lipoidica diabeticorum as a complication offrom 14 patients with necrobiosis lipoidica were studied. Also, biopsy material from 25 consecutive diabetes nwllitus. Oppenheim (2)later inpatients with granuloma annulare was studied. 1932, reported another patient with diabetes Clinical data was obtained from clinical records, who had the same cutaneous involvement andquestionaires, personal interviews, and examina- used the term dermatitis atrophicans lipoidestion of the patient. All specimens were fixed in 10% neutral buffered formalin and most of the diabetica. Since then necrobiosis lipoidica dia-tissue was processed for routine paraffin-blocked beticorum has been generally the term used forsections. Multiple sections stained with hema- this skin disease associated with diabetes. Manytoxylin and eosin were examined from all patients. examples of necrobiosis lipoidica ot associatedSections of representative specimens from 5 pa- with diabetes have been reported (3—5) andtients each with necrobiosis lipoidica diaheticorum, necrobiosis lipoidica and granuloma annulare were the incidence of associated diabetes is variouslyprepared by the following methods: periodic reported from 25 to 87% (6—10). Necrobiosisacid-Schiff (PAS) reaction, with and without lipoidica diabeticorum occasionally precedesdiastase digestion; colloidal iron reaction (12), clinical evidence of diabetes (6, 9). -

Seborrheic Keratosis
Benign Epidermal and Dermal Tumors REAGAN ANDERSON, DO- PROGRAM DIRECTOR, COLORADO DERMATOLOGY INSTITUTE, RVU PGY3 RESIDENTS- JONATHAN BIELFIELD, GEORGE BRANT PGY2 RESIDENT- MICHELLE ELWAY Seborrheic Keratosis Common benign growth seen after third/fourth decade of life Ubiquitous among older individuals Tan to black, macular, papular, or verrucous lesion Occur everywhere except palms, soles, and mucous membranes Can simulate melanocytic neoplasms Pathogenesis: Sun exposure- Australian study found higher incidence in the head/neck Alteration in distribution of epidermal growth factors Somatic activating mutations in fibroblast growth factor receptor and phosphoinositide-3-kinase Seborrheic Keratosis Sign of Leser-Trelat: Rare cutaneous marker of internal malignancy • Gastric/colonic adenocarcinoma, breast carcinoma, and lymphoma m/c • Abrupt increase in number/size of SKs that can occur before, during, or after an internal malignancy is detected • 40% pruritus • M/C location is the back • Malignant acanthosis nigricans may also appear in 20% of patients • Should resolve when primary tumor is treated, and reappear with recurrence/mets Seborrheic Keratosis 6 Histologic types Acanthotic Hyperkeratotic Reticulated Irritated Clonal Melanoacanthoma Borst-Jadassohn phenomenon Well-demarcated nests of keratinocytes within the epidermis Seborrheic Keratoses Treatment Reassurance Irritated SKs (itching, catching on clothes, inflamed) Cryotherapy, curettage, shave excision Pulsed CO2, erbium:YAG lasers Electrodessication Flegel